
Abstract
HIV-infected children are at high risk of acquiring drug-resistant viruses, which is of particular concern in settings where antiretroviral drug options are limited. We aimed to assess resistance patterns and predict viral drug susceptibility among children with first-line antiretroviral therapy (ART) failure in Uganda. A cross-sectional analysis of children switching ART regimens due to first-line failure was performed at three clinical sites in Uganda. HIV-RNA determination and genotypic resistance testing on all specimens with HIV-RNA >1,000 copies/ml were performed. Major drug resistance mutations were scored using the 2011 International Antiviral Society–USA list. The Stanford algorithm was used to predict drug susceptibility. At the time of switch, 44 genotypic resistance tests were available for 50 children. All children harbored virus with nonnucleoside reverse transcriptase inhibitor (NNRTI) resistance [95% confidence interval (CI) 92–100%] and NRTI resistance was present in 98% (95% CI 88–100%). Forty-six percent (95% CI 30–61%) of children harbored ≥2 thymidine analog mutations. M184V was identified as the only NRTI mutation in 27% (95% CI 15–43%). HIV susceptibility to NRTIs, with the exception of tenofovir, was reduced in ≥60% of children. Ugandan children experiencing first-line ART failure in our study harbored high rates of dual-class and accumulated HIV drug resistance. Methods to prevent treatment failure, including adequate pediatric formulations and alternative second-line treatment options, are urgently needed.
Introduction
A
In resource-limited settings, exposure to nevirapine for the prevention of mother-to-child transmission (PMTCT) increases the risk of HIV drug resistance development and subsequent treatment failure of standard first-line regimens containing nonnucleoside reverse transcriptase inhibitors (NNRTIs). 9,10 Due to financial and technical constraints, virological monitoring to enable early failure detection is often not available. 1 Furthermore, the identification of resistance mutations using genotypic testing, which could aid appropriate sequencing of antiretroviral medication, is seldom performed. 8,11 As a consequence, children in resource-limited settings are empirically switched to a second-line regimen, typically containing ritonavir-boosted lopinavir and two new and/or recycled nucleoside reverse transcriptase inhibitors (NRTIs).
In Uganda, an estimated 200,000 children are HIV infected and the Joint Clinical Research Centre (JCRC) is an important provider of HIV care and treatment in Uganda. The national JCRC network has over 20 years of experience with ART, from conducting clinical trials to nationwide roll-out programs since 2003. In this cross-sectional study, we describe the resistance patterns among children failing first-line ART at three JCRC clinical sites, and predict viral drug susceptibility in order to gain insight into the optimal strategies for second-line therapy.
Materials and Methods
Study design and population
The Monitoring Antiretroviral Resistance in Children (MARCH) study is a multicenter prospective observational cohort of HIV-1-infected children who receive ART at three JCRC sites in Uganda. Site and cohort characteristics have been described previously. 12 Potential participants were informed of the study and screened for eligibility by the study staff. Children aged 12 years or below who initiated a first- or second-line ART regimen were enrolled. For the current analysis, only children requiring a treatment switch from first- to second-line ART due to treatment failure were included. Local definitions of immunological and virological treatment failure were in accordance with WHO guidelines, i.e., immunological failure was defined as developing or returning to age-related CD4 thresholds and virological failure was defined as a persistent viral load >5,000 copies/ml after at least 6 months of treatment. 13 For children receiving ART at JCRC, routine 6-monthly viral load monitoring is available. As JCRC serves as a referral clinic, children with suspected treatment failure based on clinical and/or immunological criteria are referred to JCRC for second-line ART. In these cases, targeted viral load testing was performed to confirm treatment failure. The ethical committees of JCRC in Uganda and the Academic Medical Center of the University of Amsterdam in The Netherlands approved the study protocol. The parent(s)/guardian(s) of all eligible children provided written informed consent. Children above the age of 8 years who were aware of their HIV status provided written informed assent. Sociodemographic and clinical data were collected using electronic case report forms, which were aggregated in a web-based database.
