
Abstract
Presenting episodes of intermittent viremia (EIV) under combination antiretroviral therapy (cART) is frequent, but there exists some controversy about their consequences. They have been described as inducing changes in immune responses potentially associated with a better control of HIV infection. Conversely, it has been suggested that EIV increases the risk of virological failure. A retrospective analysis of a prospective, randomized double-blinded placebo-controlled study was performed. Twenty-six successfully treated HIV-infected adults were randomized to receive an immunization schedule or placebo, and after 1 year of follow-up cART was discontinued. The influence of EIV on T cell subsets, HIV-1-specific T cell immune responses, and viral load rebound, and the risk of developing genotypic mutations were evaluated, taking into account the immunization received. Patients with EIV above 200 copies/ml under cART had a lower proportion of CD4+ and CD4+CD45RA+RO− T cells, a higher proportion of CD8+ and CD4+CD38+HLADR+ T cells, and higher HIV-specific CD8+ T cell responses compared to persistently undetectable patients. After cART interruption, patients with EIV presented a significantly higher viral rebound (p=0.007), associated with greater increases in HIV-specific lymphoproliferative responses and T cell populations with activation markers. When patients with EIV between 20 and 200 copies/ml were included, most of the differences disappeared. Patients who present EIV above 200 copies/ml showed a lower CD4+ T cell count and higher activation markers under cART. After treatment interruption, they showed greater specific immune responses against HIV, which did not prevent a higher virological rebound. EIV between 20 and 200 copies/ml did not have this deleterious effect.
Introduction
O
There exists some controversy about the real significance and consequences of EIV. It has been considered that it is both clinically irrelevant and could induce changes in immune responses, accelerate viral evolution, and jeopardize the long-term effectiveness of cART. On the one hand, patients with EIV present higher levels in both the magnitude and the breadth of total HIV-specific CD8+ and CD4+ T cell responses compared to persistently undetectable patients. 6 –9 These responses could help to control viral replication 8 and they would be associated with higher CD4+ T cell counts 4 without increasing the risk of virological failure. 1,3,4,10 –14 On the other hand, it has also been shown that EIV increases T cell activation and therefore facilitates the extension of HIV infection. 13,15,16 Moreover, EIV could be associated with the development of mutations that confer resistance to cART 10,14,15 and, therefore, to an increased risk of virological failure. 5,15 Finally, one observational study evaluated the influence of EIV in the control of viral replication after cART interruption, and found a higher viral rebound among patients who had EIV (“blippers”). 7
To explore the influence of EIV on T cell subsets, HIV-specific T cell responses, and viral rebound before and after discontinuing cART, we reanalyzed the data of a prospective study evaluating the influence of vaccination on VL rebound and immune responses, and where immunizations were not associated with an increase in detectable VL.
Materials and Methods
Study design
Data from a clinical trial evaluating the effect of a vaccination schedule in HIV-infected individuals was retrospectively analyzed. 17 Briefly, the trial was a prospective, randomized, double-blinded, placebo-controlled study performed at the Hospital Clínic of Barcelona, Spain, from April 2003 to July 2006. Twenty-six HIV-infected patients successfully treated under cART were randomized to receive during 12 months either a vaccination program or placebo. The vaccination program included seven different usually recommended vaccines against 10 different agents: hepatitis B (Engerix B, Smithkline bF1 Beecham SA; months 0, 1, 2, and 6), hepatitis A (Havrix 1440, Smithkline Beecham SA; months 4 and 10), influenza (2003–2004 WHO recommended vaccine [A/New Caledonia/20/99 (H1N1), A/Moscow/10/99 (H3N2), and B/Hong Kong/330/2001]; month 1), pneumococcus (Pneumo 23, Aventis Pasteur MSD SA; month 2), varicella (Varilrix, Smithkline Beecham SA; months 4 and 6), measles-mumps-rubella (Priorix, Smithkline Beecham SA; month 8), and tetanus-diphtheria (Ditanrix Adult, Smithkline Beecham SA; month 10). The placebo group received the same doses of placebo (0.5 ml of saline solution) at the same months. On month 12, cART was interrupted in both groups. Blood samples were taken monthly during treatment and after interruption. All patients provided written informed consent. The study was approved by the institutional ethics review boards and was registered in the public clinical trials database of the NIH (number NCT00329251). In that previous study we concluded that immunizations were not associated with an increase in EIV. Once the study was finished we retrospectively reclassified patients into patients with EIV (those who present at least one detectable VL during the cART period) and patients without EIV (those whose VL was persistently under the level of detectability).
