
Abstract
Slovenia is a small European country with a total of 547 HIV-infected individuals cumulatively reported by the end of 2011. However, the estimated incidence rate of HIV infections increased from 7.0 per million in 2003 to 26.8 per million in 2011. In this study, we assessed the prevalence of transmitted drug resistance (TDR) in the past 6 years (2005–2010) and analyzed the time trend of the proportion of men having sex with men (MSM) and HIV-1 subtype B among newly diagnosed individuals in a 15-year period (1996–2010) in Slovenia. Among 150 patients included in the study, representing 63% of HIV-1 newly diagnosed patients in 2005–2010, TDR was found in seven patients (4.7%). The prevalence of TDR to nucleoside reverse transcriptase inhibitors, nonnucleoside reverse transcriptase inhibitors, and protease inhibitors was 2% (3/150), 2% (3/150), and 0.7% (1/150), respectively. The majority of patients were infected with subtype B (134/150, 89%), while subtype A was detected in 6.0% (9/150), subtype D in 1.3% (2/150), and subtype G and CRF02_AG in 0.7% (one patient each). Three of 150 sequences could not be typed. Infection with subtype B was found to be significantly associated with male gender, Slovenia being reported as the country of the patient's nationality and origin of the virus, CDC class A, mode of transmission with homosexual/bisexual contact, sex with an anonymous person, and a higher CD4+ count. Among patients carrying the subtype B virus, an MSM transmission route was reported in 87% of patients. Although the prevalence of TDR in Slovenia is still below the European average, active surveillance should be continued, especially among MSM, the most vulnerable population for HIV-1 infection in this part of Europe.
S
The majority of HIV infections in Slovenia can be attributed to subtype B. A retrospective study conducted in 2006 on a cohort of 88% (131 of 149) of the total number of individuals diagnosed with HIV infection in the period between 1996 and 2005 showed a predominance of subtype B (110 of 131 patients, 84%), particularly among the MSM risk group (84 of 110, 76%). 4 Analysis of HIV-1 transmission networks among individuals infected with subtype B in Slovenia showed significant phylogenetic clusters comprised mostly of MSM patients, suggesting that subtype B infection among MSM is the main reason for epidemics in the country. 5
Transmission of HIV-1 drug-resistant virus among individuals (transmitted drug resistance, TDR) may reduce the efficacy of initial and/or subsequent drug regimens. 6 Genotypic resistance testing of the earliest clinical sample in all treatment-naive HIV-infected patients is suggested as the standard of care by the European Recommendations for the Clinical Use of HIV Drug Resistance Testing: 2011 Update. The European HIV Drug Resistance Guidelines Panel acknowledged the diversity in the implementation of drug resistance testing in treatment-naive patients across Europe and concluded that resistance testing is cost-effective when levels of TDR are >1–5%. 6 The prevalence of TDR in Slovenia was first analyzed by Babič et al. 5 in a study that included 87% of newly diagnosed individuals in Slovenia in the period 2000–2004. The estimated prevalence of TDR was 3.9% (3 of 77 patients) and the detected mutations conferred resistance to nucleoside reverse transcriptase inhibitors (NRTI) only. 7 The SPREAD Programme reported that the overall prevalence of TDR for 20 European countries and Israel for the period from September 2002 to December 2005 was 8.4%. There was no time trend of overall TDR, but a statistically significant decrease in protease inhibitor (PI) resistance and in nonnucleoside reverse transcriptase inhibitor (NNRTI) resistance was observed, indicating that TDR is stabilizing in Europe. 8 Since the prevalence of TDR identified in Slovenia was lower than in other European countries, routine genotypic resistance testing in all newly diagnosed individuals was not implemented, except in selected patient groups (e.g., pregnant women, patients known to be infected abroad).
