
Abstract
Behavioral interventions have been shown to both promote and change many health-related behaviors and issues. This meta-analysis was performed to assess whether behavioral interventions have the potential to increase condom use and HIV testing uptake among men who have sex with men (MSM) in China. PubMed, Elsevier Science Direct, Chinese Biomedical Literature Database (CBM), China National Knowledge Infrastructure (CNKI), and Wanfang (Chinese) were searched to June 2011 to identify relevant articles. Data of eligible citations were extracted by two reviewers. Sixteen studies were identified. Aggregated findings indicated that interventions were associated with a significant increase in condom use between MSM and male sex partners in the last anal sex act (RR=1.17, 95% CI=1.05–1.29) and consistent condom use between MSM and male sex partners in the past 6 months (RR=1.36, 95% CI=1.15–1.60) and HIV testing (RR=2.22, 95% CI=1.72–2.88). However, no significant increase was detected in condom use over the course of the intervention among MSM engaging in sex with women. In the subgroup analyses, the positive effects were not detected in some subgroups such as anal sex with casual partners and intervention interval less than or equal to 6 months. The sensitivity analysis showed that these estimates were unchanged after removal of the study that had the biggest sample or the studies that had the most rigorous study design. This meta-analysis can inform future intervention design and implementation in terms of sample size, target populations, settings, goals for process measures, and intervention interval.
Introduction
I
Behavioral interventions that effectively produce reductions in risky sexual behavior and promote maintenance for safer sexual practice remain an important tool in fighting HIV. In a recent systematic review of behavioral interventions on HIV/AIDS in China, of 25 studies we identified, most have been concentrated in South and Southwest China. All studies reported positive intervention effects including improved HIV-related knowledge, increased condom use, and reduced needle sharing. But the existing interventions have primarily concentrated on injection drug users and female sex workers, with limited data regarding MSM. 8 In a Cochrane review, 58 interventions among MSM were summarized. These were included in 44 studies of 18,585 participants, but none of these studies was conducted in China. Another recent review of the effectiveness of social marketing interventions on HIV testing uptake among MSM included only three pretest–posttest design studies and found that multimedia social marketing campaigns had a significant impact on HIV testing uptake. However, this review was limited by the small number of studies included and poor study design. 9,10 Numerous interventions targeting risk reduction among MSM have been conducted in recent years, and because of the wide diversity of methodologies, interventions, and findings, it is important to conduct ongoing systematic reviews of the empiric literature to attain an integrated understanding of effective intervention components and to make evidence-based recommendations. 10
Even though remarkable progress in China's response to the HIV/AIDS epidemic has been made in the past decade, to date, there is no meta-analytic review of the published studies on HIV/AIDS intervention among MSM in China. At the critical moment when the global HIV/AIDS epidemic levels off while China's HIV/AIDS epidemic keeps growing, it is important to review the existing HIV/AIDS intervention efforts and make recommendations for future research. Accordingly, this study systematically reviews the literature on HIV/AIDS intervention studies among MSM in China with the following objectives: (1) to synthesize the published literature on HIV intervention studies among MSM in China; (2) to compare and summarize the key components of the intervention studies, including type of sexual partner, intervention interval, sample size, design, and intervention outcomes; and (3) to identify gaps in the existing literature and make recommendations for future research.
Materials and Methods
Search strategy and selection criteria
We searched PubMed, Elsevier Science Direct, the Cochrane Library, Chinese Biomedical Literature Database (CBM), China National Knowledge Infrastructure (CNKI), and Wanfang (Chinese) for relevant reports from January 1, 1990 to June 30, 2012. The following key words were used for searching: (“AIDS” or “HIV”) and (“prevention” or “control” or “intervention”) and (“homosexuality” or “bisexuality” or “gay” or “bisexual” or “MSM” or “men who have sex with men”). We placed no language restrictions on the searches or search results. Additional strategies included hand searches of journals not indexed in the electronic source, web-based searches, and screening of reference lists of retrieved studies for further potentially relevant articles. We collected data only from full published papers, not meetings or conference abstracts. Two investigators (M. Wang and L. Fu) searched the electronic databases independently, using the same methodology. The abstracts were reviewed independently by two investigators to determine whether they met the criteria for inclusion. References in the studies were reviewed to identify additional studies. If discrepancies occurred, a third investigator (C. Tu) performed an additional assessment. All studies that evaluated the effectiveness of behavioral interventions to reduce the risk of HIV transmission were assessed carefully with regard to the following criteria for inclusion in the meta-analysis: (1) studies conducted in China; (2) randomized controlled trials (RCTs) or controlled clinical trials (CCTs) that compared behavioral interventions with a control; and (3) pretest–posttest design studies (controlled or uncontrolled), i.e., studies in which outcome measurement data were collected before and after the intervention, to assess the effect of behavioral intervention on no intervention or control. Posttest-only studies and studies that combined prepost data were excluded. Interventions that targeted the general public but did not include MSM or did not have outcome data for MSM were excluded
We excluded studies that contained overlapping data. When there were multiple publications from the same population, only the one with the larger sample size was included. When a study reported the results from different subpopulations, we treated them independently.
