
Abstract
To assess qualities and outcomes of women participating in a large, community-based HIV vaccine trial, the present study was conducted among female participants of the RV 144 prime-boost trial in Thailand from 2003 to 2009. Qualities of participation refer to complete vaccination, retention, and status change. Outcomes of participation refer to incident rate, adverse event, and participation impact event. A total of 6,334 (38.6%) women participated in the trial, of whom about 50% were classified as low risk and 11% as high risk. About 85% of participants completed four vaccinations and 76% were included in the per-protocol analysis of the on-time vaccination schedule. More women (88%) completed 42 months follow-up compared with men (85%). Women aged 21 and above had more adverse events compared to younger age groups. More women (5%) compared with men (3%) reported participation impact events (PIEs). High-risk women had more PIEs and a higher infection rate compared to the low-risk group. Complete vaccination and retention on last follow-up were more common in married women aged above 21, and being a housewife. Female volunteers showed the same qualities and outcomes of participation as males in the HIV vaccine trial. There was no statistically significant difference in vaccine efficacy between men and women, especially among the high-risk and married women. The study highlighted the important behavioral, social, and cultural issues that could be considered for future HIV vaccine trial designs.
Introduction
I
There are many challenges in HIV vaccine research and development such as absence of known immune correlates of protection and lack of validated animal models. Clinical trials on promising vaccine candidates require target participants, especially young adults including women and adolescents. 9 Young adults need to be included in trials as HIV incidence is higher in these groups, and they would benefit the most from an HIV vaccine. Women compared with men are more likely to become infected and to acquire asymptomatic sexually transmitted diseases, which increase the susceptibility to HIV. Some women resort to anal intercourse to prevent pregnancy, which further increases their risk of acquiring HIV. 10 While studies such as the VAX 004 (that tested the efficacy of AIDSVAX rgp120 B/B′) Phase III trial and Phambili using the MRK Ad5 HIV vaccine suggested that a vaccine might have a different efficacy among male and female subjects, we cannot say the same from STEP, where only one event occurred among women. 11 Social and behavioral issues such as lack of empowerment, inability to make a decision without consulting their partners, low educational status, discrimination, pregnancy, and stigma of being labeled as high risk for HIV prevent participation of women. 12,13
The prime boost HIV vaccine trial RV144 in Thailand from 2003 to 2009 enrolled 16,402 participants of whom 38.6% were women. Since HIV transmission was generally heterosexual in Thailand, the government wanted to develop a vaccine for the general population. The RV144 trial involved male and female participants of different sociocultural backgrounds from urban and semiurban areas of Thailand. The main objective of this study was to determine the qualities and outcomes of women's participation including their risk behavior and factors associated with compliance to study protocol, retention, pregnancy, as well as safety and efficacy endpoints.
Materials and Methods
Prime-boost HIV preventive vaccine trial (RV144)
The ALVAC HIV vaccine priming and AIDSVAX vaccine boosting efficacy trial published in 2009 was a double blind, placebo-controlled community-based, multisite trial at two Eastern Seaboard provinces of Thailand. 14 From 2003 to 2005, recruitment was conducted through local media (radio and television), booth presentations, community education, and health forums. Each participant signed an informed consent form. There were four immunization visits in the first 6 months of enrollment; follow-up was done every 6 months for 3 years. Participants who reported any adverse events and participation impact events (PIEs) were given risk reduction counseling. Follow-up was done until the event resolves. The health officer may assist by providing brochures/documents or necessary information, if required.
Blood was taken for HIV serology and immune responses. Treatment and care were administered, if necessary. All enrolled women used contraceptive methods in the initial 9 months of enrollment to avoid pregnancy. Institutional review boards in Thailand and the United States approved this study.
