
Abstract
Prompt entry into care and retention in care are critical for improving outcomes among HIV-infected individuals. This study identified factors associated with HIV-infected adolescents who delayed entry into HIV care (DEC) after diagnosis of HIV or who fail to remain in care afterward (FRC). We reviewed clinical, demographic, and social data from the records of 202 HIV-positive adolescents (13–21 years old) infected via high-risk behaviors. Strength of association between clinical and social factors and DEC or FRC were estimated with log-linear regression models. DEC occurred in 38% (76/202) of adolescents. Factors independently associated with DEC were unstable residence (RR 1.5; CI: 1.0–2.1) and, compared with less education, college attendance (RR 2.1; CI: 1.5–3.2). FRC occurred in 29% (52/177) of adolescents established in care. Compared with college attendees, high school students (RR: 4.5; CI: 1.2–17.3) and those who dropped out of high school (RR: 4.0; CI: 1.1–15) were more likely to FRC. Compared with adolescents with private insurance, adolescents without insurance (despite access to free care) were more likely to FRC (RR: 2.8; CI: 1.1–6.9). Controlling for sex, adolescents with children were more likely to FRC (RR: 1.8; CI: 1.0–3.1). Interventions to avoid DEC that target HIV-infected adolescents with unstable residences or those diagnosed while attending college are warranted. Among patients engaged in care, those with only high school education or without insurance—which may be markers for socioeconomic status—need additional attention to keep them in care.
Introduction
F
Delay in treatment has a profound effect on the patient's quality and length of life. 5,6 Adolescents are a vulnerable population: they underutilize nonemergency health services, 7 –9 are less likely to be insured or to have a medical home, 9,10 and are at a higher risk for delays in diagnosis and treatment than adults. 11 There are few consistent predictors of delayed or poor engagement in medical care after diagnosis of HIV among adult populations. 12 –22 We reviewed clinical data for adolescents infected with HIV via high-risk behaviors to identify associations with delayed entry into HIV care (DEC) and failure to remain in care (FRC) after linkage to care had been established. These factors may identify potential targets for interventions designed to improve engagement and retention in care.
Materials and Methods
Study population
We reviewed the clinical records for 266 adolescents (13–21 years old) infected with HIV via high-risk behaviors, attending a large, urban, comprehensive pediatric/adolescent HIV clinic (St. Jude Children's Research Hospital) from January 1998 to October 2009. We excluded patients transferring from other HIV care clinics, as well as pregnant and postpartum adolescents who received initial care at an obstetrical clinic.
Definitions and variables
The standard of care at our institution is to schedule a clinic appointment within 7 days after referral of a patient newly diagnosed with HIV. Patients are referred directly from the local health department, primary-care clinics, local hospitals, blood banks, community testing drives, and occupational screenings. If a referred patient misses the initial appointment, contact letters are sent to the address of record 2, 3, and 4 weeks after the missed appointment. DEC was defined as failing to appear for care after a period of >2 months from the initial referred appointment date. We chose >2 months as our definition of DEC because the county health department's early intervention service conducts a home visit for each patient who fails to appear within 2 months after the initial referral to HIV care. Patients were scheduled to be seen at least once every 3 months. Patients were considered to have started engaging the clinic once they appeared for two consecutively scheduled visits. Patients were considered to be engaged in care in a given 1-year period if they appeared for care in each quarter. After having engaged in care for at least 1 year, FRC was defined as neither appearing in the clinic nor collecting medications for ≥6 consecutive months and missing at least one scheduled visit during that time. Appointments that were rescheduled at least 1 day in advance and were subsequently kept did not count as missed appointments. We excluded patients who had not been enrolled in care ≥12 months from the FRC analysis (this analysis required a minimum of 18 months of observation time from the initial clinic visit).
We abstracted demographic, clinical, and social variables from the clinical record. A sexually transmitted disease (STD) diagnosis (other than HIV) was considered concurrent to the HIV diagnosis if the STD diagnosis was made within 1 month before or after the HIV diagnosis. Residence was defined as unstable if the permanent address changed ≥3 times in the preceding 12 months or there was no permanent address (e.g., shelter, vehicle, or street). We documented whether the patient lived with guardians, a spouse or committed partner, or alone; whether the patient had custody of a child and whether that child was HIV infected; whether another person in the home was known to be HIV infected; level of education; medical insurance (regardless of Ryan White assistance); current employment; alcohol usage; drug usage; and history of arrests. We collected CD4 count and viral load upon entry into care and the most recently recorded values upon loss to follow-up or the end of the follow-up period.