Data extraction
We developed and modified a data abstraction form after a training exercise for investigators. We abstracted data on study details (e.g., randomization of cluster of participants, setting, duration of intervention, type of intervention), characteristics of participants (e.g., mean age, proportion who were male), outcomes assessed, and study results (e.g., condom use in the last anal sex with a man at baseline and the end of the intervention for the control and intervention groups). Types of behavioral intervention include HIV voluntary counseling and testing (VCT) and social and behavioral support (such as peer education, assertiveness and relationship support, discussing attitudes and beliefs, videos). Small group and community interventions include group counseling or workshops, interventions in community areas, training community leaders, and community-building empowerment activities. We excluded interventions that focused not on sexual transmission but on cognitive or affective outcomes such as distress associated with HIV testing or health and coping for seropositive men. We also excluded pharmaceutical interventions. Sex partners were categorized as female sexual partners or male sexual partners. Female sexual partners and male sexual partners were categorized as main or casual partners, respectively. A main partner was someone with whom the participant felt most committed (e.g., boyfriend, spouse, significant other, or life partner). A casual partner was someone with whom the participant did not feel committed, who he did not know very well, or with whom he had sex in exchange for something such as money or drugs. Two investigators (Y. Fang and Z. Huang) extracted the data independently using a standard protocol, and the results were reviewed by a third investigator (C. Tu). We contacted authors of the studies included to obtain further information for data items that needed clarification. The Cochrane EEOC method was used to assess the risk of bias in individual studies. Discrepancies were resolved by discussion with other term members (M. Wang, L. Fu, and J. Hao) or contract with original investigators, who were all sent data extraction sheets with requests for correction.
Statistical analysis
The Cochrane Collaboration Review Manager 4.2 (Cochrane Collaboration,
Publication bias was investigated with the funnel plot, in which the standard error of log OR for each study was plotted against its OR (odds ratio). Funnel plot asymmetry was assessed further using Egger's linear regression test. 15 If there is asymmetry, the regression line will not run through the origin; the intercept α provides a measure of asymmetry. The larger its deviation from zero, the more pronounced the asymmetry. The analyses were performed using the software Stata version 10 (StataCorp LP, College Station, TX). All p-values were two-sided. A p-value less than 0.05 was considered to be statistically significant.
To test the robustness of the main results, we conducted sensitivity analyses; we repeated the meta-analysis after removing the study by Zeng and colleagues that had the biggest sample and the study by Lau and colleagues and Hao and colleagues that had a more rigorous study design (i.e., a randomized controlled study). 16 –18
Results
Characteristics of eligible studies
There were 952 papers potentially relevant to the search terms (PubMed: 280; Elsevier Science Direct: 456; Cochrane Library: 0; CBM: 51; CNKI: 124; Wanfang: 41). The study selection process is shown in Fig. 1. There were 436 potentially relevant studies after duplicates were removed. During the screening of the abstracts, 415 of these articles were excluded (28 were review articles; 375 were not conducted in China; 12 had no control group). This left 21 studies for full publication review; of these, five were excluded (four for multiple publications from the same population and one due to no available data).