Procedures
Routine laboratory results including CD4 cell count and serum hemoglobin concentration were obtained from local laboratory records. Immunodeficiency for age was classified according to the 2010 WHO guidelines. 13 Plasma was sampled before switch to second-line ART (<30 days prior) and sent to a central reference laboratory for HIV-RNA testing. Genotypic resistance testing was performed on all specimens with HIV-RNA >1,000 copies/ml. For HIV-RNA determination, the COBAS Ampliprep/COBAS Taqman HIV-1 test (Roche, Branchburg, NJ) was used. For HIV-1 genotyping, an in-house sequencing method encompassing the whole of protease (PR) and codons 1–300 of reverse transcriptase (RT) with a Beckman Coulter CEQ 8000 analyzer (Beckman Coulter Inc., Fullerton, CA) was used. 14 Sequences were assembled and manually edited using BioEdit software version 7.1.3.0. Subtypes were determined using MEGA 5.10 software. Drug resistance mutations were scored according to the 2011 International AIDS Society-USA list. 15 HIV drug susceptibility for each participant was predicted using the Stanford algorithm, version 6.1.0, 16 and was categorized as susceptible, potential low-level resistance, low-level resistance, intermediate resistance, or high-level resistance. The proportions of virus with drug resistance mutations were calculated with 95% confidence intervals (CI). Nutritional status was assessed by means of the World Health Organization (WHO) Child Growth Standards: WHO Anthro version 3.2.2 (age 0–5) and WHO Reference 2007 for height and weight (age 5–19). 17,18 Underweight was defined as a weight-for-age z-score<−2 standard deviation (SD) and stunted as a height-for-age z-score<−2 SD. Categorical data were compared using the chi-square test. Analyses were performed using Stata version 10 (StataCorp LP, TX).
Results
Between January 2010 and July 2011, 369 children were enrolled in the MARCH study, of whom 50 (14%) children switched to second-line after first-line ART failure. The patients originated from Kampala (n=29), Mbale (n=18), and Fort Portal (n=3). The median age was 5.5 years old [interquartile range (IQR) 4.0–10.1] and 50% (25/50) of the participants were girls. The mother was the primary caregiver for most children (n=30, 60%); nine (18%) children were orphans. At the time of the child's enrollment, 26 (52%) mothers used ART. Overall, 23 (46%) children had a WHO stage 3 or 4 event at the time of switch, 9 (24%) children were underweight, and 25 (50%) children were stunted. Of the children with virological failure, 24 (50%) were also classified as immune-deficient based on their CD4 percentage or CD4 cell count for age. The median CD4% was 23.2 (IQR 14.0–30.0) in children<5 years old and the median CD4 cell count was 460.5 (IQR 86.0–645.5) in those >5 years old.
The decision to switch to second-line ART was based on virological failure in 48 (96%) and immunological failure in 2 (4%). For 25 (50%) children, a detectable viral load was measured at least 30 days prior to switch (range 30–297 days). First-line ART had been received for a median of 30 months (IQR 25.1–48.4). The most common first-line regimen consisted of zidovudine/lamivudine with either nevirapine (n=23, 46%) or efavirenz (n=12, 24%), followed by stavudine/lamivudine/nevirapine (n=10, 20%) and abacavir/lamivudine with nevirapine (n=3, 6%) or efavirenz (n=1, 2%). Single-drug substitutions within NRTI drug class were common (n=23, 46%). Thirteen (26%) children had been exposed to nevirapine for PMTCT.
Genotypic tests results were obtained for 44 (88%) children: four specimens had a plasma viral load below the sequencing threshold (1,000 copies/ml) and two specimens failed amplification. Subtype D was most commonly identified (n=19, 43%), followed by A (n=16, 36%), C (n=1, 2%), and various circulating recombinant forms (n=8, 18%). Drug resistance mutations were detected in all children with a genotypic test result. Within the NRTI drug class, M184V was present in 41 (93%) and multiple thymidine analogue mutation (≥2 TAMs) in 20 (46%). In 64% of children M184V occurred in combination with ≥1 TAM and in 27% the M184V was the only NRTI mutation identified. The most frequent NNRTI mutations were K103N (n=17, 39%) and G190A (n=16, 36%). Dual-class NRTI and NNRTI resistance was present in 43 (98%) children. Figure 1 depicts frequencies of individuals mutations by the type of NRTI or NNRTI used in the (most recent) first-line regimen. TAMs appeared more frequently when zidovudine was used, whereas K65R was less common (differences not significant; Fig. 1A). Multiple NNRTI mutations were observed more frequently when efavirenz was used as opposed to nevirapine (p=0.043; Fig. 1B).
