
Abstract
Few data report the prevalence in actual clinical settings of lipodystrophy (LD), and in particular of facial lipoatrophy (LA), in HIV-infected patients treated with long-term antiretroviral therapy (ART). A French, multicenter, cross-sectional, observational study was conducted in HIV-infected patients on continuous ART for more than 12 months. The main objective was to assess the prevalence of facial LA in this population. Additional objectives were to make the same assessments for nonfacial LA and lipohypertrophy. The presence of LD signs, type, and severity was assessed by clinicians and compared with patient self-evaluations through two questionnaires. A total of 2,131 assessable patients had a median age of 46 years and a median time on ART of 10 years. Physicians diagnosed facial LA in 54% of patients and these subjects had received ART for a longer duration than those without LA. Thymidine analog usage was associated with an increased likelihood of facial LA, but 28% of patients recently treatment-initiated (1–5 years) were also affected. At other sites, LA and lipohypertrophy were diagnosed in 59% and 57% of cases, respectively. The concordance between physician and patient assessments was good for facial and buttocks LA. In this study, facial LA affects more than half of the subjects and is frequent even among the most recently treated patients. The prevalence of facial LA significantly increases with the duration of ART, with male gender, hepatitis C virus (HCV) coinfection, and non-African origin being independent risk factors. Lipohypertrophy is frequent and appears early after ART initiation.
Introduction
C
The pathophysiological mechanisms of LD are multifactorial and include mitochondrial dysfunction, hormonal and inflammatory marker disturbances, and alteration of stem cell differentiation. 3 The causes of LD can include specific host genetic factors, 5 HIV infection itself, and also antiretroviral (ARV) therapies. Among ARV therapies, data consistently point toward the role of thymidine analog nucleoside reverse transcriptase inhibitors (NRTIs) 6 in the development of LA. However, the causes of lipodystrophy appear complex, and may involve most ARV drug classes and/or be partially dependent on different drug–drug interactions. 2,7
The occurrence of LA, and particularly of facial LA, often appears as a visible stigmatizing sign of HIV infection. This can induce diverse psychological effects and eventually cause erosion of self-esteem and depression. 8,9 The psychological impact of facial LA may even put a patient's compliance to ART at risk, 10,11 with the associated risk of virologic failure.
Previous studies have reported prevalence rates of lipoatrophy of between 15% and 38%; however, a consistent definition of LA is lacking and varies between the patient groups studied. 12,13 Similarly, the prevalence of LD varies across studies between 38% and 62%. 14 –16 The most common risk factors identified for LD and/or facial LA are the duration of ART, underlying patient conditions including female gender, 13,15 increasing age, body mass index, and duration and severity of the HIV infection. 13 –16 Risk factors for children and adolescents are very similar. 17,18
There is no unique treatment for LD: in general, prevention of lipoatrophy by avoidance of thymidine analogs is advocated. 6,19,20 In patients with established lipodystrophy, there are limited treatment options, including plastic corrective surgery or refill injections for LA. 21 To date few drugs have a proven efficacy despite numerous studies, particularly with the glitazone class. 22
In France, HIV treatment is scrutinized with regard to its medical and psychological impact on patients. Data on the prevalence of LD (and specifically regarding facial LA), and the factors associated with this condition, are lacking. Whether newer treatment strategies using recent drugs did reduce the frequency of these disturbances can be questioned. Therefore, this epidemiological study was performed to assess the prevalence of facial LA and the prevalence of LD in French HIV-infected patients treated with long-term ART.
Materials and Methods
Study design
This observational, cross-sectional, multicenter study was conducted in France from January to October 2009. The primary objective was to evaluate the prevalence of facial LA in HIV-infected patients on ART for at least 1 year, through a questionnaire completed by the physician. Other objectives were to describe and evaluate the prevalence of lipohypertrophy and mixed lipodystrophy syndromes (physician questionnaire) and evaluate the lipodystrophy score, body image satisfaction score, and perceived quality of life score through a specific, multidimensional patient self-administered “Assessment of Body Changes and Distress” (ABCD) questionnaire. The study protocol and informed consent were approved by French Regulatory Authorities.