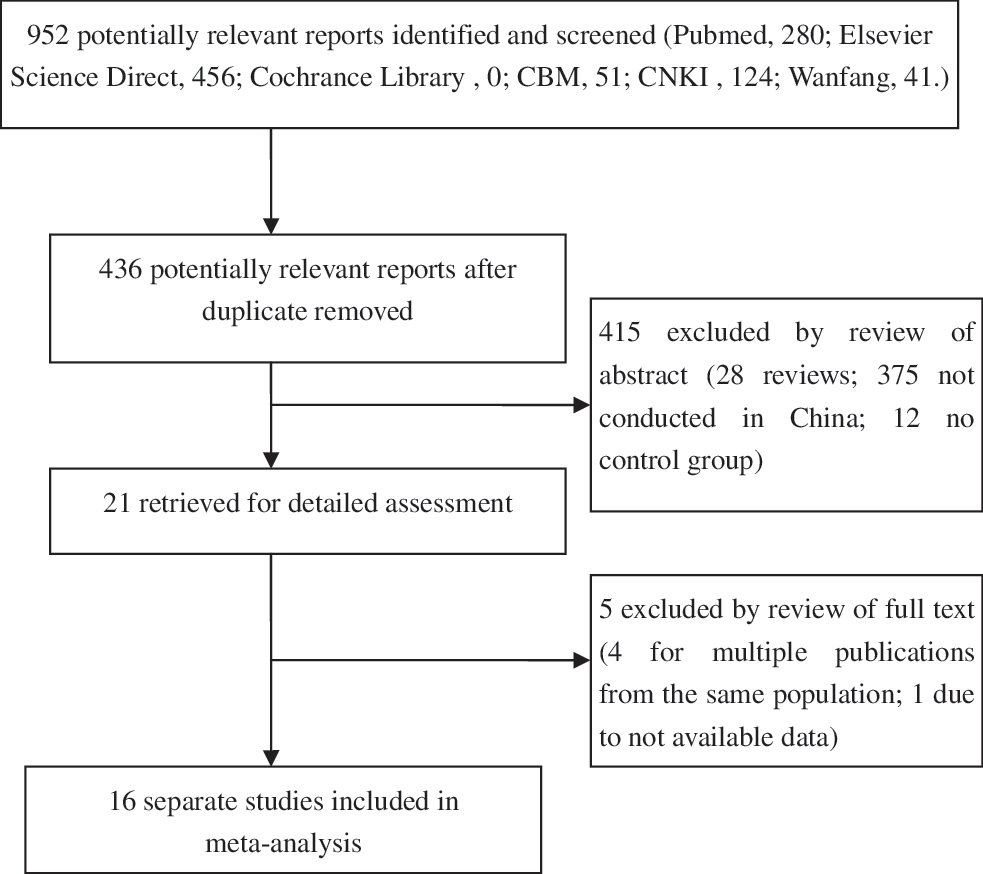
Flow diagram for selecting a study for meta-analysis.
There were 16 studies in the meta-analysis, and the characteristics of the included studies are presented in Table 1. 16 –31 The included studies appeared between 2007 and 2011. On average, samples were 25.58±8.12 years old. Most studies (93.75%) were conducted on the Chinese Inland (it is frequently used in the context of areas ruled by the People's Republic of China, referring to people from mainland China as opposed to other areas controlled by the state such as Hong Kong or Macau), with the majority (81.25%) of these studies conducted in medium to large cities.
A, condom use in the last anal sex with a man; B, consistent condom use when having anal sex with men in the past 6 months; C, condom use in the last sex with a woman; D, consistent condom use when having sex with women in the past 6 months; E, HIV testing.
VCT, voluntary conseling and testing.
The majority of studies (75%) used a pretest and posttest design. The present analyses used measures taken at the first follow-up, which occurred at a mean of 10.13±1.47 months from the intervention. The randomized controlled study design was used only in the study conducted in Hong Kong by J.T. Lau and colleagues and in Nanjing by Hao and colleagues. 17,18
Overall effects
The Q-test of heterogeneity was almost always significant and we conducted analyses using random effect models except in evaluating the effect on condom use in the last sex with woman and consistent condom use when having sex with women in the past 6 months in the overall population.
As Table 2 depicts, these analyses indicated that, overall, interventions were associated with a significant increase in condom use between MSM and male sex partners in the last anal sex act (RR=1.17, 95% CI=1.05–1.29) and consistent condom use between MSM and male sex partners in the past 6 months (RR=1.36, 95% CI=1.15–1.60) and HIV testing (RR=2.22, 95% CI=1.72–2.88). However, no significant increase was detected in condom use over the course of the intervention among MSM engaging in sex with women.
A, condom use in the last anal sex with a man; B, consistent condom use when having anal sex with men in the past 6 months; C, condom use in the last sex with a woman; D, consistent condom use when having sex with women in the past 6 months; E, HIV testing.
Results of analyses stratified by types of sexual partners
Behavioral interventions were associated with a significant increase in condom use in the last anal sex act (RR=1.20, 95% CI=1.04–1.38) and consistent condom in the past 6 months (RR=1.97, 95% CI=1.10–3.52) between MSM and regular sexual partners. When we examined the effects on condom use in the last anal sex act and consistent condom in the past 6 months between MSM and causal sexual partners, the differences were not detected.