Data management and analysis
We collected demographic data on enrollment and each follow-up visit along with data on safety and primary efficacy endpoints. To estimate potential risks for infection and participation impact between the two groups, a behavior risk assessment questionnaire was used on each follow-up visit. For trial integrity, site investigators monitored any participation status change and loss-to-follow-up cases. Age stratification (≤20, 21–25, and ≥26) was based on available information on risk potential behavior and infection outcome. The occupation of female participants was classified into four groups based on their social roles and respective potential risk: housewife, student, sex workers including those who worked in the entertainment business, and others. We used self-response questionnaires to assess risk behaviors such as injecting drug use (IDU), risky sexual behaviors, and sexually transmitted disease (STD) at baseline and on scheduled follow-up. Baseline risk was categorized into three levels: (1) high risk (if study participants considered themselves as high risk or reported high-risk behaviors, e.g., needle sharing, multiple sex partners, sex work, STD symptoms); (2) low risk (if study participants perceived their risk as low, and in the previous 6 months reported 0–1 sex partners and no sex with sex workers, casual partners, same gender partners, HIV-infected partners, IDU partners, or a partner with multiple partners; reported no STD symptoms within 6 months of the study enrollment); and (3) moderate risk (study participants were neither low nor high risk). PIEs were categorized as positive and negative. The positive PIEs include employment/school benefits, personal relationship benefits, positive recognition, and medical and dental care benefits, whereas negative PIEs include problems at employment/school place, problematic personal relationships, discrimination, and health and life insurance problems.
Primary endpoint was diagnostic of HIV infection based on repeat positive results. Infection time was defined as the midpoint between the last negative result and the first positive result. Retention was defined as the time from enrollment until the final visit within the study period.
Pregnancy was not considered a participation outcome, but the percentage of women who became pregnant during the study was important as it may impact the study results scientifically, statistically, and ethically. A urine pregnancy test was performed prior to vaccination and during follow-up. Participants who became pregnant during the study period continued on with all scheduled visits, but were not given further immunizations. The date of current pregnancy was estimated from the self-reported date of the last menstrual period or the date when pregnancy was confirmed. However, many were incomplete due to uncertainties in recall. In this study, missing and incomplete dates of pregnancy were retrospectively estimated from the date of delivery.
In the main study, 14 populations were classified as intent-to-treat (ITT), modified intent-to-treat, and per-protocol. The intent-to-treat population was defined as all study participants randomized to either study arm during the accrual period. The modified intent-to-treat population was the ITT population except for seven HIV-infected subjects. The per-protocol population excluded participants who did not comply with the protocol-defined vaccination schedule, those not fully vaccinated, those who did not receive the correct randomized treatment (active or placebo), or those who were randomized and became infected during the immunization period. The analysis of this study was based mainly on ITT population.
Chi square test was used to compare different parameters between men and women. Changes in behavior on follow-up were determined using generalized estimation equation analysis. The characteristics and outcomes of female participants were analyzed based on their risks using logistic regression and Cox's proportional hazard regression. The analyses were exploratory in nature, and neither multivariate adjustment for confounders nor multiple comparisons were done.
Results
Difference between male and female participants
Among 16,402 enrolled participants, 6,334 (38.62%) were women residing in urban and semiurban communities, of whom about 12% were housewifes, 5% were sex workers or worked in the entertainment business, and about 6% were students. The majority of women (76.6%) classified as others (Table 1) include those who worked as laborers, farmers, government officers, etc. Baseline risk categories showed that about 50% women and 46% men were low risk while 11% women and 25% men were high risk. More women (81%) reported having a sexual partner compared with men (74%) but men tended to have more than one sexual partner (15% men and 4% women). Eleven percent of women had casual sex partners, of whom 42% used a condom. In contrast, about 29% of men had casual sex partners, of whom 25% used a condom.
Based on complete responses to each question.
Participation qualities include complete vaccination, retention, and status change (as shown in Table 2). There was no difference between men and women on participation qualities. About 76% of both groups were found in the per-protocol analysis of the on-time vaccination schedule. There were decreasing trends in retention in both groups; however, more women (88%) tended to retain and complete 42 months of follow-up compared with men (85%). The number of missed visits during the study also differed between women (17%) and men (21%). About 21% women and men changed their participation status due to varying reasons for each group.
