
Abstract
The high diversity of HIV-1 has been shown to affect disease progression, transmission, and response to antiretroviral therapy and may influence HIV vaccine design. We describe the distribution trends of HIV-1 subtypes over a 7-year period among incident cases in a rural clinical cohort in Southwest Uganda and identify transmission clusters. Viral RNA was extracted from cryopreserved plasma samples from 94 participants who seroconverted and enrolled between 2004 and 2010. Partial gag (p24) and env (gp41) genes were directly sequenced to identify subtypes and transmission clusters with more than 95% bootstrap values. Direct sequencing of the partial pol gene and use of individual participant sexual life histories were also used to confirm these transmission clusters. The overall gag/env subtype distribution was A 28% (n=26), C 1% (n=1), and D 45% (n=42) and 27% (n=25) were intergene unique recombinant forms. The proportions of subtype A, D, or recombinants showed no significant increasing or decreasing trend over this time period (p=0.51). Phylogenetic analysis of the three genes confirmed 13 transmission clusters of which seven clusters were confirmed sexual partners using individual participants' sexual life histories. Subtype D has remained the predominant subtype in this population. From 2004 to 2010, there was no change in the proportions of these subtypes. Phylogenetic analysis and participants' sexual life histories revealed several transmission clusters. The high proportion of transmission clusters observed suggests continued high-risk sexual behavior and mixing in some individuals and possibly super transmitters in this presumed low-risk cohort, but also indicates that many transmissions occur in early HIV infection. This calls for early and targeted effective prevention and treatment intervention in this population.
Introduction
T
In Uganda subtype A and D predominate, 5 –7 with a few cases of subtype B, 8 –10 C, 6,10,11 and G, which was first described in Uganda in 1995 12 but has rarely been identified since then. Recombinant forms of subtype A and D have also been observed. 7,10,11,13,14 Several studies have associated subtype D with faster disease progression than subtype A suggesting that subtype D is more pathogenic than subtype A. 9,15 –19 It has also been demonstrated among HIV serodiscordant couples in Rakai district, Uganda, that subtype A viruses were more transmissible than subtype D viruses. 20 Recently another study in Rakai district among prevalent cases reported that the distribution of HIV-1 subtype A increased compared to subtype D over an 8-year period. 21 The changes in subtype proportions were attributed to faster disease progression in subtype D compared with subtype A, meaning patients with subtype D were more likely to die, and higher transmission rates of subtype A. 20 This is in contrast to a previous study among incident cases in a rural clinical cohort in Southwest Uganda that showed no significant change in proportion of subtypes A and D over a 10-year period. 5 Uganda was one of the first countries in East Africa to introduce antiretroviral therapy (ART), which reduces disease progression for those who receive ART. This may also have an effect on the distribution of subtypes; because progression is faster with subtype D 9,15 –19 and ART reduces mortality, the proportion of D is likely to remain constant or possibly increase. At the same time since subtype A is more likely to be transmitted 20 and ART reduces transmission by reducing individual and community viral load levels, then incident subtype A cases are likely to decrease over time. Information on circulating HIV-1 subtypes is important for vaccine design and may also be useful in optimizing treatment strategies as some studies have shown varying responses to treatment among the different subtypes. 22,23
Earlier studies reported that early stages of HIV infection were associated with high viral loads in blood and semen, and were therefore more important in HIV transmission and spread of the HIV epidemic. 24 –28 However, Hollingsworth et al. reported that although early and late stages of HIV disease are more infectious, this is for shorter periods, and the asymptomatic stage of infection contributes more to the net transmission over a lifetime of an infected individual because of its longer duration. 29 In a general population cohort in rural Uganda, there was a general decrease in HIV incidence from 1990 to an all time low in 2005 (with similar trends observed among men and women). However, new infections continued in some subgroups; men aged 40–44 years and women aged 30–34 years showed incidence peaks in the period 2000–2005. 30 Knowledge of HIV transmission dynamics is important in order to design more effective prevention and treatment interventions in such populations and to monitor transmitted HIV drug resistance. 31 It is therefore important to trace the etiology of new HIV transmissions to better understand our local epidemic.