Participation in the study was proposed in a random order with geographic stratification to all HIV drug-prescribing physicians throughout France. Those agreeing to participate were asked to propose the study to all eligible patients presenting at their clinic until a maximum of 25 patients were included. Accrual of any new investigating physician or patient was stopped at an appropriate time making it possible to reach the objective of including around 2,000 patients.
Demographic characteristics were completed by the physician at the end of the consultation: gender, age, weight, height, ethnicity, HIV and treatment histories, mode of infection, CD4 count and plasma viral load (VL), current or previous treatment with zidovudine (AZT) or stavudine (d4T), and coinfection with hepatitis C (HCV) or B (HBV) viruses.
The prevalence and severity of LA and LH were assessed. LA, defined as the presence of at least one among six signs of peripheral lipoatrophy (face, arms, legs, buttocks, feet, and visible veins), was rated on the day of the visit by the clinician as mild, moderate, or severe. Facial LA specifically was graded according to the James severity grading (Grade 1: limited lipoatrophy, the appearance is almost normal; Grade 2: some muscles begin to be visible, in particular the zygomatic; Grade 3: the affected area extends beyond the cheeks, the muscles are increasingly visible; Grade 4: the most serious condition, extends to the orbits). 23
LH, defined in the study as the presence of at least one among the listed symptoms (increased abdominal circumference, increased waist circumference, buffalo hump, increased chest circumference, presence of lipoma), and all other abnormalities of fat distribution were similarly assessed by the physician.
Patients completed the self-administered ABCD questionnaire (Assessment of Body Change and Distress). This validated questionnaire consists of three scores: LD score of body changes, overall satisfaction of body appearance, and quality of life (QoL) specific to LD. From questions 1 to 6, the LD score was calculated ranging from 0 (no damage) to 6 (6 affected areas). The seventh question rated the body image satisfaction from 1 to 5 (5: best satisfaction with body appearance). The 21 QoL items allowed the estimation of a QoL score based on four dimensions (disease perception [A], psychological and social impact [B], fear of the future [C], and treatment perception [D]) over the preceding 4 weeks. The calculated QoL score was between 0 and 100 (higher score equates to a better QoL). 8,24 The questionnaire was completed by the patient at the end of the consultation and handed over to the physician in a sealed envelope.
Statistical methods
Descriptive characteristics were provided by the physicians. All statistical analyses were performed on the analysis population, i.e., the total number of patients with no major deviation. The statistical analysis of the primary objective was conducted on the “patient population,” i.e., all patients for whom a patient observation form was completed by the physician. The prevalence of facial LA was estimated using the rate observed in the HIV population and its exact 95% confidence interval (CI) was provided. Secondary objectives including the prevalence of LH and mixed LD were similarly described. Additional analyses were also performed using stratification by ethnicity, previous ART, and HCV or HBV infection. It was calculated that accruing 2,000 patients would make it possible to describe a 15–20% prevalent facial lipoatrophy with a precision of 1.65–1.85%.
LD score, satisfaction with body appearance score, and the QoL scores using the specific multidimensional self-administered questionnaire ABCD were assessed in all patients with an observation form completed by the clinician who returned the self-questionnaire ABCD. The first six questions of the ABCD questionnaire were crossed and compared with the corresponding items from the clinician observation form. To assess the concordance between physician and patient, the kappa coefficient (K) was calculated for each item and was interpreted as indicated by Landis and Koch 25 (00 to 0.20: poor correlation; 0.61 to 0.80: good correlation).