There was no statistically significant difference between men and women in terms of infection regardless of type of analysis of population (Table 3). In the main study, 14 vaccine efficacy for different types of analyzed populations was not different between the two groups. Adverse events (AEs) as a safety indicator showed that women (71%) tended to have more AEs than men (66%). Men with AEs had more injury and complications, mostly due to motorcycle accidents (35% men compared to 15% women). As an indicator of social issues, women (5%) reported more PIEs compared to men (3%). Social issues included relationships in family and workplace and unpleasant comments from neighbors/co-workers. Measures were in place to address them, particularly among women (refer to Materials and Methods). Women (85%) had more problematic personal relationships compared to men (75%). In addition, men (8%) reported more problems with employment and education compared to women (6%).
Baseline risk behavior of women participants
Age-stratified analyses of baseline risk behaviors (Table 4) revealed that on enrollment about 2% women of all age groups were IDUs and about 0.7% had a history of being incarcerated. About 4% of women had more than one sexual partner and 11% had casual partners; more women aged ≥26 reported having sex with sex workers (2%). Workers in the sex and entertainment business appeared to have high-risk behavior at baseline: IDUs (2%), more than one partner (32%), casual sex partners (43%), sex with sex workers (16%), and had a history of STDs (10%). Women with different marital status reported divergent risk behaviors. Divorced, separated, and widows tended to have high-risk behavior, of whom 28% had a casual partner, 17.5% had more than one partner, and 6.5% had sex with sex workers. Women with different educational levels also reported diverse risk behaviors with risk behaviors that tended to decrease as educational level increased. In women with no formal education, about 5% were IDUs, 26% had casual sex partners, 5% had more than one sex partner, 3% had sex with sex workers, and 3% were incarcerated. Among women classified as high risk, about 6% were IDUs, 38% had casual sex partners, 15% had more than one sex partner, 7.5% had sex with sex workers, 19% had a history of STDs, and 1% were incarcerated.
IDU, intravenous drug user; STD, sexually transmitted disease; SW, sex worker.
Differences in vaccine efficacy among risk groups cannot be determined because of the small sample size of these groups in the RV 144 trial.
Change in risk behavior among women participants
Women aged ≤20 did not significantly change their risk behaviors over time except for having less casual partners; those aged 21–25 significantly reduced having a casual partner, having more than one partner, and having sex with sex workers, but were at increased odds for incarceration; and those aged ≥26 also had similar decreased sexual risk behaviors but increased incarceration as shown in Table 5. Most of the risk behaviors among women aged ≤20 did not significantly change due to the fact that the percentages of those who had such risks at baseline were quite low (1–4%). That is why only having a casual partner with a high percentage at baseline (11.5%) is the only risk that showed a significant reduction.
The change in risk behavior appeared to be similar for each occupation risk group. Almost all occupation risk groups had significantly less sexual risk behaviors. Similarly, for women with different marital status, most reported significantly decreased sexual risk behaviors. Women with no formal education did not significantly change their risk behaviors except for fewer casual partners compared with women who had primary and secondary education. Women who were low risk and medium risk appeared not to significantly change their risk behavior except for decreasing the odds of having regular and casual partners; however, the low-risk group had increasing incarceration. The high-risk group reported decreasing odds in all risk behaviors except being IDUs.
Participation qualities among women participants
More women aged ≥26 (82%) followed by those aged 21–25 (76%) had vaccine completion compared with those aged ≤20 (72%). Being a housewife and married showed higher odds of vaccine completion. Vaccine completion was highest among housewives (82%), among students and other occupations (76–77%), among sex workers (72%), and among different marital status: married (79%), single (74%), and ever married (72%). Baseline risk behaviors appeared not to be associated with vaccine completion but showed an increasing trend—low risk (78%) and moderate and high risk (76%).