The primary aim of this study was to assess the prevalence of TDR in the past 6 years (2005–2010) and to evaluate the need for implementation of routine genotypic resistance testing of newly diagnosed treatment-naive HIV-infected individuals in Slovenia. Additionally, the epidemiological time trend of the proportion of MSM and subtype B among newly diagnosed HIV-infected individuals in Slovenia was evaluated for a 15-year period (1996–2010).
A total of 239 individuals were diagnosed with HIV-1/AIDS at the Slovenian AIDS Reference Center in the period from 2005 to 2010. Epidemiological (age, nationality, route of infection, etc.) and clinical (CD4+ T cell count, HIV-1 viral load, coinfection status, CDC class, etc.) data for each newly diagnosed HIV-infected individual are routinely collected by clinicians in the form of a blinded questionnaire, approved by the Medical Ethics Committee at the Ministry of Health of Slovenia (Approval Ref. No.: 126/12/03). The inclusion criteria for the study of TDR in the period from 2005 to 2010 were treatment-naive patients, available questionnaire, and at least 400 μl of the patient's plasma sample taken within 3 months after diagnosis. The part of the study analyzing the epidemiological time trend of HIV-1 infection in Slovenia (particularly in the context of the MSM risk group and subtype B infections) included, in addition to the patients mentioned above, HIV-infected patients diagnosed at the Reference Center in the period 1996–2005 with documented information on the most probable mode of HIV-1 acquisition and on HIV-1 subtype.
For sequencing samples of patients diagnosed prior to 2006, the ViroSeq HIV-1 Genotyping System version 2 (Celera Diagnostics, Alameda, CA) was used, following the manufacturer's instructions. Alternatively, HIV-1 RNA was extracted from 400 μl of a patient's plasma sample using an EZ1 Virus 2.0 kit in the BioRobot EZ1 system (Qiagen, Hilden, Germany) and amplified using the SuperScript III One-Step RT-PCR System with Platinum Taq High Fidelity (Invitrogen, Carlsbad, CA). If a PCR product of insufficient quantity was obtained, nested PCR was performed using AmpliTaq Gold DNA polymerase (Applied Biosystems, Foster City, CA). For the PCR and sequencing reactions primers were used as reported elsewhere, spanning the entire protease gene and 1–253 amino acids of the reverse transcriptase gene. 9 Amplicons were purified with the addition of enzymes Exonuclease I and Shrimp Alkaline Phosphatase (Thermo Fisher Scientific, Waltham, MA) and subjected to direct sequencing using a BigDye Terminator v3.1 Cycle Sequencing Kit (Applied Biosystems) with four primers giving bidirectional sequences. A DyeEx 2.0 Spin Kit (Qiagen) was used according to the manufacturer's instructions for the removal of unincorporated dye terminators from the sequencing reactions and obtained sequences were assembled using Vector NTI Advance v 11.0 (Invitrogen, Carlsbad, CA).
The presence of resistance mutations in the studied sequences was determined according to the surveillance drug resistance mutation (SDRM) list, updated in 2009 and subtyped by using the REGA HIV-1 Automated Subtyping Tool, version 2.
10
–12
The clinical significance of SDRM for the virological response to antiretroviral treatment was evaluated by using the Stanford University HIV Drug Resistance Database, Genotypic Resistance Interpretation Algorithm version 6.1.1 (
For statistical analysis, the on-line statistical package Epi Info Version 3.5.3 was employed (
Among randomly selected samples, 150 pol sequences were successfully obtained, representing an overall 63% coverage of all newly diagnosed patients during the years 2005–2010 in Slovenia. Selected demographic, epidemiological, and clinical data of the patients included in the TDR analysis are presented in Table 1. The majority of the enrolled patients were males (133 of 150, 89%) from the MSM risk group (120 of 150, 80%) reporting sex with an anonymous person as the most probable mode of HIV acquisition (90 of 150, 61%).
For significance testing, the Fisher exact test was employed for categorical data and t-statistics for continuous data.
Proportion among all newly diagnosed HIV-1 patients in the period 2005–2010 in Slovenia.