All previous described data were also stratified by gender and by the duration of ART therapy (>1; <5, ≥5; <10 and 10 years or more). A multivariate logistic regression analysis was performed with covariates such as gender, ethnicity, ART duration, and type of treatment in order to identify the factors independently associated with the diagnosis of facial LA. The results of these analyses were expressed as an adjusted odds ratio (OR) with a 95% CI. Regarding the gender, a crude OR was also calculated and compared with the adjusted OR taking into account the duration of treatment. Variables were compared using appropriated statistical tests (Wilcoxon rank, Chi square, Fisher exact, Kruskal–Wallis), which were two-sided with an alpha level of 0.05. Statistical analyses were carried out using SAS software (version 8.2, SAS Institute, Cary, NC).
Results
Disposition of questionnaires
A total of 122 HIV care centers enrolled 2,410 patients and 2,131 physician observation forms were analyzed. The ABCD questionnaire was correctly completed by 2,026 patients, representing a return rate of 95.1%.
Patient characteristics
The majority of patients were male (69.7%) and white (75.9%) (Table 1). The mean age was 47.1±9.7 years. Overall, women were both significantly younger (43.8±9.6 vs. 48.6±9.3 years, p<0.001) and more likely to be from sub-Saharan Africa (31.1% vs. 7.2%, p<0.001) than men. The mean duration of HIV diagnosis was 12.7±6.1 years overall. The modes of transmission were mostly through sexual contact (81%) and drug abuse (13%). HCV and HBV infection were reported in 16.5% and 8.1% of patients, respectively. The mean ART duration was 9.3±4.6 years, and was significantly longer in male than in female subjects (9.6±4.5 years vs. 8.8±4.7 years, p<0.001). Previous ART included zidovudine (AZT) in 83.3% and stavudine (d4T) in 50.9% (mean duration of exposure of 56.5±42.1 months and 43.7±28.8 months, respectively) of patients. Men were more frequently treated with d4T than women (53.1% vs. 45.7%, p=0.002). Treatments with either AZT or d4T were still ongoing in 20.0% and 1.2% of patients, respectively.
BMI, body mass index; ART, antiretroviral therapy.
The majority of patients were virological responders as HIV VL was undetectable in 86.4% of participants, and their mean CD4 count was 585±278 cells/mm3.
Primary endpoint: facial lipoatrophy, physician's assessment
Facial LA was diagnosed by clinicians in 54% of patients (CI 95% 51.9–56.2%). Among these, facial LA was Grade 1 in 36.3%, Grade 2 in 37.0%, and Grades 3–4 in 26.8%. It was more prevalent in men than in women (61.0% vs. 37.8%, p<0.001). Patients with facial LA had received ART for a longer duration than those without LA (10.8±4.1 years vs. 7.6±4.4 years, p<0.001). The prevalence of facial LA significantly increased with the duration of ART (27.8% for >1 to <5 years, 47.5% for ≥5 to <10 years, and 69.7% for ≥10 years, p<0.001) (Fig. 1). It was more prevalent in HCV coinfected patients compared with non-infected patients (74.3% vs. 50.1%, p<0.001) and in non-Africans in comparison to Africans (59.0% vs. 32.5%, p<0.001).

Presence of facial lipoatrophy.
Facial LA was significantly more frequent in patients who had received d4T alone (66.7%), d4T or AZT (73.6%), or AZT alone (38.7%) than in those never treated with these drugs (22.8%) (p<0.001). The severity of facial LA increased significantly parallel to the duration of exposure to d4T.
Logistic regression analysis showed that, regardless of gender, increased duration of therapy with ART (OR: 5.10) and intake of d4T alone (OR=6.44), (3.87–10.73), or d4T or AZT (OR=9.89) were associated risk factors of facial LA (p<0.0001). Conversely, the risk of facial LA was not associated with ethnicity (Table 2) and gender was a confounding factor.
Wald chi square test.
LA, lipoatrophy; AZT, zidovudine; d4T, stavudine.
Secondary endpoints: non-facial lipoatrophy, physician's assessment
Other signs of peripheral LA were present in 58.9% of patients with two, three, four, and even five different anatomical localizations being reported in 8%, 13%, 16%, and 10% of these cases, respectively. This occurred more frequently in men than in women (61.7% vs. 52.2%, p<0.001). The most frequent nonfacial LA signs were slimming of the buttocks (48.0%) and legs (45.0%) (Fig. 2).