Statistical analysis
Descriptive characteristics for DEC and FRC cohorts were calculated and compared using t-test, Wilcoxon rank sum test, or chi-square test, as appropriate. We calculated unadjusted relative risks to measure the association between various factors and the two outcomes of interest: DEC and FRC. Those factors with a significance ≤0.15 in the bivariate analysis were included in the multivariate log-linear regression model. We estimated the adjusted relative risks using PROC GENMOD (Poisson distribution, log link, and a repeated statement with unstructured covariance). Analyses were performed using SAS 9.2 (SAS Institute, Inc., Cary, NC).
Results
Demographics and HIV disease characteristics
We excluded 64 adolescents whose disease was diagnosed while they were pregnant, transferred from another clinic, or lacked outcome data (Fig. 1). All 202 remaining patients were included in the cohort analysis for DEC. We excluded an additional 24 patients enrolled <18 months from the FRC analysis (Fig. 1). The baseline characteristics of the 202 adolescents included for analysis are detailed in Table 1. There was no correlation between DEC and FRC (p=0.93).
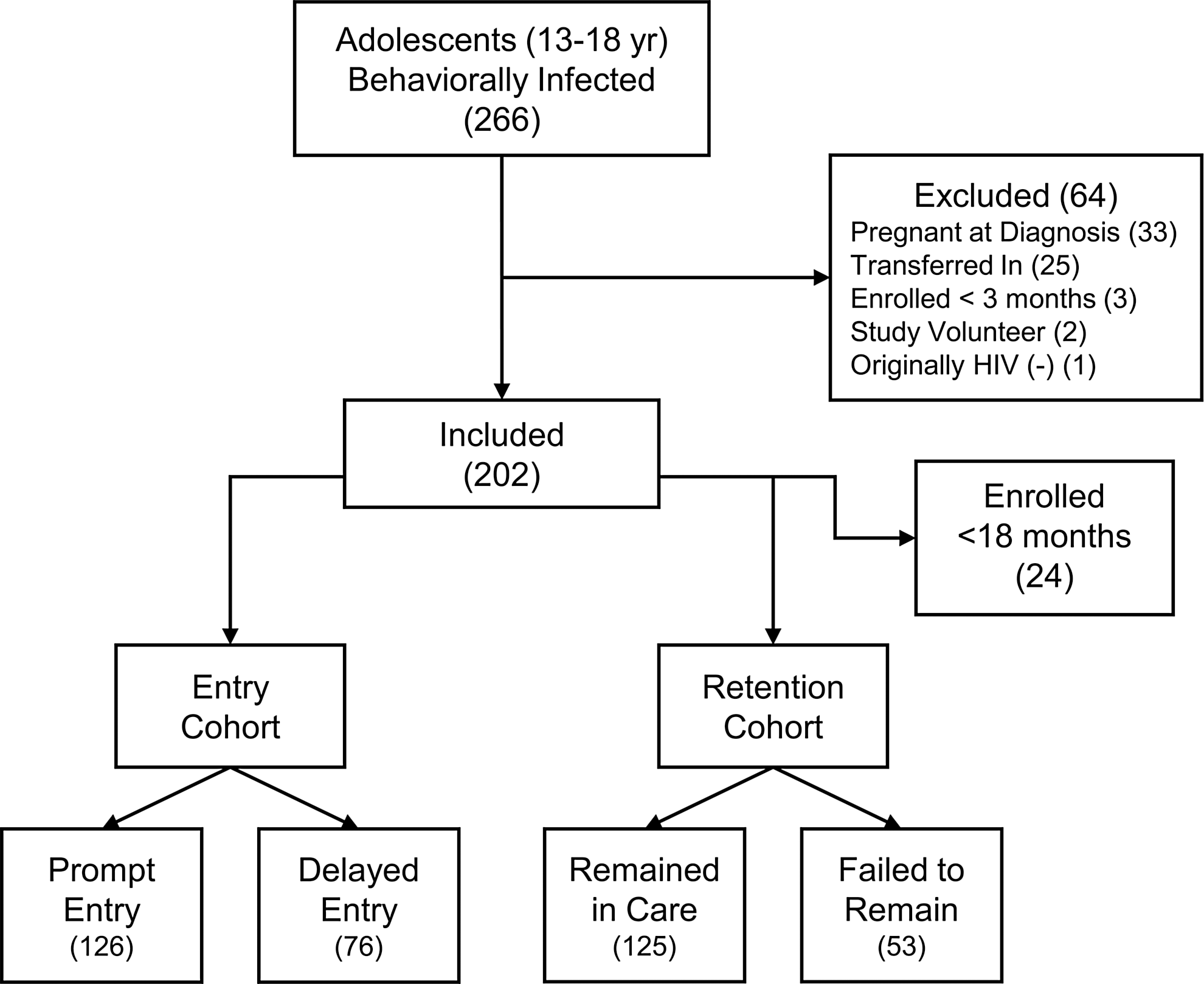
Subject assignment for adolescent entry and retention cohorts.