Defined as having an HIV-1-negative test result within 12 months prior to the first reactive HIV-1 result or having laboratory evidence of seroconversion within a sample (having only a fourth generation HIV assay reactive or having undetermined/negative Western blot and/or immunoblot).
SD, standard deviation; CDC, Centers for Disease Control and Prevention; SDRMs, surveillance for drug resistance mutations.
Mutations associated with TDR (SDRMs) were found in seven of 150 patients (4.7%). SDRMs associated with NRTI and NNRTI resistance were found in three patients each (2.0%) and PI resistance in one patient (0.7%). SDRMs associated with resistance are listed in Table 2. All patients with SDRMs were males from the MSM risk group who had reported sex with an anonymous person as the most probable mode of HIV-1 acquisition. Two of seven patients with SDRMs identified Slovenia as the probable country of infection (Table 2).
SDRMs, surveillance for drug resistance mutations; NRTI, nucleoside reverse transcriptase inhibitors; NNRTI, nonnucleoside reverse transcriptase inhibitors; PI, protease inhibitors; NA, not assigned; ABC, abacavir; 3TC, lamivudine; LPV/r, lopinavir/ritonavir; EFV, efavirenz; DRV/r, darunavir/ritonavir; TDF, tenofovir; FTC, emtricitabine.
The clinical significance of detected mutations for the treatment response in patients with SDRMs was evaluated by using the Stanford algorithm. Highly active antiretroviral therapy (HAART) was initiated in all patients with SDRMs, prior to the TDR analysis, and a potential low level or low level resistance to one or two drugs used in the initial regimen in four of seven patients with SDRMs was predicted by the Stanford algorithm. High level resistance to efavirenz was predicted for one patient with a K103N mutation. All patients with SDRMs achieved a complete virological response to the selected combination of drugs (Table 2). Despite the initial virological response to the combination of efavirenz, abacavir, and lamivudine in the patient with a K103N mutation, the patient's drug regimen was changed to a combination of abacavir, lamivudine, darunavir, and ritonavir after the results of the primary resistance became available (virological success to the second-line treatment was also achieved). The first-line regimen in patient 1 was changed due to adherence problems and, despite predicted intermediate resistance to efavirenz, the patient achieved a sustained virological response to the second-line regimen. No significant differences were observed between the characteristics of patients with SDRMs and patients without SDRMs, probably due to the small sample size.
The majority of HIV-infected individuals analyzed in the period 2005–2010 were infected with subtype B (134/150, 89%); subtype A was detected in 6.0% (9/150), subtype D in 1.3% (2/150), and subtype G and CRF02_AG in 0.7% (one patient each). Three of 150 sequences could not be typed by the REGA bioinformatics tool. Subtype B infection was significantly associated with male gender, Slovenian nationality, CDC class A, mode of transmission with homosexual/bisexual contact, sex with an anonymous person, Slovenia as origin of the virus, and a higher CD4+ count (Table 1).
For the subtype time trend analysis of HIV infection in Slovenia for the period 1996–2010, a total of 255 patients were studied, or 69% of 370 newly diagnosed HIV-1 patients in the 15-year period. Subtype B was detected in 219 of 255 (86%) patients. The remaining subtypes were subtype A in 14 of 255 patients (5.5%), CRF02_AG in eight of 255 (3.1%), D in three of 255 (1.2%), CRF01_AE in two of 255 (0.8%), and F1 and G in a single patient each (0.4%). HIV subtypes in seven of 255 (2.7%) patients remained unassigned, possibly due to a recombination event happening in the past. A total of 180 of 184 (97.8%) MSM patients enrolled in this part of the study were infected with subtype B, while the remaining four were untypable by REGA. In contrast to this finding, 29 of 36 (81%) patients infected with non-B subtypes belonged to the heterosexual group. The time trend for the proportion of MSM among all newly diagnosed HIV-1 patients in Slovenia and of the proportion of MSM and subtype B among observed patients in this study over the years 1996 through 2010 is shown in Fig. 1. A decrease in subtype B infections was recorded in 2009, due to more infections attributable to subtype A, with a 12.5% prevalence in 2009 (5/40 patients diagnosed in 2009 and included in the study, three of them originating from the Ukraine and the remaining two from Bosnia and Herzegovina; data not shown). The time trend analysis for the period 1996–2010 also showed an increase in MSM infections, mostly with subtype B virus, among newly diagnosed HIV-infected individuals in the country.