With retention at month 42, housewives (97%) had the highest retention followed by students and sex workers (92–93%) and others (94%). Being married (96%) had the highest retention followed by others (93%). Baseline risk behaviors did not seem to be associated with retention. Using a failure curve (Fig. 1), no significant trend was found among different baseline risk categories even though low-risk groups had lower discontinuation toward the last follow-up visit. Discontinuation appeared to increase during the vaccination period (first 6 months) and the period close to the scheduled final visit.
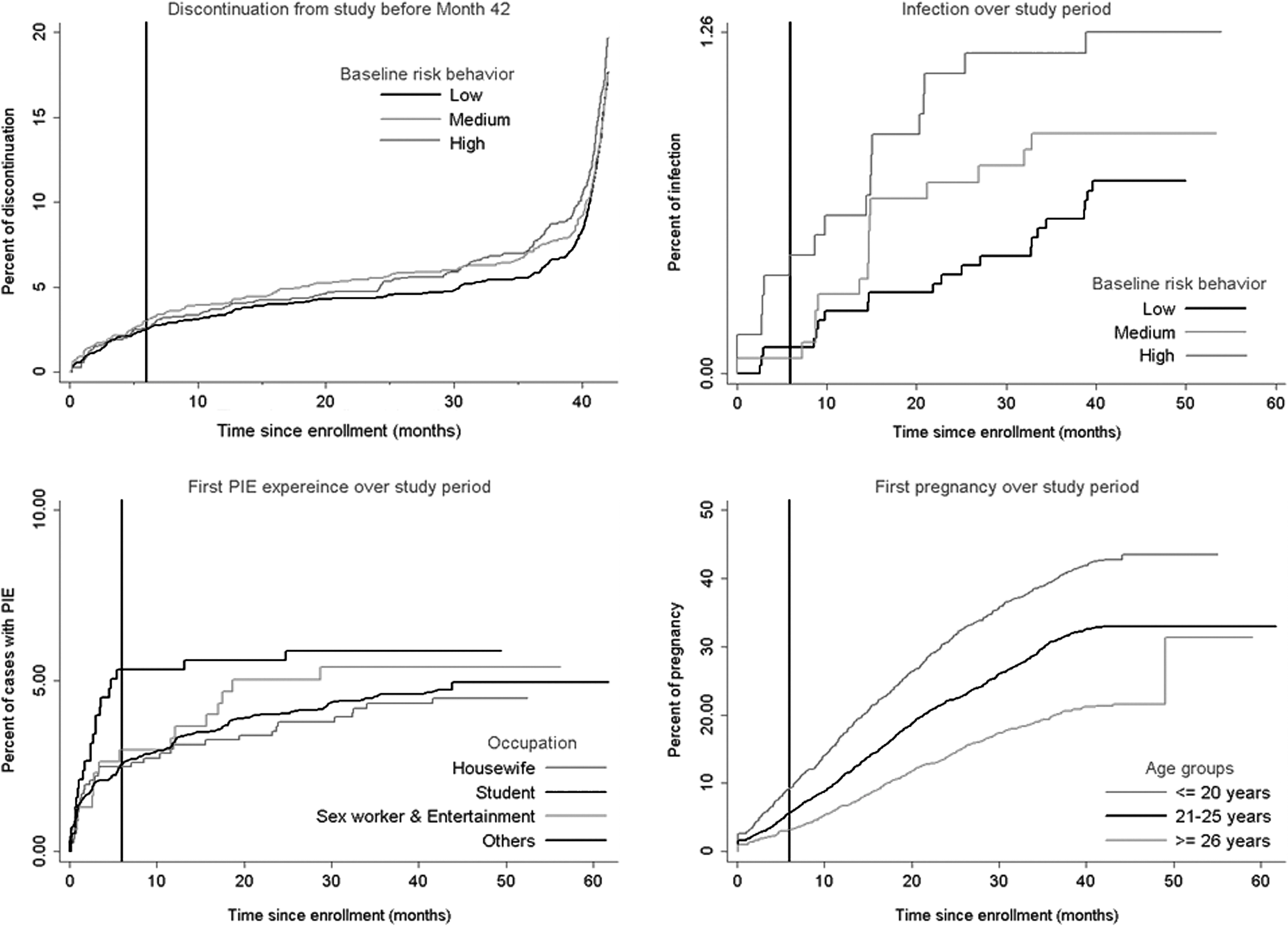
Time to participation events during study period.