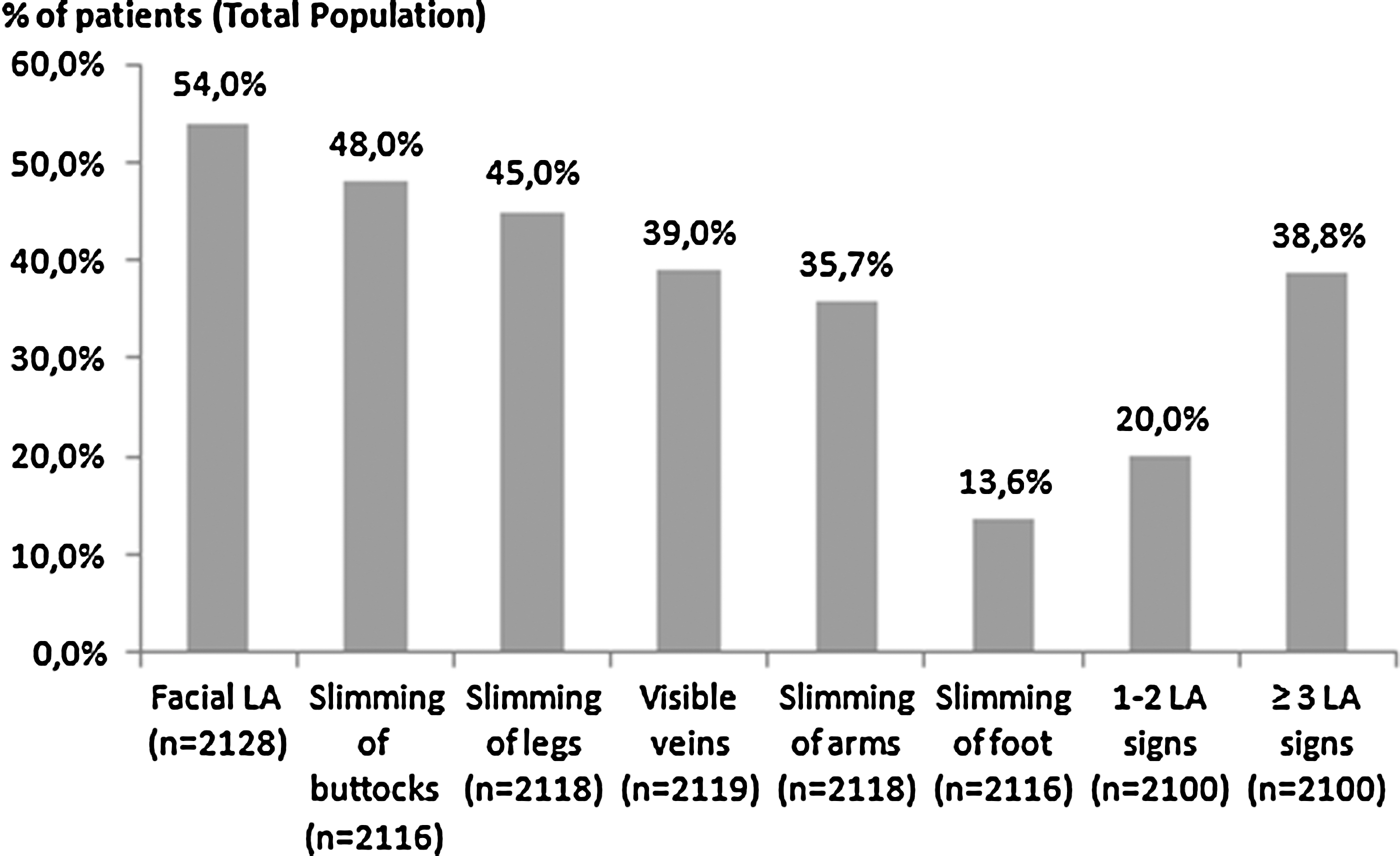
Distribution of lipoatrophic signs (total population).