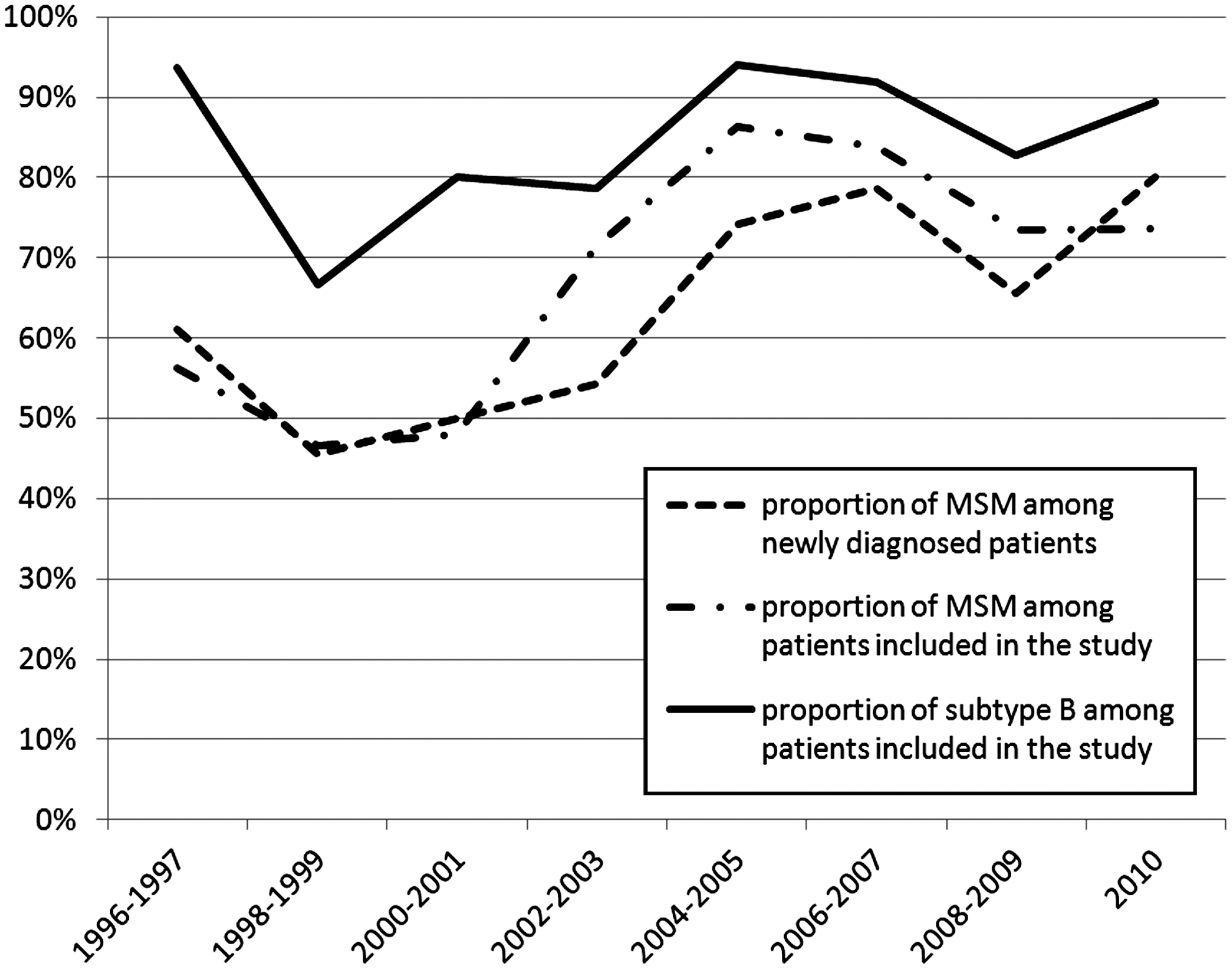
Concomitant time trend in the proportion of men who have sex with men (MSM) and subtype B among HIV-1 infections over the 15-year period (1996–2010) in Slovenia.
