
Abstract
This study aimed to estimate HIV incidence among women at higher HIV risk in Addis Ababa, Ethiopia using cross-sectional data. To refine the estimate, we sought to determine a local correction factor by estimating a false recent rate for the BED assay. The overall study had two parallel phases: cross-sectional incidence and BED false recent (BED FR). A total of 1856 women at higher HIV risk were enrolled into the cross-sectional phase. For the BED FR, 500 women and 70 men with known HIV infection of greater than 12 months were enrolled. Rapid HIV tests were used to assess participant HIV status. Samples from women with positive results on HIV rapid testing were then analyzed using the BED assay to determine incident HIV infections. The overall HIV prevalence was 11.3%, with women greater than 25 years old having a higher prevalence (26.5% vs. 7.9% for younger women). The overall unadjusted HIV incidence was 3.3%. The estimated HIV incidence was 2.6% when adjusted using the locally derived false recent rate of 3.5%. Similar incidence rates were found between the younger and older age groups. This is one of the first field-based studies of HIV incidence in Ethiopia; it demonstrates that there is sufficient incidence to warrant further HIV prevention efforts among women at higher risk of HIV infection.
Introduction
HIV/AIDS
HIV prevention trials have reported promising results for trials of male circumcision, topical microbicides, and oral preexposure prophylaxis. 3 –7 Studies of these and other prevention modalities require research sites with properly trained staff, experience in clinical research, linkages with the surrounding community, the ability to enroll substantial numbers of study participants, and a substantial HIV incidence rate. Several international programs have spurred the preparation of new clinical research sites, including the FHI 360 Site Identification and Development Initiative (SIDI).
We conducted a cross-sectional study, utilizing the BED assay, to estimate the HIV incidence among women at higher risk of HIV infection in Addis Ababa, Ethiopia and to prepare a new clinical research site for future studies. Specifically, the conduct of this study served as site preparation, while the HIV incidence estimates both informed future prevention programs as well as demonstrated the suitability of the site for future HIV prevention trials. To further characterize the study site and cohort, we also measured participant accrual, summarized their basic demographic features, and measured contraceptive use and the pregnancy prevalence.
Materials and Methods
Study site and recruitment
This study was conducted at the Armauer Hansen Research Institute (AHRI) in Addis Ababa, which is part of the Federal Ministry of Health and contributes to Ethiopia's national HIV research program. AHRI is the research arm of the ALERT Hospital (the full name of ALERT Hospital is All Africa Leprosy Rehabilitation and Training Center, although it is widely known only as ALERT), which provides a wide range of services to the local population, including voluntary counseling and testing (VCT) and antiretroviral therapy (ART).
Participants were recruited in collaboration with a local NGO, HAPSCO, that works with the surrounding community. An initial community mapping phase identified venues where people meet potential sexual partners 8,9 and provided locations from which we could recruit initial participants. A peer-driven methodology 10 was used to recruit women from these risky venues, whereby women noted as potentially eligible and interested in participating in a research study were given a coupon that invited them to the AHRI site. After an initial wave of 100 participants was recruited, a peer-driven recruitment process was implemented in which eligible women were provided up to three additional coupons to be given to female friends whom they thought might be eligible and interested.
Cross-sectional study procedures
Women arriving at the clinic for the study first completed the informed consent process and received a participant number. Women were screened for eligibility after providing consent. Eligible women were between the ages of 18 and 35 years at the time of screening, of unknown HIV status, and at higher risk of sexual acquisition of HIV, as indicated by reporting two heterosexual sex acts per week over the past 1 month, or having two or more different sexual partners in the previous 1 month. During the interview to determine eligibility, baseline demographic, medical and sexual behavior information was collected for each participant. Eligible women were then administered HIV and pregnancy tests. Women who complained of sexually transmitted infection (STI) signs and/or symptoms received syndromic treatment per national guidelines.