Currently, there are no data describing trends of HIV-1 subtypes among incident cases in this rural cohort since the introduction of ART, which has proven efficacious in reducing transmission. In this study, we describe the HIV-1 subtype distribution and trends among incident cases diagnosed between 2004 and 2010 after the introduction of antiretroviral therapy in a rural clinical cohort in Southwest Uganda. We also describe the HIV-1 transmission clusters identified in this cohort.
Materials and Methods
Study population
In 1989 the Medical Research Council Programme on AIDS in Uganda established a General Population Cohort (GPC) with around 5000 adults residing in 15 villages in rural Southwest Uganda. 32 In 1999, an additional 10 villages were added to this cohort. 33 In 1990, a natural history cohort (NHC) was established to study the disease progression of HIV-1-infected participants within the GPC. 34 In 2004 free ART was introduced for all eligible study participants according to the Uganda Ministry of Health National ART guidelines, 35 and the NHC was renamed the Rural Clinical Cohort (RCC). New HIV-seropositive participants (incident cases) with estimated dates of seroconversion were identified through annual GPC serosurveys, and invited to enroll in the RCC. At enrollment, all HIV-1 incident cases had 4 ml of blood collected in an EDTA tube and transported within 24 h to the Medical Research Council (MRC)/Uganda Virus Research Institute (UVRI) Basic Science laboratory for testing or storage. Of the 115 participants that seroconverted between 2004 and 2010, samples from 94 incident participants were used in this study. Sexual life history information was also collected by study field workers from the participants through individual interviews.
Laboratory procedures
Viral RNA was extracted from cryopreserved plasma using the QIAamp Viral RNA Mini kit (Qiagen Inc., Valencia, CA) according to the manufacturer's instructions. The eluted RNA was expanded by reverse transcriptase polymerase chain reaction (RT-PCR) followed by nested PCR in two separate reactions using in-house gene-specific primers. The primers and protocols used to amplify portions of the gag (p24) (HXB2 nt 1577–2040) and env (gp41) (HXB2 nt 7850–8310) genes have been described in detail previously. 14,36 To support suspected transmission clusters identified in the gag and env, the pol gene encompassing amino acids 1–99 of protease and 1–242 of reverse transcriptase was amplified using in-house gene-specific primers as previously described. 37 Amplified PCR products were purified using the Qiagen purification kit (Qiagen Inc., Valencia, CA). The sequencing of the three genes (gag, env, and pol) was performed under conditions previously described. 14,36,37 The DNA sequencing was carried out using a Beckman CEQ 8800 automated capillary DNA sequencer.
Phylogenetic analysis and subtyping
The chromatogram files were assembled and edited using Sequencher version 4.10.1 (GeneCodes Corporation, Ann Arbor, MI). The edited sequences were aligned with reference subtype sequences of HIV-1 group M downloaded from the Los Alamos National Library HIV Sequence Database (
Statistical analysis
For descriptive purposes the subtypes were classified as A, C, D, or recombinants and were cross-tabulated by year of seroconversion, gender, and age group, respectively. The age distribution was compared between subtypes using a Kruskal–Wallis test. To determine whether the distribution of subtypes changed over time and also whether the distribution varied by gender and age group, the following procedure was adopted. First, separate logistic regression models were fitted to the proportions of subtype A, subtype D, and recombinants, treating year as a continuous variable, i.e., examining linear trends over time; thereafter an overall multinomial logistic regression model was fitted with the response being subtype categorized as D, A, C, or recombinant with subtype D being the reference category. Analysis was carried out using STATA release 10.0 (Stata Corp., 2008).
Ethical considerations
The Uganda Virus Research Institute Science and Ethics Committee and Uganda National Council for Science and Technology approved the study. All participants provided signed or thumbprinted written informed consent for their samples to be stored and used for future research purposes.