Twenty-four subjects were excluded from analysis for enrollment time <18 months.
Overall, the cohort was predominantly African-American (95%). Males were predominantly identified as men who have sex with men, and females were identified solely as heterosexual (Table 1). DEC occurred for 38% (76/202) of HIV-infected adolescents. The median delay from HIV diagnosis to entry into care for these patients was 123 days (IQR: 79–230). Those who experienced DEC were similar to those who promptly entered care based on initial clinical stage, age at enrollment, or driving distance from their primary residence to the HIV clinic (Table 1). Baseline CD4+ cell count, baseline viral load, most recent CD4+ cell count, change in CD4+ cell count, and change in viral load were not significantly different between those who DEC and those who entered care promptly (Table 2). FRC occurred for 29% (52/177) of adolescents. There was no significant difference in the baseline CD4+ cell count, baseline viral load, or most recent CD4+ cell count between those who remained in care and those who failed to do so (Table 2). Patients who remained in care showed slightly greater improvements in CD4+ cell count and significantly larger reductions in viral load at last visit than those who failed to remain engaged in care (Table 2).
Twenty-four subjects were excluded from analysis for enrollment time <18 months.
Factors associated with delayed entry into HIV care
Patient factors associated with DEC are shown in Table 3. Lack of a stable residence, being enrolled as a student in college, and residing within 5 miles of the HIV clinic were independently associated with DEC (Table 3). There were no significant associations between DEC and diagnosis of an adjustment disorder (p=0.08), hospitalization at the time of HIV diagnosis (p=0.21), regular alcohol use (p=0.35), regular drug use (predominantly marijuana) (p=0.36), concurrent diagnosis of a sexually transmitted disease (p=0.74), HIV testing location (p=0.77), or medical insurance status (p=0.85). The mode of HIV transmission was not associated with DEC (p=0.85), and there were no documented intravenous drug users in this cohort.
Relative risk (RR) was adjusted for unstable residence, living alone, education, and distance from clinic.
Factors associated with failure to remain engaged in HIV care
Patient factors associated with FRC are shown in Table 4. Students enrolled in college, once engaged in care, were less likely to fall out of HIV care than were high school students and those who did not complete high school. The association remained after adjusting for having a dependent child, sex, and type of insurance (Table 4).
Relative risk (RR) was adjusted for insurance status, custody of a child, gender, and education.
Discussion
The prevalence of DEC was higher (38%) in our adolescent cohort than the overall rate reported in a comprehensive meta-analysis of adult studies (31%) 12 ; however, most of these studies used a period of ≥3 months as their criteria for DEC, which might decrease the likelihood that a study would classify a patient as delayed. 20,23 There are limited published data on characteristics predictive of DEC. Our study found adolescents with an unstable living situation and those whose disease was diagnosed while they were in college to be associated with a delay >60 days between initial diagnosis and entry into HIV care. One study found that minority race, sex, insurance status, and nonlocal residence were predictive of HIV-infected adults delaying entry into care. 20 Similar to our findings, age and whether they were referred by a clinician were not associated with delay. 20 There was no association between sex and delay in our cohort. The effect by sex in the previously published study was found only among those of white race; there was no effect by sex in the minority patients. 20 As our cohort was predominantly African-American, this finding is consistent. However, in our cohort, sex was also almost completely confounded by sexual orientation.
We did not find a significant association between DEC and manner of referral (provider versus self) or insurance status. However, our clinic provides care, including antiretroviral medications, without charge to the patient. This practice may obviate any effect insurance might have had and limits our ability to generalize this finding. Distance from the HIV clinic had an unexpected, paradoxical positive association with DEC. Adolescents residing within 5 miles of the HIV clinic were almost twice as likely to experience DEC as those who lived farther away. This predictor was independent of accessing our clinic's free transportation services, which collects patients within a radius of 30 miles around the clinic. This finding differs from an adult study that found residing farther away from the clinic was weakly associated with DEC. 20 Distance between residence and clinic may be serving as a surrogate for other factors. The residential blocks within a 5-mile radius of our clinic have extremely high rates of poverty (median: 54%) in the county than other regions (median: 7.7%). 24 However, this finding shows that residential proximity and free transportation services do not guarantee engagement in care.