The results of studies on the prevalence of TDR from different countries/regions are often not directly comparable, due to major differences in the studied populations, geographic regions, national coverage, sampling strategies, and algorithms used to score mutations relevant for TDR. The prevalence of TDR in Slovenia reported in this study (2005–2010) is comparable to the results obtained in the previous period 2000–2004 (4.7% vs. 3.9%; p>0.99), despite the use of different algorithms for the identification of mutations relevant for TDR in the two Slovenian studies (International AIDS Society-USA vs. WHO recommended algorithm). The comparability of the data is reinforced by the very high national coverage of newly diagnosed treatment-naive HIV-infected individuals achieved in both studies (87% for the period 2000–2004 and 63% for the period 2005–2010). 7 To the best of our knowledge, both studies report data with the largest national coverage for TDR analysis published to date.
Analysis of TDR according to separate classes of antiretroviral drugs has shown, for the first time, TDR to NNRTI and PI among newly diagnosed treatment-naive individuals in Slovenia (2005–2010). TDR in the period 2000–2004 remained restricted to NRTI. 7 These results show important changes in the pattern of TDR in Slovenia in the period 2005–2010, supporting the idea that continuous surveillance of TDR on a national level is essential. Furthermore, both Slovenian studies provided evidence of the continuous transmission of drug-resistant HIV-1 in Slovenia for the past 10 years, suggesting the need to reevaluate the national strategy on resistance testing in newly diagnosed treatment-naive patients. 7 Importantly, the prevalence of TDR in Slovenia is above the 1% minimum threshold for the cost-effectiveness of this diagnostic approach, based on the most recent European recommendations. 6
Vercrauteren et al. 8 reported an 8.4% prevalence of TDR in newly diagnosed patients (n=2793 patients) from European Union countries and Israel (SPREAD programme) for the period 2002–2006. The prevalence of TDR in Slovenia for the period 2005–2010 is significantly lower than that reported for the SPREAD programme. The prevalence of SDRM associated with both NRTI and PI resistance in Slovenia is also lower than that shown by the results of the SPREAD study (2% vs. 4.7% and 0.7% vs. 2.9%, respectively). 8
Studies on the prevalence of TDR in newly diagnosed treatment-naive HIV-infected individuals from neighboring countries (Italy, Austria, Hungary, and Croatia) are diverse in terms of national coverage, study design, and interpretation algorithms. The prevalence of TDR in Italy was monitored as a part of a CASCADE study (119 seroconverters, 1992–2003) and SPREAD study (271 newly diagnosed treatment-naive individuals, 2002–2005). 13 The prevalence of TDR reported in both the CASCADE study (15.1%) and the Italian part of the SPREAD study (12.2%) was higher than the Slovenian data. 13 Similar to these findings, a recent study among newly diagnosed patients from Croatia for the period 2006–2008 also showed a significantly higher prevalence of TDR (21.6%, Grgić et al., unpublished data) compared to Slovenian data. Mezei et al. 14 reported a 16.6% prevalence of TDR in a study on 30 treatment-naive HIV-infected MSM from Hungary. To the best of our knowledge, data on the TDR prevalence in Austria on a national level are not available. The consistently higher prevalence of TDR among newly diagnosed treatment-naive HIV-infected patients from neighboring countries further emphasizes the need for continuous surveillance of TDR in Slovenia.