We drew approximately 15 ml of blood via venipuncture for HIV testing and specimen storage. The national HIV testing guidelines require at least two positive HIV rapid tests to confirm HIV-positive status. We conducted parallel testing using two HIV rapid tests (Abbott Determine HIV-1/2 and Trinity Biotech Capillus HIV-1/HIV-2), unlike the serial testing prescribed in the national algorithm. If the results were discrepant, a third rapid test (Trinity Biotech Unigold) was administered as a tie-breaker. Pretest and posttest counseling was provided for each participant. HIV-positive participants were referred for follow-up counseling and care.
Pregnancy testing was done using “One Step RapiDiphCGInstaTest Urine” (Cortez Diagnostics). Both the pregnancy and HIV testing were done in accordance with manufacturer's instructions. Results of the HIV and pregnancy tests were provided to the participant during her visit.
BED false recent study procedures
We estimated the number of incident (recent) HIV infections in the cross-sectional cohort with the BED EIA HIV-1 incidence assay (Calypte). The commercially available BED-CEIA assay tends to overestimate incidence estimates when compared with prospective studies done in the same population, 11,12 because it falsely classifies some persons with long-term infection as recently infected.
The BED False Recent study was conducted to measure the false-recent (FR) rate in the same area and at the same time as the cross-sectional study. We recruited women and men at ALERT Hospital and other local treatment centers who were 18–35 years of age, had documented HIV-positive status for at least 12 months, and had no history of ART.
Written informed consent was administered, followed by an interview to collect demographic, medical, and sexual histories. Duration of HIV-infected status and never-use of ART were confirmed by medical record review. Once the interview and medical record check was complete, approximately 15 ml of blood was drawn via venipuncture. BED test results were not provided to the participants since it was done for research purposes only and is not diagnostic.
Ethical considerations
The protocols, informed consent forms, and any participant educational or informational items were reviewed and approved by the FHI 360 ethics committee, the AHRI ethics committee, and the National Ethical Review Board in Ethiopia prior to study start.
The informed consent form was read to each volunteer verbatim prior to enrollment and data collection. Consents were available in both Amharic and English. Witnesses were utilized for low-literate and illiterate participants.
Statistical analysis
All enrolled participants were included in the cross-sectional analysis. We summarized participant's sociodemographic characteristics, self-reported STI symptoms, and HIV risk behaviors by calculating the mean and standard deviations. We calculated baseline prevalence of HIV infection and pregnancy, along with 95% confidence intervals (CI). We used multiple logistic regression to evaluate the association between baseline factors and prevalent HIV infection, indicated by odds ratio (OR) estimates.
The unadjusted HIV incidence estimation by BED testing was calculated using the formula provided in the assay's package insert as
where w is the window period for detecting recent infections (assumed to equal 197 days regardless of clade or population 13 ), N inc is the number of incident (recent) infections identified by BED among participants with a positive rapid test, and N neg is the number of HIV-negative individuals. The CI of the incidence rate was calculated based on the assumption that the number of incident infections follows a Poisson distribution.
The BED false recent rate in the BED FR study was computed as the total number of BED recent test results divided by the total number of participants with confirmed longer-term HIV infection. We calculated the BED false recent adjusted HIV incidence estimate using Hargrove's formula and Welte's adjustment. 11,14
Results
Study enrollment
A total of 1,856 women were eligible and enrolled in the cross-sectional phase of the study with 1,855 undergoing HIV testing. Women enrolled in this phase came from all regions of the country; the majority were born in Amhara, Oromiya, or Southern Nations, Nationalities, and People's Region (SNNP). Most resided in several subcities on the west side of Addis Ababa (Fig. 1). The study site was located within the subcity of Kolfe-Keranyo, where a majority of the women also resided. For the BED false recent phase a total of 570 participants were eligible and enrolled; 500 women were enrolled and 500 were tested, and 70 men were enrolled with 68 tested.