Virological evaluations
Plasma HIV-1 RNA levels were determined using the Amplicor HIV-1 Monitor Ultra Sensitive Specimen Preparation Protocol Ultra Direct Assay (Roche Molecular Systems, Inc., Somerville, NJ) with a limit of quantification of 200 copies/ml. Samples below the detection limits were retested with a lower limit of detection of 20 copies/ml. Population-based genotypic resistance testing was performed during treatment every time VL rose over 1,000 copies/ml and with the first VL over 1,000 copies/ml after cART interruption, with use of the TruGene Assay (Visible Genetics).
Immunological evaluations
Several immunological parameters were evaluated in order to explore the influence of EIV on the immunological system, especially over the CD4+ and CD8+ T cell subsets and their response against HIV.
Different T cell subsets were determined as previously described using three-color flow cytometry. 18 Briefly, peripheral blood mononuclear cells (PBMCs) were obtained by separation on Ficoll Hypaque centrifugation gradient. Samples containing 105 cells were used for direct staining with different monoclonal antibodies (Becton Dickinson, Mountain View, CA). The stained cells were analyzed on a FacSCalibur (Becton Dickinson, San Jose, CA) flow cytometer. Data were analyzed using CellQuest software.
PBMC proliferation assays [lymphoproliferative responses (LPR)] were performed essentially as previously described. 19,20 Briefly, cells were cultured in the absence or presence of phytohemagluttinin (PHA) 0.5 and 1% 90 μg/ml (Murex, Biotech Ltd, England), OKT3 10 ng/ml (Ortho Biotech Inc., Raritan, NJ), anti-CD28 100 μg/ml, pokeweed mitogen 10 μg/ml (Sigma, St Louis, MO), Tetanus toxoid 2750 U, cytomegalovirus (CMV) antigen 10 μg/ml, and 5 μg/ml of HIV-1 antigens gp160 and p24 (Protein Sciences, Meriden, CT). Incorporation of tritium-labeled thymidine was assessed for the last 18 h of culture (Betaplate LKB Wallac, Sweden). Results were expressed as mean counts per minute (cpm). The stimulation index (SI) was calculated for each sample as cpm for cells with stimulus/cpm for cells without stimulus. A positive response to polyclonal stimulation was considered when the SI was greater than 15. Positive antigen-specific responses were defined as more than 3,000 cpm and an SI greater than 3.
An ELISpot assay (enzyme-linked immunospot assay) was used to measure HIV epitope-specific CD8+ T cell interferon-γ release from cryopreserved PBMC samples, as previously described. 21 –23 Briefly, PBMCs were plated in the presence of different HLA class I-restricted synthetic peptides from gag, pol, env, and nef proteins. Spot-forming cells (SFC) were counted using an AID ELISpot reader (Autoimmun Diagnostica GmHb, Germany). After subtracting background counts obtained with PBMCs and medium alone, results were normalized to SFC/106 PBMCs. A positive response was considered when counts were >40 SFC/106 PBMCs.
Statistical analysis
The analysis was done for two different limits of detectability: 200 and 20 copies/ml. Virological and immunological data were analyzed comparing both groups (patients with EIV vs. patients without EIV) taking into account the immunizations received. Continuous variables are reported as medians and interquartile ranges. Comparisons between groups were made by using the Mann–Whitney U test for continuous data and the χ2 or Fisher's exact test for qualitative data. Correlations were studied by using Spearman's rank correlation. Changes and durability in quantitative variables were analyzed by an area-under-the curve (AUC) measurement that incorporated the baseline value. Two-sided tests were considered significant when p<0.05.
Results
Clinical characteristics
The 26 patients included had a median age of 39 years (interquartile range 25–58). There were 21 men and 5 women, and their main risk factor for HIV infection was sexual contact (92%). With the assay with a limit of quantification of 200 copies/ml there were 10 patients with some detectable VL and 16 persistently undetectable. There were no significant differences between the detectable and undetectable group in clinical baseline characteristics (Table 1). Even the proportion of vaccinated and placebo patients was balanced (50% in each group). However, the undetectable group included all the women in the study and presented a higher proportion of patients treated with inhibitors or protease (IP).
These are expressed as the median and interquartile range for quantitative variables and the number of patients and percentage for categorical variables.