Results of analyses stratified by intervention interval
Interventions were associated with a significant increase in condom use between MSM and male sex partners in the last anal sex act (RR=1.15, 95% CI=1.00–1.31) and consistent condom use between MSM and male sex partners in the past 6 months (RR=1.39, 95% CI=1.16–1.66) when the intervention interval was more than 6 months. However, we did not detect significant intervention effects on these two outcomes when the intervention interval was less than or equal to 6 months.
Interventions did increase HIV testing in both the following subgroups: intervention interval less than or equal to 6 months (RR=1.85, 95% CI=1.11–3.10) and intervention interval more than 6 months(RR=2.33, 95% CI=1.18–2.51).
Results of analyses stratified by sample size
Interventions were associated with a significant increase in condom use between MSM and male sex partners in the last anal sex act (RR=1.29, 95% CI=1.02–1.62) when the sample size was less than or equal to 200. However, we did not detect significant intervention effects when the sample size was more than 200.
Interventions can significantly increase consistent condom use between MSM and male sex partners in the past 6 months when the sample size was less than or equal to 200 (RR=1.77, 95% CI=1.08–2.91); the RR was smaller but still significant when the sample size was more than 200 (RR=1.28, 95% CI=1.06–1.55).
We found similar result when we examined whether the behavioral intervention impacted HIV testing stratified by sample size. Aggregated findings indicated that interventions did increase HIV testing among MSM, but the RR was smaller when the sample size was less than or equal to 200 (RR=2.53, 95% CI=1.65–3.87) compared to when the sample size was more than 200 (RR=1.93, 95% CI=1.24–3.01).
Results of analyses stratified by published in different country
We performed subgroup analyses stratified by published in a different country only concerning the outcome of consistent condom use when having anal sex with men in the past 6 months. Interventions can significantly increase consistent condom use between MSM and male sex partners in the past 6 months when the study was not published in a Chinese journal (RR=2.37, 95% CI=1.07–5.27) and when the study was published in a Chinese journal (RR=1.28, 95% CI=1.07–1.52).
Evaluation of publication bias
We assessed funnel plot asymmetry using Egger's linear regression test. The results are shown in Table 3. There was no publication bias in any of the analyses.
A, condom use in the last anal sex with a man; B, consistent condom use when having anal sex with men in the past 6 months; C, condom use in the last sex with a woman; D, consistent condom use when having sex with women in the past 6 months; E, HIV testing.
Discussion
This is the first meta-analysis, to our knowledge, to evaluate the effect of behavior interventions to reduce risk of HIV transmission among MSM in China, and a total of 12 pretest–posttest design studies and two randomized controlled studies and two quasiexperimental design studies were included. Our meta-analysis confirmed that behavior interventions were effective in promoting HIV testing and increased condom use when having anal sex with male sexual partners but had no effect on condom use when having sex with female sexual partners among MSM in China. The positive effects were not detected in some subgroups such as anal sex with casual partners and intervention interval less than or equal to 6 months. The behavior interventions had a protective, but not statistically significant effect on condom use among MSM with casual partners. It is possible that we were unable to detect statistically significant intervention effects on these outcomes due to higher condom use with casual male sex partners at baseline. Studies have shown that condom use among MSM is less likely with regular partners than with casual partners at baseline; it was more likely to assess a positive effect of the intervention among MSM with regular partners, while it was less likely among MSM with casual partners. 32 –34
This meta-analytic review suggests that interventions were successful at improving condom use in the “long term” (more than 6 months), but not the “short term” (less than 6 months). One possible explanation is that lack of time was the reasons why participants did not change their practices after intervention. 35,36 This explanation is based on theories of social learning and habit, central and peripheral routes to persuasion, and the influence of descriptive and prescriptive social norms and social support. People who are likely to change in the short term are called “innovators” and “early adopters.” In contrast, those who are slow to change are called “late adopters” and those unlikely to change are called “laggards.” So innovators and early adopters may be convinced by rational arguments, have a social network that supports change, and some self-efficacy to try the new practice before accepting or rejecting it. In contrast, late adopters may not adopt a new practice or product quickly because it requires some cognitive effort and social support to recall the message in the right context, to inhibit the old habit, and to initiate the new one. Late adopters may therefore not change until they see a critical mass of others in the community adopting the innovation. 37
The more common HIV intervention items among MSM in China have largely consisted of distributing condoms and educational materials through MSM volunteers and often in MSM social venues (bars frequented by MSM, bathhouses, parks, and public restrooms) and HIV VCT provided by the Center for Disease Prevention and Control. 21 One study reported that the intervention content items associated with the greatest effectiveness among community-level interventions were personal skills, self-reinforcement for behavior change, behavioral self-management, and longer follow-up times. 9 Another meta-analysis concluded that those interventions targeting higher risk groups, promoting interpersonal skills, focusing on younger MSM, and being delivered at the community level were more likely than other programs to be effective. 38 Our meta-analysis concluded that those interventions with a longer intervention interval (more than 6 months) and focusing on men who have sex with a regular male sexual partner were more likely to promote intervention effectiveness. An interesting finding in our meta-analysis was that sample size cannot be considered in the future designs because they are less effective on interventions. Furthermore, MSM has become a rapidly growing group in the HIV epidemic in China and they are at high risk of HIV infection and contribute to the spread of HIV to women and the general population, 39 so we should pay more attention to MSM who often have sex with women in future intervention designs among MSM in China.