Results
Of the 94 samples genotyped in the gag (p24) and env (gp41) genes (gag/env), 42 (45%) were subtype D/D, 26 (28%) subtype A/A, 1 (1%) was subtype C/C, and 25 (27%) were intergene recombinants. The (gag/env) intergene recombinants were distributed as follows: 12 (13%) were D/A, 9 (10%) A/D, 3 (3%) C/A, and 1(1%) D/C. In the study, 66 (70%) of the participants were females. Although 50% of females were infected with subtype D compared with 32% of males, there was no evidence that HIV subtype distribution differed by gender (p=0.31) (Table 1).
Chi-square=7.14 on 6 df. p=0.31. Fisher exact p=0.26.
The majority of seroconversions, 52/94 (55%), occurred in 2007 and 2008. There was a nonsignificant decrease in the proportion of subtype D and an increase in the proportion of subtype A (p=0.51). Logistic regression models fitted to the probability of being subtype A showed no effect of gender (p=0.90), age group (p=0.73), or year of seroconversion (p=0.71). There was also no significant association between the probability of having subtype D or having a recombinant subtype and gender, age group, and year of seroconversion as none of these factors approached significance in the multinomial logistic regression model. Similarly the Kruskal–Wallis test showed no evidence that the age distributions differed between subtypes (chi-square=3.116, p=0.37). There was no particular trend in the subtype distribution over time (Fig. 1).

