
Abstract
The links between sexual violence, genitoanal injury, and HIV are understudied but potentially significant for understanding the epidemic's disproportionate impacts on young women and girls, particularly in sub-Saharan Africa, other hyperendemic areas, and conflict-affected regions. A Scientific Research Planning Meeting was convened by the Social Science Research Council at the Greentree Foundation in New York, March 19–20, 2012, bringing together an interdisciplinary group of researchers, clinicians, and policy makers to identify knowledge needs and gaps in three key areas: (1) the role of genitoanal injury on HIV transmission, acquisition, and pathogenesis; (2) the influence of sex and age-related anatomic characteristics on HIV transmission, acquisition, and pathogenesis; and (3) the role of heterosexual anal intercourse in HIV transmission. This article reflects the consensus that emerged from the Greentree Meeting regarding priority scientific research questions in these three areas, associated data collection and measurement challenges and opportunities, and implications for policy and practice.
Introduction
T
This White Paper reflects a consensus agenda for research, policy, and practice that resulted from a Scientific Research Planning Meeting on Sexual Violence and HIV, convened by the Social Science Research Council on March 19–20, 2012 at the Greentree Foundation in New York (hereafter referred to as the “Greentree Meeting”). The Greentree Meeting was sponsored by the National Institutes of Health, Office of AIDS Research; the Joint United Nations Programme on HIV/AIDS (UNAIDS), and UN Action Against Sexual Violence in Armed Conflict. The Greentree Meeting brought together basic, clinical, epidemiological, and social science researchers and policy makers with the goal of generating new insights about the physiology of sexual violence and its role in HIV transmission, particularly among women and girls. b The meeting objectives were to (1) examine what is known about the physiology of sexual violence and its role in HIV transmission, acquisition, and pathogenesis; (2) specify the sex and age-related anatomic and physiological factors that increase the risk of HIV transmission, acquisition, and pathogenesis during the maturation of the female genital and anal tracts throughout the reproductive cycle; and (3) develop a research agenda to explore unanswered questions. This article summarizes the consensus reached through the Greentree Meeting regarding priority research questions, associated data collection and measurement challenges, and implications for policy and practice. The summary Report of Proceedings and the review papers developed for the Greentree Meeting are in preparation for publication in a Special Issue of the American Journal of Reproductive Immunology.
Research Priorities
The role of genitoanal injury in HIV transmission, acquisition, and pathogenesis
The biology of HIV sexual transmission is not well understood. 17 Most scientific studies of vaginal transmission use ex vivo cervicovaginal tissue models that cannot reproduce the cellular interactions that occur in vivo. Nor can primate models, which deliver HIV or SIV atraumatically through intravaginal and intrarectal inoculations, recreate the microabrasions and injuries that occur naturally from vaginal and anal intercourse, or more excessively from forced and violent sex.
In creating a physiological pathway that facilitates viral transmission, genitoanal injury may significantly increase the per-act probabilities of heterosexual transmission in specific contexts (Fig. 1). 18 –20 Normally, the lower female reproductive tract, which constitutes the outer cervix and vaginal walls, is composed of a multilayer stratified epithelium that gives greater protection against injury and infection than the single-cell columnar epithelium lining the upper reproductive tract (endocervix and uterus). A number of factors can disrupt this otherwise protective barrier and immune protection in the female genital tract. These include ulcerations and inflammation due to sexually transmitted infections (STIs), as well as proinflammatory immune factors associated with exogenous 21 –23 and endogenous 24 –26 hormones and sex/semen. 27,28 Cervical and vaginal lesions, microabrasions, inflammation, and immaturity of the female reproductive tract (cervical ectopy) may modulate susceptibility to HIV infection since damaged areas provide open access to the subepithelial structures where HIV-1 target cells predominantly reside. 29 The columnar epithelium of the upper reproductive tract and that associated with ectopy may render these sites more susceptible to injury than the lower genital tract. Very little is known about the compounding effects of genital trauma in environments where multiple cofactors are present, such as STIs, cervical ectopy, and the use of hormonal contraception.