Fisher's exact test.
cART, combination antiretroviral therapy.
Differences in virological and immunological parameters during the cART period in patients with EIV above 200 copies/ml
Virological changes
There were 314 determinations of VL. Twenty-two of them were detectable above 200 copies/ml [incidence of 0.07 detectable VL/determination (95% CI 0.044–0.104)]. Of them, six were isolated episodes and the remaining 18 appeared in four clusters of consecutive determinations (from 2 to 6). The range of magnitude of detectable VL was 210–51,200 copies/ml, median 544.5 copies/ml (Fig. 1A). Seven of these determinations (31.8%) were related either to a discontinuation or a decrease in adherence to cART. We did not find other potential causes for the remaining EIV.

We did not find clinical relevant mutations associated with EIV. Only one patient presented an M184V mutation during treatment. It was associated with a high increase in VL (51,200 copies/ml), which the patient reported was due to a decrease in cART adherence to 75%. He was taking lamivudine, didanosine, and nelfinavir, and lamivudine was changed to tenofovir and the VL returned to undetectable levels after 1 month.
Changes in T cell subsets, LPR, and HIV-specific CD8+ T cell responses
At baseline and/or during treatment, patients with EIV above 200 copies/ml had a lower proportion of CD4+(p=0.047, 0.053, 0.012, and 0.055 in months 3, 6, 9, and 12, respectively) and CD4+CD45RA+RO− T cells and a higher proportion of CD8+ and CD4+CD38+HLADR+ T cells compared to persistently undetectable patients (Table 2). There were no differences in other T cell subsets, although at baseline a trend to lower CD8+CD38+ corrected after it was found.
These are expressed as the median and interquartile range.
Measured by stimulation index.
Measured by spot-forming cells/106 peripheral blood mononuclear cells (SFC/106 PBMCs).
p<0.05 for the comparison between groups in that month.
LPR, lymphoproliferative responses; PHA, phytohemagluttinin; CMV, cytomegalovirus.
There were no differences between groups in LPR to polyclonal mitogens or to recall and HIV antigens (Table 2).
The detectable group showed higher HIV-specific CD8+ T cell responses at baseline both in the magnitude of the responses [against gag peptides p1, p2, p6, and p7 (small pool) p=0.014, total gag peptides pool p=0.059; p17 p=0.085, total specific CD8+ T cell responses p=0.25] and in the breadth of responses (p=0.032 for the quotient between total specific CD8+ T cell responses and number of peptides). These differences were maintained and in some cases increased during treatment (Table 2).
Differences in virological and immunological parameters after cART interruption
Virological changes
Undetectable and detectable patients presented a significantly different evolution. Although viral rebound was present in both groups, it was higher in the detectable patients as defined by a higher peak VL (5.33 vs. 4.68 log10, p=0.022), a higher VL at month 14 (2 months after interruption) (4.85 vs. 4.08 log10, p=0.005), and a higher AUC of VL after interruption (13.51 vs. 9.57, p=0.007) (Fig. 1B). We did not find clinical relevant mutations.
Changes in T cell subsets, LPR, and HIV-specific CD8+ T cell responses
Some T cell subsets had a different evolution in the detectable and undetectable group, mainly in the initial period of interruption (months 12 to 14). CD4+ T cells dropped significantly more and sooner in the detectable group (p=0.026 for comparison of change between groups); meanwhile T cells with activation markers such as CD4+CD38+ and CD4+CD38+HLADR+ increased significantly more and sooner during the early phase of this period in these patients (p=0.038 and 0.007, respectively, for the comparison of change between groups), as well as CD8+CD38+ and CD8+CD38+HLADR+ (but not significantly). However, all these differences tended to disappear at month 18 (6 months after cART interruption) (Fig. 2 and Table 2).