A MSM transmission route and infection with subtype B were shown to be statistically significant predictors of TDR in the SPREAD study. 8 Although no statistically significant difference was found in our study (probably due to the small sample size), all patients with TDR were males from the MSM risk group reporting sex with an anonymous person and infected with subtype B virus (six of seven patients), similar to the results of the SPREAD data. 8
The molecular epidemiology of HIV-1 in the Balkan Peninsula has been recently reviewed by Stanojević et al. 15 This showed a high diversity in the distribution of HIV-1 subtypes and major transmission routes among countries. With an 84% fraction of subtype B infection, Slovenia clearly belongs to countries with the highest prevalence of subtype B in Central and Southeastern Europe (Hungary, Croatia, Serbia, and Montenegro). Remarkably, all but one MSM from Slovenia diagnosed between 1996 and 2005 (84/85) were infected with subtype B. 4,15 The analysis of HIV-1 subtype distribution among individuals included in the analysis of TDR in the period 2005–2010 confirms our previous observation of a very high prevalence of subtype B infections (89%), particularly among MSM, since all but three of 120 patients with a reported MSM transmission route (98%) were infected with subtype B virus.
Transmission clusters, particularly of MSM individuals, play an important role in the spread of HIV-1, particularly in closed populations. 16,17 A study on transmission patterns of HIV-1 infection in Slovenia showed that transmission of HIV-1 in this country is probably driven by recently infected individuals, who were present in the majority of clusters. 5 A similar observation was made in the SPREAD study, suggesting that resistant HIV-1 strains are further transmitted primarily from untreated individuals. 8
The increase in the incidence of HIV-1 infection in Slovenia over the past decade can be attributed almost exclusively to an increase in newly diagnosed patients from the MSM group (the annual reported rate of newly diagnosed HIV-1 cases among MSM in 1999 of 2.5 per million increased to 17.0 in 2011). 1,2 An increase in unsafe sexual behavior among MSM in Slovenia has recently been reported, indicated by recent reports of an increased number of syphilis diagnoses (two out of three reported early syphilis cases in 2008 among MSM were from HIV-infected individuals). 3 This is in accordance with our data showing that 17% of newly diagnosed HIV-1 patients had syphilis and that all of them reported MSM as the transmission route.
In conclusion, this study showed that 4.7% of treatment-naive individuals from Slovenia diagnosed with HIV infection in the period 2005–2010 were infected with the virus carrying SDRMs. TDR to all three major classes of antiretroviral drugs (NRTI, NNRTI, and PI) was identified. The increased overall prevalence of TDR, as well as the appearance of SDRMs associated with NNRTI and PI resistance in recent years, emphasizes the need for continuous surveillance of TDR in Slovenia (particularly among MSM infected with subtype B virus) and reevaluation of the national strategy on resistance testing in newly diagnosed treatment-naive patients. This study also showed the urgent need to promote HIV prevention programs directed at MSM individuals, who are most affected by the HIV-1 epidemic in Slovenia and may substantially contribute to the spread of resistant virus in the near future.
Sequence Data
GenBank accession numbers for the reported sequences are GQ398934, GQ399003, GQ399157, GQ399167, GQ399210, GQ399318, GQ399406, GQ399433, GQ399494, GQ399553, GQ399574, GQ399677, GQ399709, GQ399721, GQ399731, GQ399787, GQ399882, GQ399950, GQ399979, GQ400015, GQ400033, GQ400039, GQ400057, GQ400283, GQ400355, GQ400410, GQ400411, GQ400442, GQ400452, GQ400472, JX028303–JX28406, and JX046402–JX046417.
Footnotes
Acknowledgments
The research leading to these results received funding from the European Community's Seventh Framework Programme (FP7/2007–2013) under the project “Collaborative HIV and Anti-HIV Drug Resistance Network (CHAIN),” grant 223131. The authors would like to thank Janez Stare (Ljubljana) for help with statistical analysis.
Author Disclosure Statement
No competing financial interests exist.