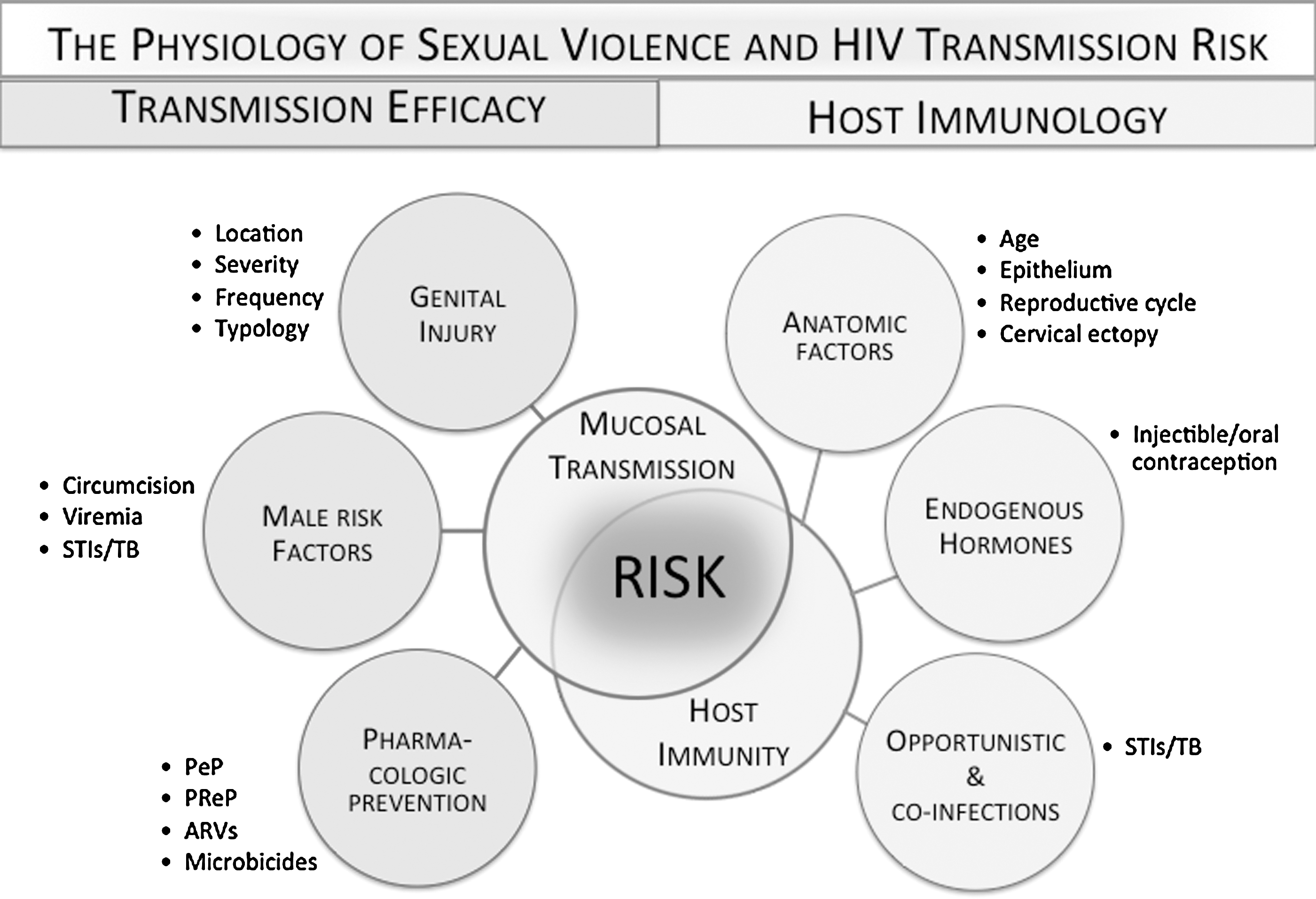
The physiology of sexual violence and HIV transmission risk.
Inflammation, abrasions, and injury can result from both forced and consensual sex, 30,31 although most studies associate higher rates (up to three times higher) of injury with sexual assault. 32 –34 Rates of reported injury in cases of forced sex vary immensely, with studies estimating between 32% 30 and 94%. 34 Sexually assaulted prepubescent girls and adolescents may sustain more injuries than adults due to the hymeneal, vaginal, or cervical lacerations that occur naturally with sexual debut. 35 –37 The severity, frequency, location, and patterns of injury will vary in relation to many factors, including age, the degree of force or coercion, the use of objects, the perpetrator's characteristics and motivation, and exposure opportunities. c But injury reporting may not capture these differences. The absence of standard definitions, classifications, reporting, and collection protocols means that injury detection will vary according to the individual examiner, clinical capacity, legal requirements regarding sexual assault reporting, and the techniques used. d In many cases, clinical reports and related research do not specify anal injuries or inflammation, both significant risk factors for HIV transmission. 38 –40,e
The physiological effects of intimate partner violence (IPV) on the immune system are also underresearched. An emerging literature points to immune system effects that result from altered hypothalamic, pituitary, and adrenal gland interactions and the suppression of Th1 cell cytokine production (which fights bacteria and viruses). 7 Posttraumatic stress disorder (PTSD) and depression—comorbidities associated with intimate partner violence—can also contribute to immune suppression, proinflammatory responses, and faster progression to AIDS. 41 –43
Priority scientific research questions identified by the participants included the following:
1. What is the impact of genitoanal injury on the female reproductive and anal tracts? How do these effects vary in relation to different developmental stages of the female reproductive and anal tracts?
2. How are genitoanal injuries defined and measured; and is there a “threshold” that can be as
3. How do the immunological and other effects of intimate partner violence increase the risk of HIV transmission and progression?
4. What is the contribution of genitoanal injury to HIV transmission, acquisition, and pathogenesis when multiple cofactors are present, such as STIs and hormonal contraception?