Several specific details of this meta-analysis merit consideration. First, even though most of the studies were concentrated in the areas with a high HIV prevalence such as Guangdong, Guangxi, Sichuan, Yunnan, and Anhui, the existing literature suggests a geographic concentration that may not appropriately reflect the geographic variation of the HIV/AIDS epidemic in China. For example, Xinjiang is a region with the highest HIV infection rate compared to other regions, but no study was reported. Furthermore, no study was reported from Beijing, Shanghai, and Guangzhou, the three largest metropolitan areas with the highest MSM population in China. There was also a lack of data from northern China, northwest China, and northeast China. As the HIV virus has spread in all 31 provinces in China, future HIV/AIDS interventions need to be conducted in more diverse locations and multiple sites to reflect the wide geographic variations of the epidemic in China.
Second, the majority of the studies employed weak study designs (i.e., pretest–posttest design), thus producing a low quality of evidence. However, only four studies had a more rigorous study design (i.e., a randomized controlled study or quasiexperimental design). In community-based HIV prevention intervention, it is a challenge to conduct rigorous RCTs. A challenge is that MSM is a stigmatized, hidden population in all areas of the world and is a population difficult to access, and therefore many surveys rely on convenience sampling. The social stigma associated with an HIV diagnosis, as well as with identification as a gay man, and the resulting potential for discrimination generate a reluctance to access testing, treatment, or sources of information on prevention. Fear of discovery may mainly contribute to barriers to accessing prevention information and materials. 40 Another challenge is that there is a limited training and research capacity to conduct field-based (particularly community-based) HIV prevention interventions in China. As several experts pointed out, a lack of professional personnel, particularly at local levels, is one of greatest challenges in conducting HIV prevention interventions in China. Therefore, capacity-building in conducting field-based HIV behavioral interventions needs to be prioritized in China's national agenda of HIV/AIDS epidemic control. 41,42
Third, there are limitations in outcome measurement. Only a small number of the existing studies employed biomarkers (current HIV or STI infectious status) as outcome measurements while the majority relied on self-report behavioral outcomes (e.g., condom use, HIV testing). Self-reported data are subject to many potential biases including recall errors or socially desirable responses. Future intervention studies should complement self-reported behavioral measures with more objective biological outcomes (HIV prevalence or incidence) in predictions of intervention efficacy and to collect information on partner selection. In addition, because direct methods of assessing sexual behavior are unethical and impractical, future intervention evaluations are advised to consider using new technology (e.g., computer-assisted assessments) to improve the validity of self-reported sexual behavior.
Conclusions
MSM constitute a population that is highly susceptible to the rapid spreading of HIV in recent years. Our study shows that behavioral interventions can effectively increase HIV testing and condom use among MSM when they are having sex with male sexual partners, but the efficacy of condom use is limited when they are having sex with female sexual partners. However, the positive effects were not detected in some subgroups such as groups having anal sex with casual partners and groups in which the intervention interval is less than or equal to 6 months. Our findings imply that the general female population, as regular partners of MSM, has a high risk of contracting HIV that is bridged from their bisexual male partners. This meta-analysis is hampered by methodological weaknesses and the short time period for follow-up in all studies reviewed. To begin to address these gaps in the evidence, high-quality epidemiological research is needed that focuses specifically on all target populations and longer intervention intervals.
Footnotes
Acknowledgments
The authors would like to thank all for their valuable contributions to this article.
Author Disclosure Statement
No competing financial interests exist.