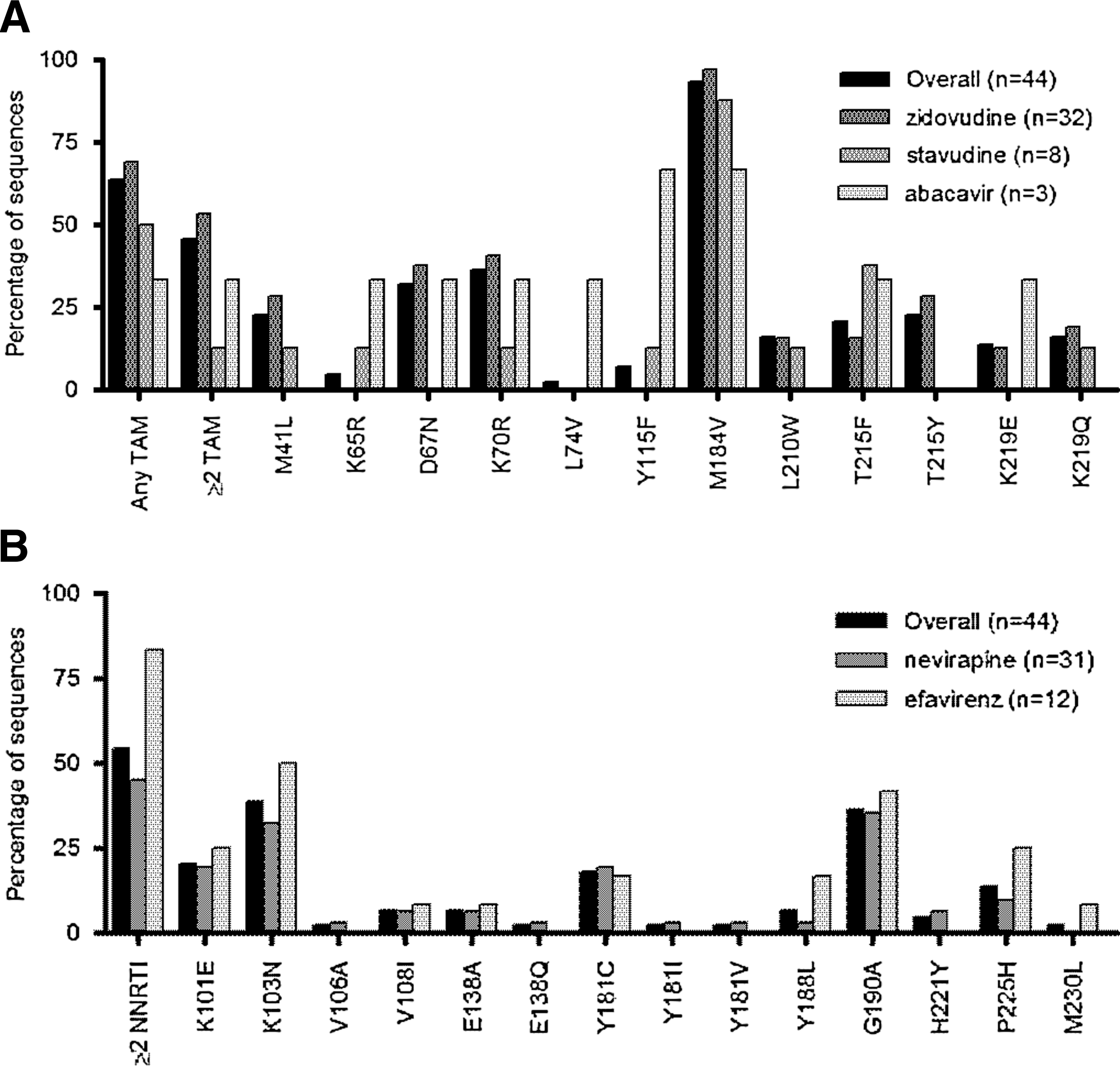
Frequencies of individual drug resistance mutations by nucleoside
Predicted HIV susceptibility to lamivudine and emtricitabine was reduced in nearly all (98%) children due to the high frequency of M184V (Fig. 2). For the other NRTIs, reduced susceptibility (i.e., low- to high-level resistance) was predicted for abacavir in 71% of sequences, zidovudine in 59%, stavudine in 68%, didanosine in 61%, and tenofovir in 39%. For the NNRTIs, reduced HIV susceptibility was frequently predicted for efavirenz and nevirapine (98%) and less frequently for the second-generation drugs etravirine and rilpivirine (52%). Reduced susceptibility was not predicted for any of the ritonavir-boosted protease inhibitors (PIs).