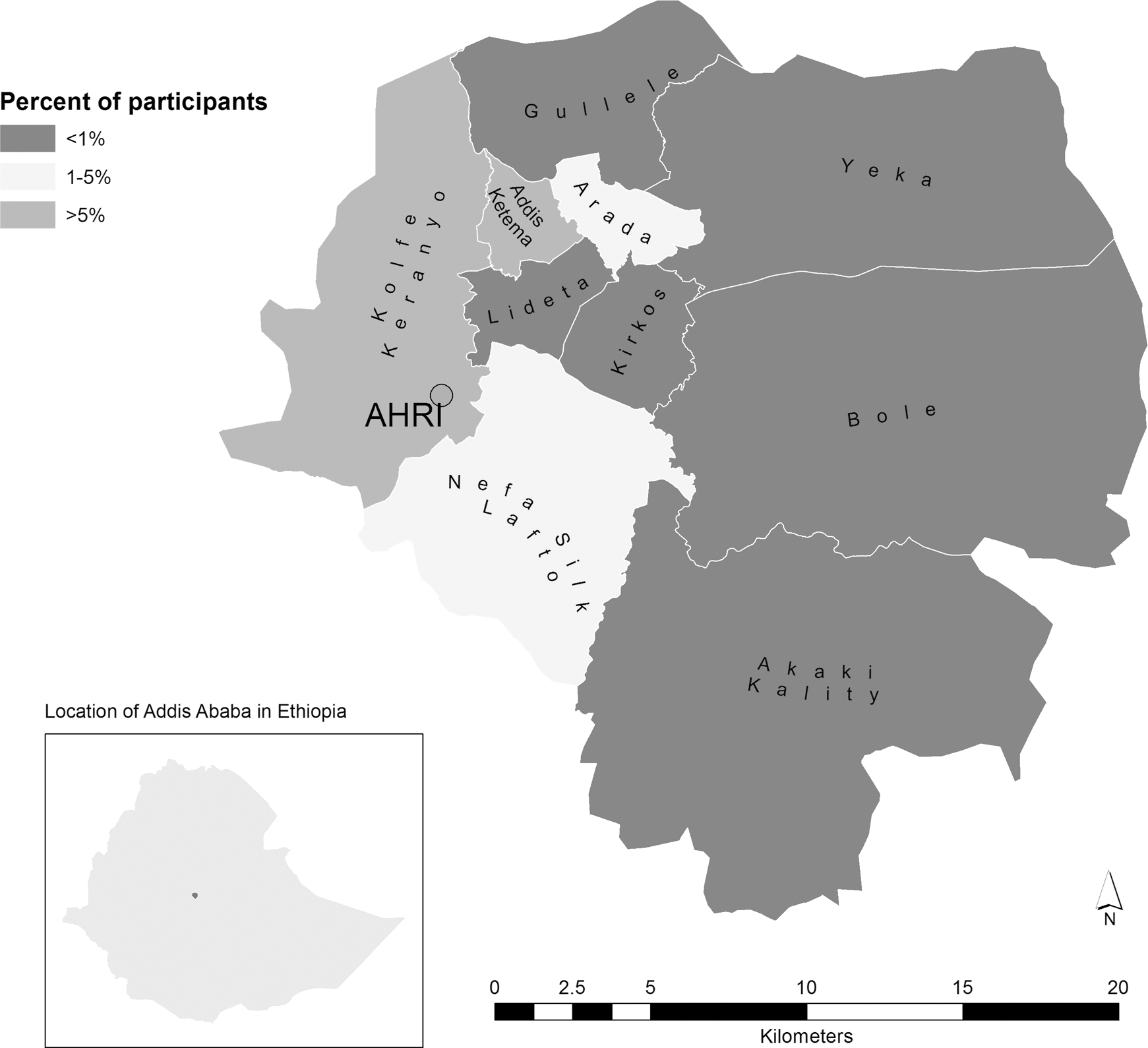
Participant residence by subcity in Addis Ababa.
Participant demographic characteristics
The majority (71%) of women enrolled in the cross-sectional phase were young (<23 years old) with low educational attainment (Table 1). Their average length of residence in Addis Ababa was 11.1 years. Of the women 94.5% self-identified as sex workers, with>5 sex partners in the last month, including many new partners. Over 95% of the women used some form of contraception, with injectables (42%), condoms (35%), and orals (14%) predominating.