Trends in subtype A, D and recombinant distribution over time (2004–2010). HIV-1 subtype proportions by year among the incident cases in the rural clinical cohort.
Identification of possible transmission clusters
The phylogenetic analysis revealed some possible transmission clusters with bootstrap values >95% in more than one genomic region (Table 2). In the gag (p24) (Fig. 2) there were nine clusters (C2, 3, 4, 5, 6, 7, 9, 10, and 16) and env (gp41) (Fig. 3) had 10 clusters (C2, 6, 7, 8, 9, 10, 11, 12, 13, and 16) with bootstrap values of >95%. To confirm these clusters, a larger fragment of the pol gene was sequenced (Fig. 4). A total of seven clusters (C1, 2, 6, 7, 9, 10, and 16) had participants with their sequences clustering in all three regions (gag/env/pol) (Figs. 2, 3, and 4). Eight clusters (C1, 2, 6, 7, 8, 9, 10, and 16) appeared in both gag/env, 10 clusters (C1, 2, 6, 7, 9, 10, 11, 13, 15, and 16) appeared in both env/pol regions, and 9 clusters (C1, 2, 3, 4, 6, 7, 9, 10, and 16) appeared in gag/pol. There were three clusters, which appeared only in either gag (C5), env (C12), or pol (C17) and these were excluded from the analysis. Seven of the total 13 clusters (C3, C4, C7, C8, C9, C10, and C11) were either confirmed sexual partners or individuals confirmed to have shared a partner, using participant individual sexual life histories, whereas the other clusters had no data to support their clustering (Table 2).
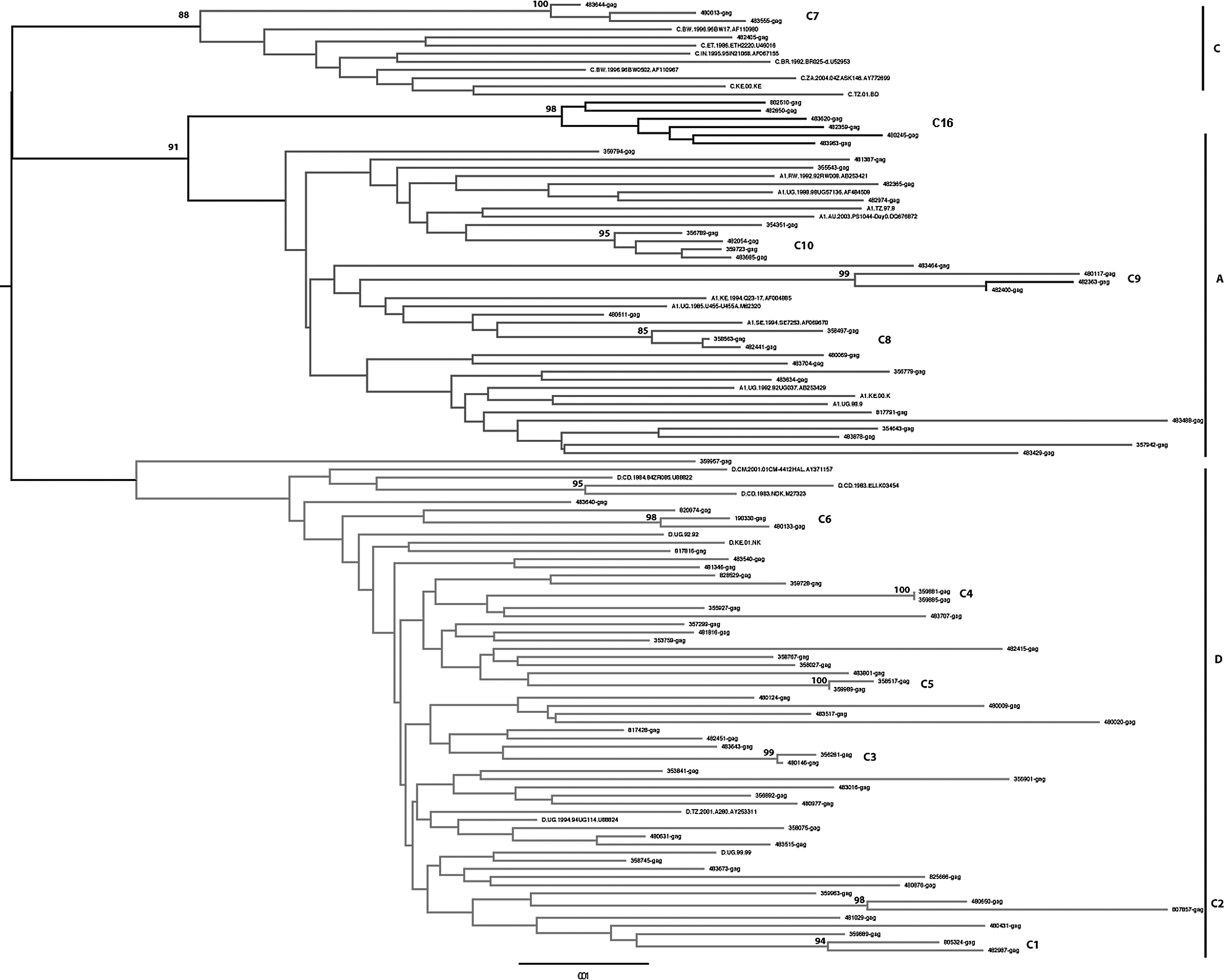