The prevalence of non-facial LA significantly increased with the duration of ART (p<0.001) and almost doubled in patients treated for 5–10 years versus less than 5 years.
Lipohypertrophy, physician's assessment
Overall, LH was reported in 57% of patients of whom the majority were male (63.1%). Increased abdominal circumference (50.9%) and waist and chest circumferences (43.3% and 24%, respectively) were the most frequently observed signs, with significant association to older age, weight, and body mass index (BMI) (p<0.001). LH appeared mainly between 1 and 5 years of ART (48.0% in patients receiving ART for less than 5 years, versus 56.4% for 5–10 years, p<0.001).
Mixed lipodystrophy syndrome, physician's assessment
Mixed LD, defined as the presence of at least one LA sign and one LH sign, was reported in 42.0% of patients. Its occurrence was correlated with the duration of ART (OR: 5.84, CI 95%: 4.36–7.81), with a prevalence in subjects on ART for more than 10 years of 53.6%, versus 21.5% in those treated for less than 5 years (p<0.001).
Medical and surgical care, physician's assessment
At least one sign of LD was present in 1,766 patients. There was no intervention in 765 cases (43.3%). Drug intervention was used in 105 patients (5.9%) (levocarnyl, metformine, glitazones). The remaining 896 patients had a change of ARV treatment (38.1%), an injection of fillers (18.6%), liposuction (2.1%), or autologous fat transfer (1.9%).
Of the 1,150 patients experiencing facial LA, 26.9% had surgical care [e.g., injections of fillers (poly-
Patient reported outcomes (PRO): self-administered questionnaire
Wasting of the buttocks (50.6%), increased waist circumference (47.0%), sunken cheeks (46.5%), slimming arms and/or legs (45.5%), increased chest (24,4%), and buffalo hump (12,5%) were reported by patients. The mean LD score was 2.3±1.7. The mean satisfaction score of physical appearance was 3.2±1.1. Moreover, 29.2% of all patients reported being unsatisfied or very unsatisfied with their body image. The mean QoL score (Table 3) was 68.8±21.3, with a lower score in females than in males, in patients with LA versus those without LA, in HCV coinfected versus HIV monoinfected subjects, and in those corrected versus those not corrected with fillers injections (p<0.001 for each). The mean QoL score significantly decreased according to the duration of ART from 74.4±20.0 in patients treated for less than 5 years to 71.2±20.8 in patients treated for 5–10 years and 65.0±21.5 in patients treated over 10 years (p<0.001).
Disease perception [A], psychological and social impacts [B], fear of the future [C], treatment perception [D].
Rank test of Wilcoxon and test of Kruskal–Wallis used for comparisons between gender and duration of treatment, respectively.
NA, nonapplicable.
Overall, female patients reported a higher LD score and level of dissatisfaction within each category (A, B, C, D) than male patients (p<0.001).
Correlations between the physician's and patient's answers
The concordance of answers between physician and patient (expressed in K=kappa coefficient) was rated “good” for two questions: “wasting of the buttocks” (K=0.64) and “facial LA” (K=0.61), whatever the gender. It was good for the slimming of the limbs (K=0.62) only in female patients. Regarding other body areas (waist and chest circumferences, slimming legs and/or arms, buffalo hump), the correlations were “moderate” (K ranging from 0.6 to 0.47).
Overall, patient's and physician's perceptions were convergent for several causes of dissatisfaction with LA or LH: very unsatisfied with the wasting of buttocks (76.1% of patients, 60.3% of physicians) and increase in waist circumference (66.4% of patients, 69.5% of physicians).
Discussion
There is no standardized, consensual way to define and evaluate facial LA. This applies even more to non-facial LA and LH. Consequently, we elected to base our assessments on two questionnaires: (1) one medical questionnaire completed by the physician, and (2) one evaluating the perception of LD symptoms through the ABCD validated questionnaire and completed by the patient.