Participation outcomes among women
There was no statistically significant association between infection and demographic characteristics except ever-married women (1.64%) were more infected than single women (0.55%). Baseline risk categories were not significantly associated with infection even though increasing trends of risk levels were observed in both infection rates (Table 6) and time-to-infection (Fig. 1). A total of 12,345 adverse events occurred in 4,472 of 6,334 (70.60%) women. Those aged 21–25 (72%) and ≥26 (71%) had significantly higher odds of AEs compared to women aged ≤20 (68%) (Table 6). Three hundred and thirty-six of 6,334 women (5.30%) had 370 PIEs, of which 28 (8.33%) had two PIEs. High-risk women had more PIEs compared to low-risk women. There was an increasing trend on risk levels in both proportions of PIEs (Table 6) and time-to-first PIE (Fig. 1). In 336 initial PIEs, 210 events (62.50%) occurred during the vaccination period.
PIE, participatory impact event; AE, adverse event.
Pregnancy during the study period
The pregnancy rate was quite high in Thailand among the study age groups. A total of 1,922 of 6,334 women (30.34%) became pregnant during the study period, of whom 255 (4.03%) and 13 (0.21%) had second and third pregnancies, respectively. The highest rate of pregnancy was in women aged ≤20 (41%), followed by the 21–25 (31%) and ≥26 (21%) aged groups. Pregnancy within the first 6 months of the study was noted in 362 of 1,922 women (18.83%), of whom 22.32% were aged ≤20 followed by 21–25 (17.76%) and ≥26 (15.48%). There was no difference in pregnancy rates between vaccinated and placebo recipients.
Discussion
The percentage of women participating in clinical trials varies by year, phase, and product type. 6 In this trial, almost 40% women were enrolled and retained. This was large enough to be considered a good representative of HIV risk groups in Thailand, where men are at higher risk than women. Factors associated with women's participation vary by community settings and so future HIV prevention and/or treatment programs targeting women should address their needs within individual communities. 15 –18
This trial utilized gender-sensitive and risk-based communication media and conducted community outreach programs targeting women, therefore encouraging their participation. Results of this trial suggest that men and women were comparable in most aspects. Similar to other clinical trials, most of our study participants were young with a high school level of education and lived in urban and semiurban areas. This study showed results similar to other trials involving heterosexual transmission with men having more than one partner, more casual and high-risk sex partners, and less use of condom for protection. 19 –21
Compared to their respective subgroups, a higher proportions of sex workers and ever married women had more than one sex partner, with casual and high-risk partners, and a history of STDs. Housewives and students had about 10% casual sex and a 3% history of STDs despite being perceived as a low-risk group. Most women who were IDUs (4%) with a history of incarceration had neither formal education nor primary education. Risk behaviors in most subgroups significantly decreased within 36 months of follow-up. These may be due to intensive counseling by research teams and preventive measures on each follow-up visit. Similar results were obtained in other studies using the same product (AIDSVAX) alone, one of the two vaccines in the RV 144 prime-boost protocol. 22,23
Vaccine completion in men and women were about 85%, and both groups were in compliance with the protocol immunization schedule for about 75% of the time. More women (88%) were retained compared with men (85%). In addition, 17% women had missed visits compared to men (21%). Subgroup analysis showed married women aged 21 and above and being a housewife had more retention on last follow-up visit and with complete vaccination compared to other groups. Recruitment and retention of women are more complex and expensive than men due to differences in socioeconomic status and expectations and requirements for participation.116 Women may be reluctant to address their sexual behaviors, restrain from being pregnant, and burdened with family care. 24 –26 Several strategies for study compliance and retention include consented home visits, weekend and off-hour clinic visits, consented confidential visits when incarcerated, and community advocacy. Other studies used telephone reminders for missed visits, giving certificates of completion on final visits, and a high level of acknowledgment for participating in the study. 27 –31
Results of the main study showed that 132 subjects were diagnosed with HIV infection (56 in the vaccine group and 76 in the placebo group), therefore providing preliminary evidence that an HIV vaccine regimen has the potential to prevent infection in the modified ITT analysis. 14 Similar findings were obtained in our study when male-to-female infection rates and vaccine efficacy were compared.