Phylogenetic analysis of the gag (p24) sequences obtained from the rural clinical cohort, reference sequences from the Los Alamos sequence database. The phylogenetic plots represent consensus sequences of the participants.
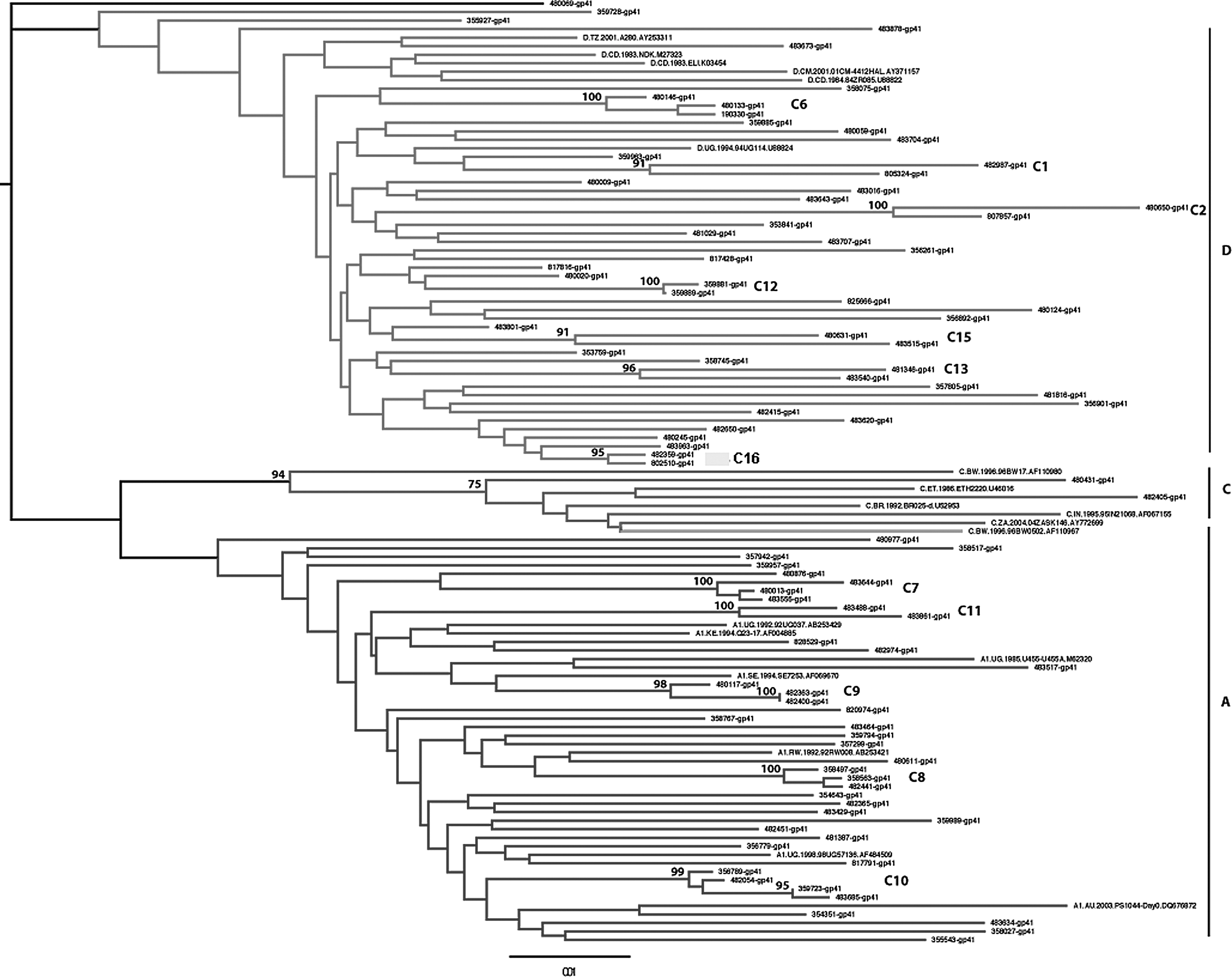
Phylogenetic analysis of the env (gp41) sequences obtained from the rural clinical cohort, reference sequences from the Los Alamos sequence database. The phylogenetic plots represent consensus sequences of the participants.
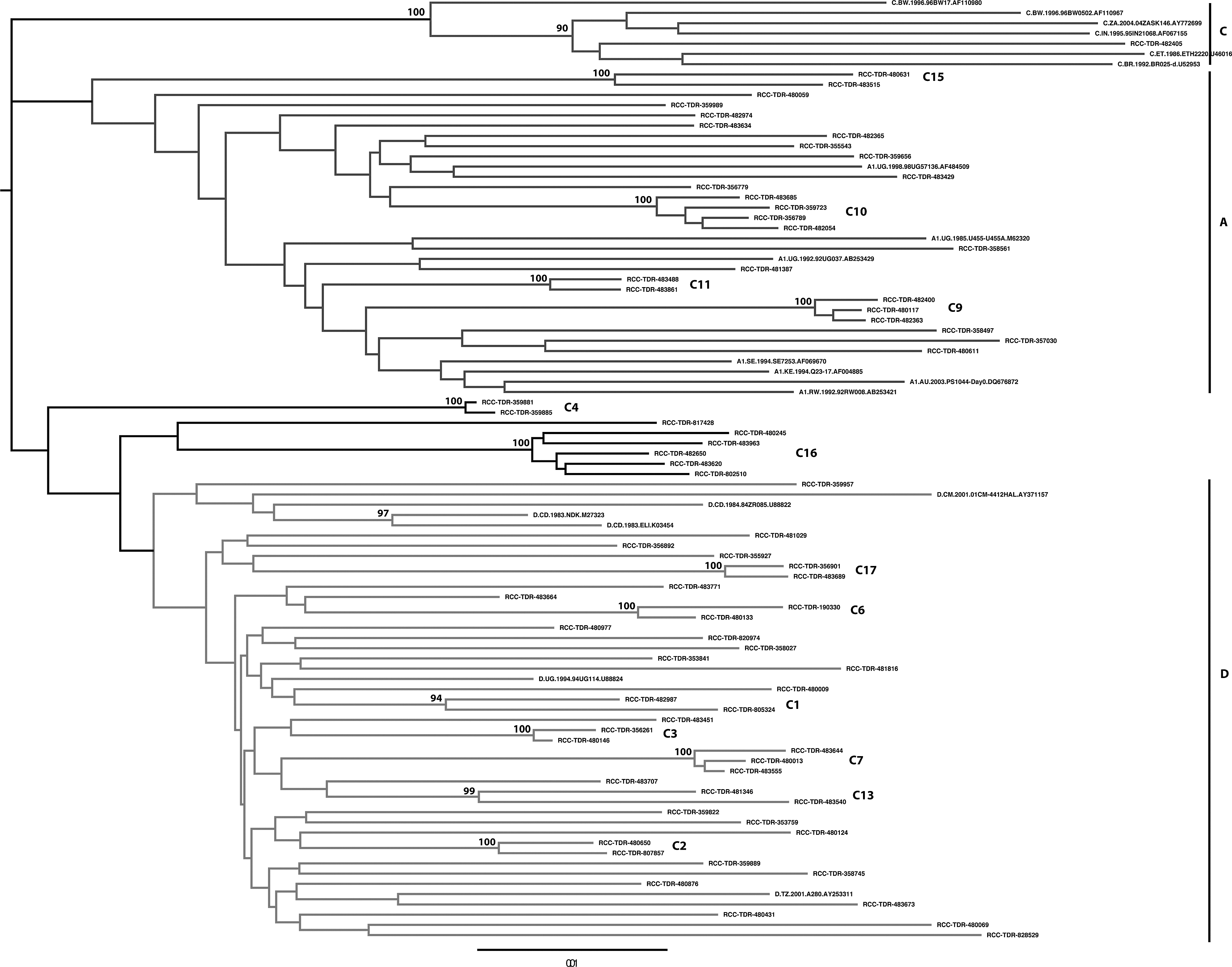
Phylogenetic analysis of the pol sequences obtained from the rural clinical cohort, reference sequences from the Los Alamos sequence database. The phylogenetic plots represent consensus sequences of the participants.
ART, antiretroviral therapy.
Discussion
In this study of the distribution of HIV-1 subtypes over time, which included the period of introduction and roll out of ART in a clinical cohort in rural Southwest Uganda, subtype D remained the predominant subtype with a prevalence of 45% followed by subtype A (28%) and recombinants (27%). Previous studies have also found subtype D to be predominant in rural Southwest Uganda 5,7,43,44 while subtype A is predominant in the central and northern parts of Uganda. 36,37,45 In our study, there was only one (1%) subtype C incident infection, a finding that is consistent with other reports that found no significant increase in the proportion of subtype C infection. 5,21,46
We did not find any significant trend to show that the proportion of one subtype or recombinant increased or decreased over this study period. Our findings partly agree with those previously found between 1990 and 2000 in the same cohort that reported no significant changes in the proportions of the different subtypes over the 10-year period; however, a significant reduction in the proportion of recombinants from 36% in 1990/1991 to 14% in 1998/19995 was observed, which was not the case in our study. Our findings are also consistent with earlier studies in other parts of Uganda, among patients attending clinics in Kampala and Entebbe over a 3-year period 6 and among women attending antenatal clinics over a 12-year period, 45 which also reported no significant changes in the proportions of HIV-1 subtypes A, D, or their recombinants. However a recent study in Rakai district, Southwest Uganda, among the prevalent cases reported significant declines in subtype D infections from 70.2% to 62.4% and increases in subtype A infections from 16.7% to 23.3% but they did not report any significant changes in the infections caused by recombinants. 21 This was not the case in our study; the main difference between these two studies is the use of incident cases in our report compared to the use of prevalent cases in the Rakai study. Using incident cases better reflects the subtypes that are being transmitted in the population at a particular time. This warrants further studies with larger incident case sample sizes to ascertain the true picture of the trends of HIV subtypes in the country, which will help us better maximize control and prevention strategies.