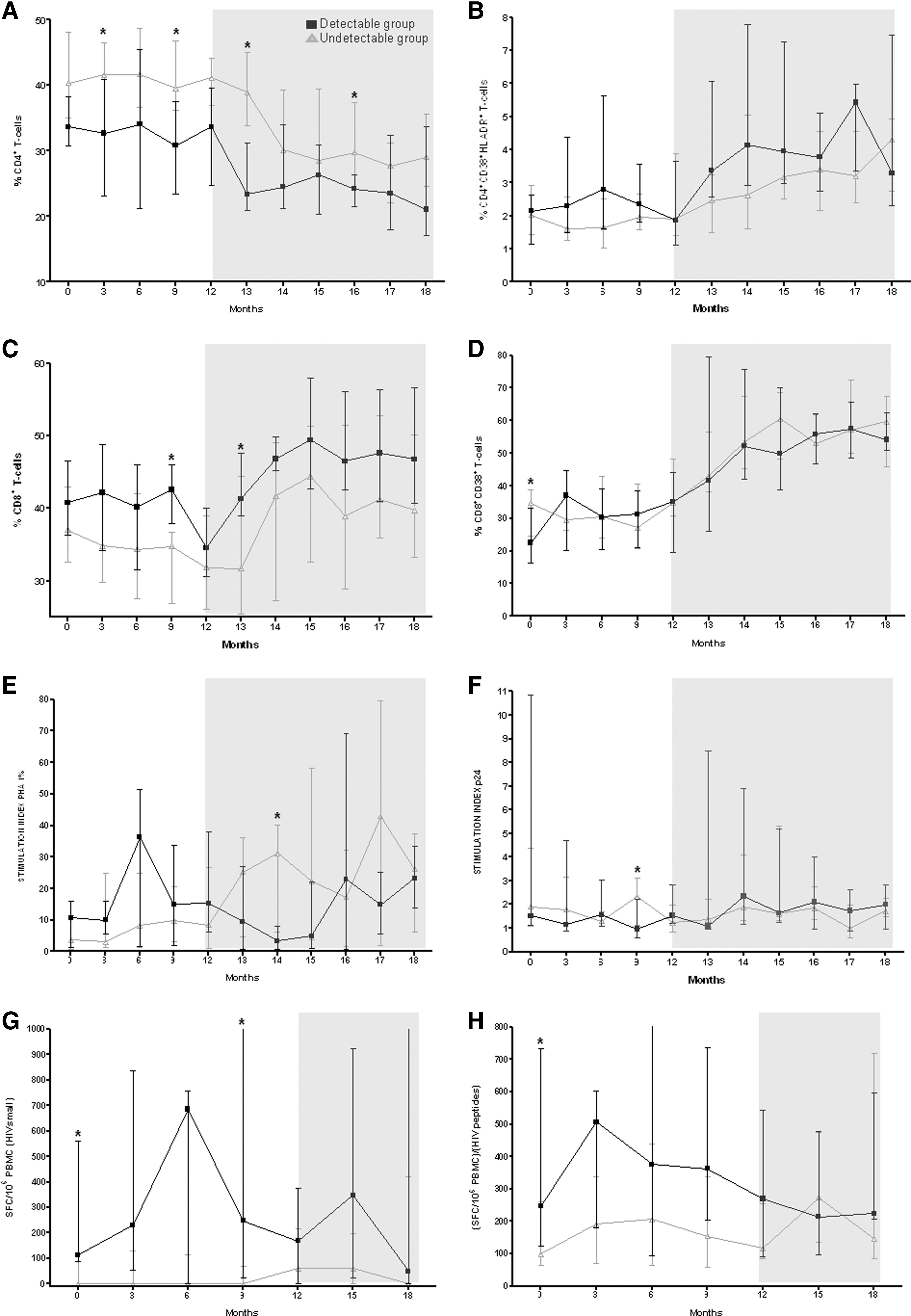
Evolution of immunological parameters during the study period. Months 0 to 12, patients were on cART. At month 12 cART was discontinued (shady area) [■ and black line, detectable (≥200 copies/ml) group; Δ and gray line, undetectable group].
LPR presented some differences between groups, mainly in the earlier period. The detectable group tended to present a greater increase in specific anti-HIV LPR responses, whereas LPR against polyclonal mitogens tended to increase more among the undetectable group. However, the differences were not significant (Fig. 2 and Table 2).
Finally, HIV-specific CD8+ T cell responses in undetectable patients presented a greater and earlier increase, tending to reach the level of response in the detectable group (p=0.045 for the differences among months 12 and 14 in the quotient of total responses and number of peptides) (Fig. 2 and Table 2).
Substudy with patients with EIV above 20 copies/ml
When samples with VL below 200 copies/ml (293 determinations) were reanalyzed with an assay with a limit of detection of 20 copies/ml, the total number of detectable VL increased to 49 determinations (incidence of 0.156, 95% CI 0.12–0.2), with a range of 21–51,200 copies/ml and a median of 210 copies/ml. Four new patients were then considered detectable (n=14).