In this nation-wide French study, the prevalence of facial LA was 54%, whereas it varied from 11% to as much as 83% in previous studies 14,16 in differing populations. Increased age and a lower baseline BMI were identified risk factors regardless of the duration of ART. In addition, facial LA was more prevalent in men than in women (61% versus 38%). Stratified analysis showed that the duration of ART was a determining factor in the occurrence of facial LA, regardless of gender.
Facial LA was more prevalent in HCV coinfected patients, consistent with results from previous studies, including a French cohort study. 16,26 HIV and HCV (and possibly use of interferon plus ribavirin) may independently cause mitochondrial DNA damage, and in conjunction with the length of ART exposure account for the greater risk and severity of LA in HIV-HCV coinfected patients. 26
Globally, the prevalence of facial LA was strongly linked to the use of thymidine analogs, but even in subjects recently initiated on HIV therapy it remains a frequent adverse event (28% in patients treated for 1–5 years). Although facial LA was more frequent in persons of non-African versus African origin, the logistic regression analysis showed that the prevalence was not influenced by ethnicity when considering the exposition to thymidine analogs, while other studies in HIV-infected children or adults found that a smaller proportion of African people is affected by LA. 1,15 In terms of frequency, our results do not differ from those recently observed in Senegal. 27 The correction of facial LA was mainly based on refill injections (26.9%), as this intervention is reimbursed in France. 21,28 Most frequently, the decision to use this type of intervention is based on the patient's subjective perception of his condition.
Apart from the face, LA can affect other body sites, most frequently the buttocks and legs. Of note, slimming of the fat in the soles was reported in 13.6% of our patients and is an adverse event that has been rarely reported elsewhere.
The prevalence of LH is 57.9%. Contrary to LA, LH signs appeared earlier and tended to stabilize over time. Increased age and higher BMI were risk factors for LH.
Finally, our study showed that a mixed LD syndrome is frequent and reported in as many as 53.6% of patients on ART for more than 10 years. Wasting of the buttocks, increased waist circumference, and sunken cheeks were the most frequently observed symptoms of mixed LD.
The QoL was low (ranging between 69 and 86), specifically in patients experiencing LA, in women, and in those with HCV coinfection. This is consistent with previous data showing the negative impact of LD on QoL. 10,11,29 –31 The PRO part of the study raised a good level of interest, as 95% of the questionnaires were completed. This type of assessment should be more routinely used when monitoring LD as it provides a personalized insight on the impact of symptoms on the patient's life.
The level of correlation between patient's and physician's perceptions of the symptoms varied according to the nature of the symptoms, with a good concordance for LA of the face and buttocks, and moderate for the other sites. These correlations were higher than those reported in non-HIV diseases. 31 This study has some limitations as it is cross-sectional and does not use objective evaluation of LD, e.g., CT scan or DEXA. There may have been some degree of selection bias, as it is possible that the patients who agreed to participate were more concerned by lipodystrophy issues than those who did not.
Considering that the grading of facial LA was performed during the inclusion visit, this might have lowered, for patients having undergone corrective actions in the past (e.g., refill injections), the grading but not the prevalence of facial LA. In spite of these limitations, this study allows us to describe, in a very large population of treated patients, the frequency of fat distribution abnormalities and their main risk factors.
In conclusion, facial LA affected more than half of the subjects with long-term HIV infection treated with ART, with a high prevalence even in patients recently initiated on ART. LA significantly affected QoL, in particular in women and in HCV coinfected subjects. The prevalence of facial LA significantly increases with the duration of ART, with male gender, HCV coinfection, and non-African origin being independent risk factors. LH was also frequent and appeared early after ART initiation. As long as we have no strategy leading to a cure for HIV, physicians must be aware of drug toxicities and their impact on patient perception and quality of life.