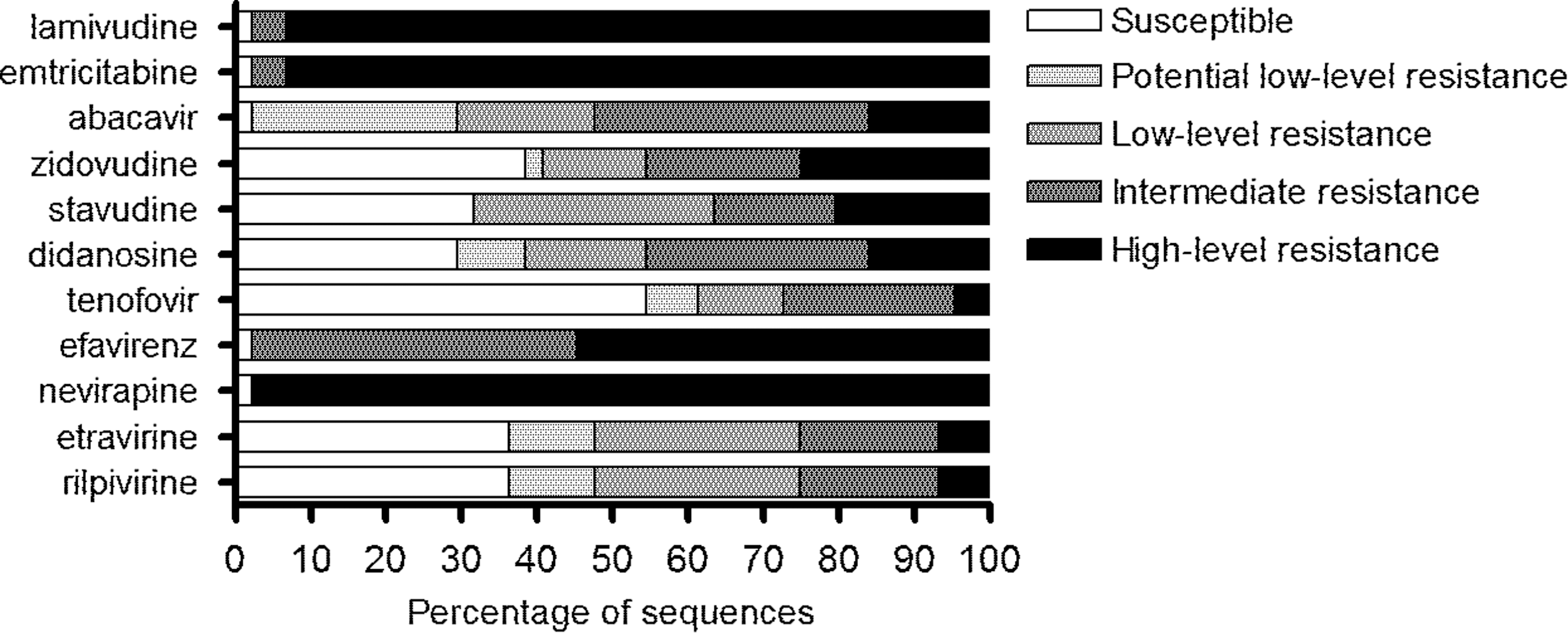
Predicted HIV susceptibility to nucleoside and nonnucleoside reverse transcriptase inhibitors in children with first-line antiretroviral therapy failure (n=44). Genotypic drug susceptibility was predicted using the Stanford HIVdb algorithm (version 6.1.0).
Discussion
This cross-sectional study among Ugandan HIV-infected children examined mutational resistance patterns after first-line ART failure and predicted the impact on second-line drug susceptibility. Nearly all children harbored dual-class resistance and multiple TAMs were detected in 46%. HIV susceptibility to NRTIs, with the exception of tenofovir, was severely reduced, jeopardizing the recycling of NRTIs in second-line ART. This issue is of particular concern in young children, for whom the number of licensed NRTIs is limited.