All previous variables were reassessed in this new scenario. All women enrolled in the study (n=5) were persistently undetectable and 50% of each group had received the vaccination program. In addition to that, the nadir CD4+ T cell count was higher in the undetectable group (Table 1).
However, most of the differences that had been found previously between the detectable and undetectable group decreased and lost significance. Virological rebound, changes in T cell subsets, LPR responses, and HIV-specific CD8+ T cell responses, both during treatment and after its interruption, were more similar between groups (data not shown).
Discussion
Some studies have suggested that EIV did not have any influence on the virological and immunological outcome. 2,4,10,24 Conversely, other authors report that EIV could improve HIV-specific responses, positively influencing the clinical outcome in HIV-infected patients. 1,3,11 –14 We have analyzed the data from a comparative double-blinded placebo-controlled study from a schedule of different usually recommended vaccines in HIV-infected patients who had monthly blood sampling during 18 months (including 12 months on cART and 6 months of cART interruption) to further address this issue. 17 We have observed that patients with EIV above 200 copies/ml presented important virological and immunological differences (both during and after the interruption of cART) compared to persistently undetectable patients (<200 copies/ml). Patients with EIV have a worse CD4+ T cell count recovery, in parallel with an increased level of activation markers. These findings likely explain the higher rebound of viral load after cART interruption despite presenting a higher level of HIV-specific responses. Finally, it seems that EIV between 20 and 200 copies/ml did not have this deleterious effect.
The baseline clinical characteristics were similar between groups and we did not find differences in some aspects previously reported to be associated with the presence of EIV, such as age, 15 current cART regimen, 4,5,11 –13,24 and previous cART regimen. 1,2,5,11,12,15,25 We did not find a clear cause of the EIV in 68.2% of the cases, as opposed to other previous publications in which 75.8% of patients did present a detectable cause. 15 In fact, although EIV had previously been identified as markers of low adherence, it has been demonstrated that this statement was wrong, 11,13,24 except for greater increases in VL. 11 It is noteworthy that 50% of patients in each group received vaccinations, and that three cases of EIV (13.6%) were preceded by a vaccination, but not the remaining 22.
Detectable patients showed immunological differences under cART compared to previously described undetectable patients. They had less CD4+ T cells 13,15,16 and an increase in CD4+CD38+HLADR+ T cells. 16 After cART discontinuation, we also found that the detectable group presented a higher viral rebound, similar to the only previous work that explored this issue. 7 These data support the hypothesis that a high level of immune activation (and not the absolute number of CD4+ T cells) is the force that fuels viral replication.
These findings could have two possible explanations (or a combination of them). On the one hand, patients who present EIV can shelter a more aggressive virus, with a higher replication capacity. This would induce EIV, and then, due to higher replication and activation, a CD4+ T cells loss, an increase in cells with activation markers, and a higher viral rebound. Previous findings of an association between EIV and pre-cART VL or the time needed to reach undetectability, as well as the reduction in number of EIV with intensification strategies, support this hypothesis. 1,15,26 –28 On the other hand, detectable patients could have a less efficient immune system in some of the antiviral mechanisms (cellular or humoral, specific or not) due to either a genetic predisposition or to greater devastation induced by HIV previous to the initiation of cART. Therefore, immunological findings will be the cause and not the consequence of EIV. Studies that have demonstrated an association between a higher incidence of EIV and a lower CD4+ T cell count before initiating cART support this idea. 12,26,28
Detectable patients showed higher HIV-specific CD8+ T cell responses under cART, as previously described. 6,7,9 Although it has been hypothesized that these responses would help to control viral replication, 8,29 –31 we have demonstrated in one previous work 7 that these patients presented a higher viral rebound after cART discontinuation. This apparent paradox could be explained by the existence of parallel dysfunctions in innate immune responses, 32,33 clonal depletion, 34 or impaired CD8+ T cell function. 35 Another possible explanation is the absence of differences in LPR responses specific against HIV that we have found (which have also been described as being increased in detectable patients 6,7,9 in other works). It is probable that the increase in HIV-specific responses seen in detectable patients, both CD4+ and CD8+, was more a consequence of more antigen availability than a strategy of the immune system to improve viral control.