Footnotes
Acknowledgments
The authors are grateful to the following for their participation: the patients from the Preface study and the study investigators: A. Berrebi, Hôpital Paule de Viguier, Toulouse; A. Blanc, CH de Bicêtre, Le Kremlin Bicêtre; A. Cheret, Hôpital Font Pré, Toulon; A. Creuwelsbonneau, CH Gaston Ramon, Sens; A. Madrid, Hôpital de la Conception, Marseille; A. Py, Réseau Pau VIH, Pau; A. Trylesinski, HEGP, Paris; B. Castan, Hôpital Impératrice Eugénie, Ajaccio; B. Christian, Hôpital Notre Dame du Bon Secours, Metz; B. Dupont, CH Necker enfants malades, Paris; B. Giffo, CHBT, Basse Terre, Guadeloupe; B. Lebouche, Hôpital Hôtel Dieu, Lyon; C. Aquilina, Hôpital de la Grave, Toulouse; C. Augustin Normand, Hôpital Hôtel Dieu, Lyon; C. Barbuat, Hôpital Caremeau, Nîmes; C. Beck, Hôpital Emile Muller, Mulhouse; C. Billy, CH François Quesnay, Mantes la Jolie; C. Biron, Hôpital Hôtel dieu, Nantes; C. Chartier, Strasbourg; C. Fontier, CH de Valenciennes; C. Gaud, CHD Félix Guyon, Saint Denis, La Réunion; C. Genet, CHU Dupuytren, Limoges; C. Penalba, Hôpital Manchester, Charleville Mézières; C. Ricaud, CHD Félix Guyon, Saint Denis, La Réunion; C. Rouger, Hôpital Robert Debré, Reims; C. Tomei, Hôpital de la Conception, Marseille; D. Binet, Paris; D. Houlbert, Centre Gui de Chauliac, Montpellier; D. Line, CH de Soissons; D. Salmon Ceron, Hôpital Cochin, Paris; E. Badsi, Hôpital Lariboisière, Paris; E. Brottier Mancini, Hôpital Saint Louis, La Rochelle; E. Carbonnel Delalande, Hôpital Edouard Herriot, Lyon; E. Klement Grandjean, CMC de Bligny, Briis sous Forges; E. Legrand, CH d'Annonay; E. Rosenthal, Archet I, Nice; F. Bani Sadr, Hôpital Tenon, Paris; F. Borsa Lebas, Hôpital Charles Nicolle, Rouen; F. Boulard, CHBT, Basse Terre, Guadeloupe; F. Granier, CH François Quesnay, Mantes la Jolie; F. Jeanblanc, GH Edouard Herriot, Lyon; F. Lescure, Hôpital Tenon, Paris; F. Lucas, Hôpital de la Grave, Toulouse; F. Lucht, Saint Galmier; F. Prevoteau, Hôpital de la Grave, Toulouse; F. Raffi, Hôpital Hôtel Dieu, Nantes; G. Cessot, Centre médical institut Pasteur, Paris; G. Force, Hôpital Notre Dame du Perpétuel Secours, Levallois Perret; G. Hittinger, Hôpital Font Pré, Toulon; G. Le Moal, CHRU la Miletrie, Poitiers; G. Lepeu, CH Henri Duffaut, Avignon; H. Touitou, Hôpital Jean Verdier, Bondy; I. Auperin, CH André Grégoire, Montreuil; I. Rouanet, Hôpital Caremeau, Nîmes; J. Berger, Hôpital Robert Debré, Reims; J. Cervoni, Hôpital Lariboisière, Paris; J. Chennebault, Hôtel Dieu, Angers; J. Esnault, CH départemental les Oudairies, La Roche sur Yon; J. Faller, CH de Belfort; J. Jacquet, Centre Gui De Chauliac, Montpellier; J. Laurichesse, CH François Quesnay, Mantes la Jolie; J. Livrozet, GH Edouard Herriot, Lyon; J. Marionneau, CH du Mans; J. Mattei, Hôpital Sainte