The most frequently observed mutation in our study, the M184V, associated with lamivudine and emtricitabine, delays resistance to zidovudine and stavudine. 19 Despite this increased susceptibility, 64% of patients harbored TAMs in combination with the M184V mutation. The rate of TAMs detected in our study is very high compared to previous reports among children in resource-limited settings where, as in Uganda, NNRTI-based first-line regimens are standard. 8,20 –23 This may be attributed to the fact that over half of children had a longer duration of treatment failure (i.e., longer than 1 month). Possibly, this reflects clinicians' reluctance to switch to second-line ART, due to regimen cost and subsequent loss of drug options. Also, some children were referred from outside clinics after experiencing clinical or immunological treatment failure. Further evidence supporting the relationship between prolonged duration of failure and drug resistance is provided by a Chinese study, in which children were continued on a failing regimen for nearly 2 years and high-level resistance occurred more frequently than in our study. 24
After failure of an NNRTI-based regimen in children, the WHO recommends a ritonavir-boosted PI, with a dual backbone of two new or recycled NRTIs, i.e., abacavir or zidovudine plus lamivudine. 13 Didanosine is proposed as a possible alternative to lamivudine. In our cohort, susceptibility to abacavir, zidovudine, and didanosine was preserved in 29%, 41%,and 39% of children, respectively. Therefore, the recommended NRTI backbone in second-line ART would be expected to have limited effect, while at the same time exposing children to considerable toxicity, especially when didanosine is used. 25 The most suitable NRTI to include in second-line ART would be tenofovir, which retains potency despite multiple TAMs. This drug has been associated with promising clinical outcomes in studies, 26,27 and its recent approval by the U.S. Food and Drug Administration (FDA) for children ≥2 years of age is particularly encouraging. 28 However, the risk of toxic effects to the kidneys and bone 26 will restrict its use in resource-poor settings, where monitoring is often limited. Therefore, constructing an active NRTI backbone for the children in this study becomes a major challenge.
An alternative strategy for second-line would be the use of boosted-PI monotherapy, which has shown conflicting outcomes in adults. 29,30 In children, this strategy has been evaluated in virologically suppressed children, with promising results. 31 PI monotherapy would have several advantages such as fewer pills, fewer drug interactions, and less NRTI-associated toxicity. However, before considering PI monotherapy in children after first-line ART failure, future research should investigate long-term outcomes and potential risks. In our study, we profiled the HIV susceptibility to second generation NNRTIs. Susceptibility to etravirine and rilpivirine is reduced in the presence of G190A and Y181C 32 and these mutations were present in 36% and 18% of children, respectively. Etravirine has shown promising results in children, 33,34 but is not yet licensed for use. For rilpivirine, no data in the pediatric population are yet available. 35 Clearly, the use of newer agents, such as integrase inhibitors, should be explored.
A limitation of our study is the small sample size. However, as resistance data on children is scarce, we believe that the results of this small cohort are important in informing clinicians in resource-limited settings when they are faced with the challenge of changing ART regimens without the aid of genotypic resistance testing. Second, a limitation related to the cross-sectional design is that the prevalent cases identified in this study may not be representative of all incident cases with virological failure, thereby limiting our data's generalizability to other pediatric populations.
This study reveals a high proportion of children with multiple TAMs and dual-class resistance after first-line ART failure. As a result, second-line regimens will primarily offer the benefit of the boosted-PI, and modest additional effect of the NRTI backbone. Deferred treatment switch is common in resource-limited settings 36,37 and results in increased mortality. 38,39 Therefore, the obstacles to second-line drug access and usage must be addressed by reducing costs and increasing the availability of new-generation antiretroviral medications with nonoverlapping resistance profiles and tolerable formulations for children.
GenBank Accession Numbers
GenBank accession numbers are JX181983–JX182026.
Footnotes
Acknowledgments
The authors are grateful to all study participants and their caregivers, doctors and nurses, and support staff at JCRC, PharmAccess Foundation and the Amsterdam Institute of Global Health and Development. At JCRC, we specifically thank Annet Nandudu, James Nkalubo, Isaac Egau, Lincoln Mugarura, and Leonard Bagenda from Kampala, Mary Kiconco, Michael Owor, and Florence Nambaziira from Fort Portal, and Mary Abwola, Fred Senono, Ronald Namisi, and Sylivia Nakusi from Mbale. At PharmAccess/AIGHD, we thank Cees Hesp and Robert Meester for database design.
C.K., T.F.R.W., R.L.H., V.M., and K.C.E.S. conceived the study. C.K., P.M., and V.M. established the MARCH cohort and supervised data collection. K.C.E.S. and J.K. contributed to implementation. K.C.E.S. analyzed the data and wrote the first draft of the manuscript. C.K., J.C., J.K., T.F.R.W., and R.L.H. critically reviewed the paper. All authors contributed to subsequent drafts and reviewed and approved the final manuscript.
The MARCH study is an initiative of JCRC and PharmAccess Foundation and was funded by the European & Developing Countries Clinical Trials Partnership (EDCTP). The funders had no role in the study design, data collection, data analysis, data interpretation, decision to publish, or writing of the report. The content of this publication is solely the responsibility of the authors and does not necessarily represent the official views of any of the institutions mentioned above.
Author Disclosure Statement
No competing financial interests exist.