Our findings could have important clinical applications. If a patient presents with an EIV over 200 copies/ml despite having a good adherence to cART, this could be a marker of “worse outcome” and a predictor of failure. Although there is controversy about the association between EIV and virological failure, 1,3,4,10 –14,36,37 this is probably because virological suppression induced by current treatments is potent enough to limit the consequences of these EIV in the short-term. But it is possible that in longer time periods detectable patients finally presented some differences in outcome, as we have found that their immunological responses are different. Larger prospective studies are needed to confirm this issue, and to determine if there is a higher risk of clinical events in patients with EIV (i.e., non-AIDS-associated events such as a higher risk of cancer, cardiovascular events, or neurological disorders); optimization or cART in order to reduce EIV or complementary treatments to control its consequences (higher level of immune activation) would be required. 38
Interestingly, when patients were reclassified with a lower limit of detectability (20 copies/ml), we found that most immunological and virological differences between detectable and undetectable patients decreased and disappeared. Two interpretations of this finding are possible. On the one hand, it is possible that some of the EIV over 20, but not over 200 copies/ml, are the result of technique or biological variability and therefore they do not reflect a “real” increase in VL. Some studies have demonstrated that repeated analysis of the same sample can show variations to 40%, 24,39 –41 in particular when VL is low or depending on the assay used. 42,43 On the other hand, some patients presented several low level EIV, which is contrary to a random variation. 44 Thus, another possible explanation is that patients who present with very low-level EIV are the ones who will really benefit from a controlled virus exposition, large enough to increase specific responses, but small enough to avoid the deleterious effects of activation and increase of replication. In any case, there were only four patients, which limits every hypothesis that could be made about this.
Therefore different levels of EIV could have different implications, depending mainly on their magnitude and number of consecutive determinations. Those around the current limit of detection of 50 copies/ml and that occur only once may not be predictors of future failure 45 and could even have some positive effect. Conversely, a higher EIV, especially over 200 copies/ml, will be deleterious. A previous study suggested a significant increase in risk of virological failure in patients whose EIV is over 120 copies/ml. 37
This study has several limitations. First, the most important is the sample size, which could be too small to find differences in some variables. Second, patients included in our study were in a “preserved” immune status because of inclusion criteria. This could influence the incidence of EIV and therefore the changes they induce. Also, this is a retrospective analysis of data from a clinical trial designed to evaluate the effect of a vaccination schedule on HIV immunological responses and EIV. However, we previously demonstrated that EIV was not associated with such vaccinations, vaccinated and placebo patients were balanced between detectable and undetectable patients, and the immunizations received are those currently prescribed for the HIV population. We employed an assay with a limit of quantification of 200 copies/ml because it was the one used in the clinical routine when the trial was done. Viral load targets have evolved over the years, dropping to the current goal of <50 copies/ml. 46 However, we continue to see patients with EIV>200 copies/ml in clinical practice, and the results found in this study are also valid for them. Finally, the follow-up time is short as we have analyzed EIV only during the 12 months under cART.
In conclusion, patients who present with an EIV above 200 copies/ml had a lower CD4+ T cell count and higher activation markers under cART. After treatment interruption, they showed higher specific immune responses against HIV that did not prevent a higher virological rebound. It seems that an EIV level between 20 and 200 copies/ml does not have this deleterious effect.
Footnotes
Acknowledgments
This study was supported in part by grants ISCIII-RETIC RD06/006, FIPSE 36536/05, SAF 05/05566, FIS PI050058, FIT 090100-2005-9, FIS PI050265, FIS 04/0503, and FIS 07/0291. Dr. Felipe García was a recipient of a research grant from IDIBAPS, Barcelona, Spain. Dr. Montserrat Plana is a researcher from the Institut d'Investigacions Biomèdiques August Pi I Sunyer (IDIBAPS) and is supported by the ISCIII (Instituto de Salud Carlos III) and the Health Department of the Catalan Government (Generalitat de Catalunya).
FIPSE is a nonprofit foundation including the Spanish Ministry of Health, Abbott Laboratories, Boehringer Ingelheim, Bristol Myers Squibb, GlaxoSmithKline, Merck Sharp and Dohme, and Roche.
FIS is the Red Temática Cooperativa de Grupos de Investigación en Sida del Fondo de Investigación Sanitaria.
Part of the information contained in this article has been previously presented at the 13th Conference on Retroviruses and Opportunistic Infections (February 2006, Denver, Colorado).
Author Disclosure Statement
No competing financial interests exist.