Also, in the main study most local and systemic reactions to the vaccine were mild to moderate; at least one adverse event was reported in 69.4% of subjects in the two study groups, with similar severity in both groups. 14 It was found that women had at least one AE more than men. Most of the AEs of men were related to injuries sustained from motorcycle accidents (35% events in men compared to 15% in women) because participants were young and motorcycles were the main mode of transportation. The second most frequent AEs (33% men and 37% women) were upper respiratory infections. The subgroup analyses of women participants revealed that those aged above 21 had more AEs than younger women. However, with regard to the safety of preventive vaccines, 32 this vaccine regimen was still considered to be safe because there were very few vaccine-related AEs with no difference in AEs between placebo and vaccine recipients.
The HIV vaccine trial poses an unusual challenge for both investigators and volunteers as study participants may experience discrimination and social stigma. 16,27,32,33 In several studies, discrimination ranged from <5% to 30%. 34 –40 Only about 4% of participants reported PIEs in this study, a finding that was similar to another trial in Thailand. 40 This could be due to differences in the background and culture of the study community as well as different procedures in assessing PIEs among participants. While men and women were concerned that participation could potentially damage their personal relationships, the concern was greater for women, who were more likely to be economically dependent. 28 In this study, women experienced more PIEs than men, and women who were in the high-risk group had more PIEs than those in low-risk groups. Similar to other studies, the most frequent PIE reported in this study was personal relationship problems, especially for women. 35,37 In addition, female student participants experienced stigma during the first 6 months after enrollment. This could be due to lack of knowledge and misunderstanding about HIV/AIDS at the early phase of the trial, as PIEs were much less frequent after that period. In this study, PIEs were rated as not serious with minimal impact on their daily lives, a finding that was similar to other vaccine efficacy trials conducted in Thailand. 37,40 Positive PIEs reported in this study include positive recognition and personal relationships. 24,38,40
Pregnancy is one of the reasons why some women do not want to participate in a study. Guidelines from UNAIDS recommend that women who are pregnant, potentially pregnant, and breast-feeding should be eligible for enrollment in HIV preventive vaccine trials, both as a matter of equity and because women are at high risk of HIV infection in many communities. 41 However, most investigators were reluctant to enroll pregnant and breast-feeding women because of concerns about health risks from the candidate vaccine. Still, pregnancy rates during HIV prevention trials were high. 19,42 As women participants in this study were young, almost one-third became pregnant during the trial. Women aged ≤20 had higher pregnancy rates compared with other groups. Over 25% of pregnant women were either single, students, or ever married. These were groups with less risk for pregnancy. Further investigation regarding this issue should be considered as a study on hormonal contraceptives showed that although women in vaccine trials frequently used prevention methods, misconceptions and their incorrect use might have led to inconsistent use resulting in undesired pregnancies. 19
Women's participation in HIV vaccine trials represents an important challenge due to women's susceptibility to infection and sociocultural and legal inequality. Other barriers in recruiting and retaining women in trials include age, occupation, education, and marital status. To achieve women's participation in this trial, several strategies were developed and fully implemented by the research teams. They considered the rights and needs of these women while encouraging community involvement and representation.
In conclusion, female volunteers showed the same qualities and outcomes of participation as males in the HIV vaccine trial. The analyses of gender issues and women's participation in this study revealed behavioral, social, and cultural indicators that could be used for future trials. Data collected from the target population may be of great help in developing effective educational materials, resolving ethical issues, and finding useful sociocultural indicators for a successful HIV vaccine trial design.
Footnotes
Author Disclosure Statement
No competing financial interests exist.