At the time of the study, US$1=ETB 11.
IDU, intravenous drug user.
In contrast, participants in the BED false recent phase were older with more education (Table 1). Their sexual risk profile was entirely different: 57% had had no sex partners in the last month, and a similar percentage (56%) did not use contraception.
HIV prevalence
The overall HIV prevalence among cross-sectional participants was 11.3% (95% CI 9.9, 12.8). The HIV prevalence was significantly higher among women 25 years or older [26.5% (21.3, 30.8)] versus 7.9% (6.5, 9.2) among younger women (p<0.001; Table 2). Women were significantly less likely to use a condom when having vaginal sex with their primary partners versus other partners (p=0.014) (Table 2). In multiple logistic regression, three factors were significantly associated with prevalent HIV infection: being older (>24 years old) (OR 4.4; 3.3, 5.9), the presence of STI symptoms (OR=2.4; 1.6, 3.6), and having vaginal sex without a condom in the past 7 days (OR=1.5; 1.0, 2.1).
Approximate Chi-square test.
Fisher's exact test.
Mean (median).
p-value for comparing median using Wilcoxon rank-sum test.
p-value for difference of mean proportion.
IDU, intravenous drug user; MSM, men who have sex with men.
HIV incidence
In the cross-sectional phase, there were 29 (14%) recent infections out of 206 BED tested samples, and the unadjusted incidence estimate was 3.3% (95% CI 2.1, 4.5). In the BED false recent study, the false-positive rate was 3.2% (1.7, 4.7) among the female participants [3.8% (2.3, 5.5) overall]. Using the false recent rate among women, the Hargrove adjusted incidence estimate was 2.7% (1.7, 3.7) and the Welte estimate was 2.6% (1.4, 3.8) (Table 3). The Hargrove adjusted incidences were 3.7% (2.1, 5.3) among women aged 18–20 years, 0.2% (0.0, 0.6) in those aged 21–24, and 3.3% (0.8, 6.9) among women aged 25–35. There were few recent infections in the latter two age strata.
Using female FRR only as the most relevant adjustment for our female cohort [of the 500 women tested, 16 (3.2%) showed as falsely recent].
CI, confidence interval.
Pregnancy prevalence
The pregnancy prevalence in the cross-sectional study was 5.9% (4.9, 7.1). Pregnancies occurred predominantly among women using condoms as their only method of family planning (pregnancy prevalence 9.5%). Women using injectable contraceptives had the lowest pregnancy prevalence (1.9%) and women using oral contraceptives had a pregnancy prevalence of 3.7%.
Discussion
The substantial HIV prevalence among these higher-risk women in Addis Ababa, Ethiopia is not unexpected. A large proportion of participants in the cross-sectional study reside in the area immediately around the ALERT hospital and the city's major market area, zones of the city with large populations of young migrants from rural areas. Typically, these women have relocated to Addis Ababa with the hopes of finding work as a house maid or nanny. Many, however, fail to find employment and revert to sex work for survival. We recruited initial participants from a variety of nearby venues including “arakibets” (informal liquor establishments) and hotels, where sex work is common, and then utilized their social networks to enroll more women into the study.
Within this predominantly sex worker population in Addis Ababa, we found an overall HIV prevalence of 11.3%, which was higher (26.5%) among those over 25 years of age, reflecting their longer exposure time. In a recent meta-analysis of HIV prevalence among female sex workers across Africa, Asia, Eastern Europe, Latin America, and the Middle East, Baral et al. 15 found an overall pooled prevalence of 11.8%, which was highest in sub-Saharan African cohorts, although they did not include any data from Ethiopia. The pooled odds of HIV infection among female sex workers was 13.5 times that of all women of reproductive age in the corresponding areas.