Marguerite, Marseille; J. Pouaha, Hôpital Notre Dame du Bon Secours, Metz; J. Riou, CH du pays d'Aix, Aix en Provence; JL. Schmit, Hôpital Nord, Amiens; K. Ghomari, CH de Beauvais; K. Koffi, Hôpital Hôtel Dieu, Lyon; L. Belarbi, Hôpital Cochin, Paris; L. De Saint Martin, Hôpital la Cavale Blanche, Brest; L. El Hajj, Hôpital Simone Veil, Eaubonne; L. Faba, CH Saint Louis, La Rochelle; L. Gerard, Hôpital Saint Louis, Paris; L. Hocqueloux, Hôpital La Source; L. Lerousseau, Hôpital d'Antibes Juan les Pins; L. Prudhomme, CHI de Castres; L. Roudiere, CH Necker enfants malades, Paris; M. Blanc Derradji, Hôpital Albert Michalon, Grenoble; M. Bonmarchand, CH Pitié Salpêtrière, Paris; M. Khuong Josses, Hôpital Delafontaine, Saint Denis; M. Kirstetter, Paris; M. Obadia, Hôpital Purpan, Toulouse; M. Philippon, CH Antoine Gayraud, Carcassonne; M. Priester, Hôpital Civil, Strasbourg; M. Souala, Hôpital Pontchaillou, Rennes; MP. Treilhou, Hôpital Cognacq Jay, Paris; N. Canu, Hôpital de Fleyriat, Bourg en Bresse; O. Taulera, Hôpital Cochin, Paris; O. Zak Dit Zbar, Hôpital Cognacq Jay, Paris; P. Allegre, CH du pays d’ Aix, Aix en Provence; P. Brousse, Hôpital des Escartons, Briançon; P. Cheval, Centre Gui de Chauliac, Montpellier; P. Chiarello, GH Edouard Herriot, Lyon; P. De Truchis, Hôpital Raymond Poincaré, Garches; P. Fialaire, Hôtel Dieu, Angers; P. Heudier, CH princesse Grace, Monaco; P. Lataste, CH de Périgueux; P. Lebret, Hôpital Bretonneau, Tours; P. Leclercq, Hôpital Albert Michallon, Grenoble; P. Mercie, Hôpital Saint André, Bordeaux; P. Muller, Hôpital Beauregard, Thionville; P. Perre, CH départemental les Oudairies, La Roche sur Yon; P. Philibert, Hôpital Ambroise Parée, Marseille; P. Poubeau, GHSR, Saint Pierre, La Réunion; P. Rodon, CHU de Blois; P. Suel, CH de Dieppe; R. Djebbar, Hôpital Avicenne, Bobigny; S. Bregigeon, Hôpital Sainte Marguerite, Marseille; S. Chadapaud, Hôpital Font Pré, Toulon; S. Radenne, Hôpital Hôtel Dieu, Lyon; S. Sire, CH Jean Rougier, Cahors; S. Tempesta, Hôpital d'Antibes Juan les Pins; T. Akpan, CHI Meulan les Mureaux; V. Baillat, Centre Gui de Chauliac, Montpellier; V. Gueripel, Hôpital Hôtel Dieu, Lyon; V. Jeantils, Hôpital Jean Verdier, Bondy; V. Martinez Tadayoni, Hôpital Antoine Béclère, Clamart; V. Reliquet, Hôpital Hôtel Dieu, Nantes; X. De la Tribonniere, Hôpital Guy Chatiliez, Tourcoing; Y. Quertainmont, CH de Bicêtre, Le Kremlin Bicêtre.
We thank Dr. Jean van Wyk, AbbVie Laboratories for his kind review of the manuscript, AbbVie Laboratories for funding the research, and Sanofi-Aventis for providing financial support
Author Disclosure Statement
S. Carret, P. Ngo Van, J. Thevenon are Abbvie employees; M. Hellet and J.P. Meunier were appointed by Abbvie for the data management and analyses. No other competing financial interests exist.