Two interesting factors associated with DEC that were identified in our study were unstable residence and college attendance. Adolescents living in unstable residences were more likely to delay their entry into care. The disruptions imposed by a transient lifestyle or concurrent, unmeasured socioeconomic factors may interfere with scheduling and accessing medical care. Patients whose HIV was diagnosed while they were attending college were four times more likely to delay entry into care. This finding may be reflective of the lack of a guardian's influence in the adolescent's decision making, inadequate health services, denial, or delays induced by the demands of an academic schedule, or initial fear of stigma. 25,26 These findings suggest a potential point of intervention at HIV testing centers. Health care providers and HIV testing centers should take steps to identify the at-risk adolescents by screening for unstable residence (i.e., frequent changes of address or a history of “couch surfing”) or college attendance and devote additional efforts to introduce the adolescent to HIV care services (e.g., having a nurse or social worker from the local HIV care clinic visit the patient on the day of diagnosis). College campuses should take steps to reduce the stigma associated with HIV, including a sexual health and HIV prevention curriculum for orienting students, faculty, and administration, and student health clinics should develop a structured system for linking students into local HIV care promptly after diagnosis.
Once the adolescent has engaged in care, the factors associated with continued engagement shift. Thirty percent of our cohort fell out of care for a period of 6 months or more after initially engaging in care. While this rate is lower than that described in a large meta-analysis of studies on retention among adults (41%), 12 it is a significant proportion of our adolescent patients, and even a single missed visit has been associated with an increased risk of mortality. 27 Patients enrolled in college were less likely to fall out of HIV care once engaged than were high school students and those who did not complete high school. Another study of adults found heterosexual practice to be predictive of falling out of care. 15 We identified a similar trend in our analysis, but the strength of association did not meet statistical significance. Four adult studies found younger age to be directly associated with FRC, 14 –17 but we found no association with age. However, the age range in our cohort is likely too narrow for this effect to be detected.
Drug use, typically intravenous drug use, was associated with poor engagement in HIV care in four previous studies. 13,17,18,21 Adolescents in our cohort who regularly used any kind of drug were no more or less likely to fall out of care. However, marijuana use was so ubiquitous in our cohort that it is difficult to detect a true difference, if one were to exist, between its use and FRC.
Our study supports the findings of three studies in adults in which having insurance was associated with remaining engaged in care and those with public insurance were less likely to remain engaged in care than those with private insurance. 17,20,22 As our clinic provides medical care without charge to the patient, whether or not the adolescent was covered under insurance should not influence his or her ability to access the clinic. This measurement may be confounded by unmeasured risk factors related to socioeconomic status and the ability to obtain insurance.
Once an adolescent had been engaged in care, those who attended college were more likely to remain engaged in care. One study found that an education beyond high school was associated with better compliance with appointments, 16 while another found no association. 14 In our cohort, although adolescents enrolled in college were more likely to delay their entry into care, we speculate they may have had a better understanding of the concepts explained at the first HIV care visit or have greater self-motivation, thereby leading to ongoing compliance with medical appointments without gaps.
Our study is limited by its retrospective design conducted with a convenience sample of adolescents enrolled in care at an HIV specialty clinic. We were limited to factors that were documented in the clinical record. Second, subjective assessments of reasons for delaying entry or concerns about attending the HIV clinic were not uniformly documented and were difficult to categorize. Qualitative studies may prove to be more effective than quantitative ones in elucidating modifiable barriers associated with delayed entry into care or failing to remain engaged in care. Finally, our study did not collect data on adolescents who were never linked to care or those who were referred but never engaged in care.
Adolescents living in stable homes were less likely to delay accessing HIV care, whereas those enrolled in college were more likely to delay. Further investigation of factors associated with delay is warranted, but our study suggests that interventions should be made at the time of diagnosis to target adolescents from unstable residences and college students with HIV to ensure prompt linkage to HIV care services. Once engaged in care, college students were less likely to fall out of care. Prospective, qualitative studies may shed additional light on factors associated with delay or failure to remain in care. Efforts to improve linkage to and retention in care, coupled with routine HIV screening, can benefit both the patient and society through improved individual health and reduced ongoing transmission in the population.
Footnotes
Author Disclosure Statement
No competing financial interests exist.