Previous studies have reported that infections due to subtype D progress faster to AIDS and death than subtype A and that subtype A was more transmissible, suggesting that subtype D would decrease over time compared with subtype A. 18,21 Our study did not show a significant decrease of subtype D or a significant increase in subtype A among the incident cases over this 7-year period, and this could be attributed to the availability of ART in this cohort since 2004. ART has been demonstrated to reduce transmission and save lives independent of the subtype. 47 Therefore with good adherence, there will be reduced transmissions and slowed progression to death leading to no differences in the subtype trends as shown in our study. Although 50% of the females and 32% of the males were infected with subtype D, there was no significant association between HIV-1 subtype and gender, age group, and year of seroconversion. We did not detect any significant trend in the distribution of subtype proportions over the study period.
Phylogenetic analysis in this study revealed several possible transmission clusters infected with closely related viruses and supported by high bootstrap values (>95%) in at least two genomic regions. We have previously used phylogenetics and participant sexual life histories data to describe the HIV-1 epidemic among female sex workers in Kampala and transmission networks were confirmed. 36 The use of both phylogenetics and sexual life histories can effectively be used to describe the dynamics of the epidemic to better understand who is infecting who and where new infections come from, especially in a cohort such as ours in which new infections continue to occur in spite of prevention efforts over the years. In our study, 37% (35/94) of sequences segregated into 13 clusters, suggesting that recent infections could originate from other recent infections or transmission from the same source to different individuals; such possible super transmitters need to be identified. This also confirms the contribution of recent infections to the spread of HIV-1.
Sexual life histories confirmed some of the transmission clusters while the other clusters had no sexual life histories to support their clustering. The lack of sexual life histories to confirm some clusters despite high bootstrap values may possibly be due to denial of sexual relationships among these cohort participants or unrecognized mixing of sexual partners. The collection of sexual life histories of participants in addition to the use of phylogenetics will be a very useful approach in the future to understand local HIV epidemics and targeted prevention efforts.
Contamination was ruled out in all the samples that clustered together by being individually repeated on separate days without altering the results. This phylogenetic analysis strongly suggests sexual mixing within the cohort among linked and unlinked individuals and cases of undisclosed relationships in the cohort or unrecognized transmissions from the same source. Further studies are needed including lifetime sexual histories to better understand the epidemic in this population, which will result in improved public health messages leading to better control and reduction of HIV transmission.
Conclusions
We have shown that in this rural clinical cohort in Southwest Uganda, subtype D is still the predominant subtype followed by subtype A and unique recombinant forms while subtype C is still very rare and with no change in the proportions of these subtypes over a 7-year period. Phylogenetic analysis and participants sexual life histories revealed several transmission clusters suggesting continued high-risk sexual behavior and possibly super transmitters in this presumed low-risk cohort, but also confirming that many transmissions occur in early HIV infection. This calls for early and targeted effective prevention and treatment interventions in this population.
Footnotes
Acknowledgments
The Medical Research Council of the United Kingdom provided funding for this study. We thank the staff and the study participants of the Rural Clinical Cohort.
A.K., F.L., C.M., D.S., and P.K. designed the study. B.N.M. coordinated the field and clinic work. A.K., F.L., B.M., and M.N. performed laboratory testing. A.K., J.L., F.L., D.S., and C.M.P. analyzed the data and wrote the first draft of the manuscript. A.K., D.S., C.M.P., C.M., B.N.M., and P.K. contributed to subsequent drafts. All authors reviewed and approved the final version of the manuscript.
Author Disclosure Statement
No competing financial interests exist.