Directly measured HIV prevalence and incidence data from Ethiopia are scarce. The available data indicate that the HIV epidemic appears to be stabilizing in Ethiopia. Various sources report prevalence rates around 18% and incidence rates estimated around 8% in the late 1990s, whereas post-2000 data indicate slightly lower prevalences around 14% prevalence with 2% annual incidence (range 0.7–3.3). 16
Our study found a similar high prevalence among 25- to 35-year-old women as the 2011 report from the Federal Ministry of Health (FMOH). 2 This is unsurprising given the longer exposure opportunity for older women. The similarity in estimated incidence rates among the younger and older women is unexpected, however, as most HIV studies demonstrate higher rates in younger age strata. 17 We did have a disproportionately high number of young women in the study between the ages of 18 and 22 and very few over 25 years, giving a wide confidence interval for this older age group and considerable overlap in the incidence rate confidence intervals.
This study emphasizes the need to conduct a locally embedded BED false recent study to adjust the BED incidence estimate. Compared to other cross-sectional studies (e.g., Sexton et al. 18 ), the false recent rates differ so as to preclude application of a common false recent factor across multiple countries or populations. Indeed, even within the same population, two different false recent rates can be found (e.g., studies within Vietnam or South Africa), 19 and if applied would create varying incidence estimates. For instance, if we applied one of the South African false recent rates of 5.6% to these Ethiopia data, the estimated incidence would be near zero, but if we applied the 1.7% FRR from Vietnam, our incidence estimate would be much greater Ideally, we would have conducted a prospective cohort study in parallel with the cross-sectional study to calculate HIV incidence, but funding did not permit.
The younger women in the cohort are newer arrivals to Addis Ababa, and perhaps less skilled in controlling or negotiating their sexual risk behaviors. The self-reported behaviors of the younger and older women did not differ much, however. We found that most of the women reported highly risky sexual behaviors and so potentially intense levels of exposure to HIV/STI. While the majority of cohort members were using some form of contraception, a large percentage were relying on condoms alone. The relatively low pregnancy prevalence is somewhat surprising in light of the moderate prevalence of effective contraception and the high coital frequencies. Integration of family planning and HIV services has been proposed in Ethiopia, 20 and this study should provide further impetus for integrated services, along with educational and risk-reduction programs targeting these young women. The ALERT Hospital is well-positioned to provide integrated reproductive health care for the at-risk surrounding population of young women in that part of Addis Ababa.
The main limitation of this study was that we were unable to conduct a prospective cohort study. Doing so would provide a direct measure of incidence, and would also demonstrate the ability of the site and the willingness of the population to follow-up over months of observation. Our incidence figures are cross-sectional estimates only and are subject to the inaccuracies of the method. Despite these limitations, one of the primary goals of this project was to nurture a new research site that could participate in future HIV prevention trials.
We partnered to increase research capacity, and found an estimated HIV incidence that is sufficient to warrant additional HIV prevention programming in Addis Ababa, as well as to explore future HIV prevention research in the higher-risk catchment area. More broadly, the clinical and laboratory staffing and experience now in place at AHRI demonstrate their readiness for clinical research on HIV and other infectious diseases.
Footnotes
Acknowledgments
This work was funded by the U.S. Agency for International Development (USAID) under Cooperative Agreement no. GPO-A-00-05-00022-00, the Contraceptive and Reproductive Health Technologies Research and Utilization (CRTU) Program, and Cooperative Agreement no. GHO-A-00-09-00016-00, the Preventative Technology Agreement (PTA). Additional support was provided by the U.S. Centers for Disease Control and Prevention (CDC) for expanding the BED false recent phase through contract #200-2010-35109-00001, HIV Incidence Assay Validation. The contents of this article are the responsibility of FHI 360 and do not necessarily reflect the views of USAID or CDC. We thank the study participants, the study team at AHRI, especially Assegid Geleta and Zeyin Zerhun, and the outreach workers at HAPSCO and EHNRI. We also thank several FHI 360 colleagues (current and former) who contributed to the overall project, including Shelly Fischer, Lisa Saylor, Kavita Coombe, Connie Sexton, and Francesca Stuer. Helpful reviews were also provided by our FHI 360 colleagues and the anonymous reviewers.
Author Disclosure Statement
No competing financial interests exist.