The influence of sex and age-related anatomic characteristics on HIV transmission, acquisition, and pathogenesis
UNAIDS estimates that 40% of new adult infections each year are among those 15 to 24 years of age. 44 Of all young people living with HIV—some five million—75% are in sub-Saharan Africa 45 and 71% of these are female (Table 1). 46 Yet epidemiological and behavioral models of HIV transmission risk have been unable to explain why young women between 15 and 24 years in sub-Saharan Africa, who average only 2.3 sex partners in their lifetime, are two to eight times more likely than men to be HIV positive. 47 –51 While HIV remains low in the United States, similar patterns emerge when examining the rates of other STIs among adolescent girls as compared to boys, particularly chlamydia, gonorrhea, and human papillomavirus (HPV). Although young people aged 15–24 years represent only 25% of the sexually experienced population in the United States, they acquire nearly half of all new STIs. In the United States, young women aged 15–19 experience the highest rates of STIs, followed closely by women ages 20–24. 52 In 2010, young women between 15 and 19 years of age were three times more likely than boys to have chlamydia. 53
UNAIDS: Report on the Global AIDS Epidemic, 2010.
Age-related anatomic, biological, and physiological risk factors amplify acquisition probabilities among young adolescent women. During adolescence, sex hormones play a central role in regulating immune protection against HIV acquisition throughout the course of the menstrual cycle and the maturation of the female reproductive tract. Adolescent and adult cervices differ strikingly in their epithelial composition; the corollary differences in mucosal immune function may increase adolescent susceptibility. 54,55 Cervical ectopy, which occurs naturally in young women, may affect HIV risk by extending columnar cells that normally line the inside of the cervical canal to its outer surface, providing easier access to the submucosa where most of the HIV target cells reside. Additionally, sexually active healthy adolescents may undergo active epithelial maturation in the cervix over relatively short periods of time; this increased cell proliferation can enhance susceptibility to HPV infection, an STI that might also contribute to enhanced HIV risk. 56 HSV-2, which increases HIV transmission, is another common STI often acquired during adolescence. 57,58
Another understudied risk factor in women's susceptibility to HIV acquisition is female genital mutilation/cutting (FGM/C), which occurs among young girls and before puberty. f Although there is little evidence linking FGM/C and HIV transmission, the few studies that have been carried out point to the potential role of nonsterile/soiled equipment, transfusion with potentially contaminated blood following hemorrhage, reproductive tract infections that increase risk of HIV acquisition, and inflammation/abrasion of vaginal tissue from the physical injury of FGM/C. 59 Other potential risk factors include earlier sexual debut, polygamous relationships, male preference for “uncut” women (therefore looking elsewhere for partners), and higher rates of anal intercourse (AI) (due to difficult and painful vaginal intercourse and as a strategy to prevent pregnancy). 60
A major limitation in assessing age-related biological and physiological determinants of HIV susceptibility among young women and adolescent girls is the absence of comparative and age-disaggregated data. Gaps in data result from the exclusion of adolescents from trials for ethical and regulatory reasons and the significant underreporting of child sexual assault as a mode of transmission. Age categories used in data collection are also inconsistent across institutions within and across regions of the world, and most do not distinguish children, adolescents (ages 13–18), or young adults (ages 19–24). The World Health Organization (WHO) defines young people as between 10 and 24 and most AIDS data are reported among the age group 18–49. For the U.S. Centers for Disease Control and Prevention (CDC), the only reportable transmission categories for children are either perinatal or “other,” which includes hemophilia, blood transfusion, or risk not identified. 61
Priority scientific research questions identified by the participants included the following:
1. How do changes in the cervical and vaginal epithelium affect immune responses to genital injury and HIV acquisition risk before, during, and after adolescence, throughout different stages of the reproductive cycle, and among postmenopausal women?
2. How do the physiological and social cofactors of forced and early sex contribute to adolescent vulnerability and increase the risk of HIV acquisition over the longer term?
3. What are direct and indirect pathways linking female genital mutilation/cutting and HIV transmission and acquisition, namely in relation to immune protection and the development of the female genital tract?
The role of heterosexual anal intercourse in HIV transmission
The role of heterosexual AI in the epidemiology of HIV is poorly understood and likely underestimated. 62 In developed countries, transmission probability for unprotected receptive anal intercourse has been estimated at 1.4%, or about 18 times the risk for receptive vaginal intercourse. 63,64 This is primarily due to the inherent fragility of the rectal mucosa, the immune environment and the chronic inflammatory state of that compartment. 65 While AI has historically been considered a significant risk factor for men who have sex with men, its prevalence and frequency are rarely reported among heterosexual population and little is known about the age-related and anatomic, physiological, or hormonal differences between the male and female anal tracts and how these differences might influence transmission risk.
From the limited available data, forced and consensual AI occurs across populations, age groups, and countries with some studies reporting that up to 20% and more of selected populations in America, Africa, and elsewhere have ever engaged in AI. 63 Condom use is often lower in heterosexual anal sex than in vaginal sex. 66,67 Some studies show that women are coerced or forced to have anal sex by their partners and in the context of transactional sex. 68,69 In cases of sexual assault, reports of forced anal penetration range between 13% and 22.5%. 33,36,70 Rates of AI may also be higher among women who have undergone the most extreme form of female genital mutilation/cutting, which makes vaginal intercourse very difficult or painful. 71,72
The potential contribution of heterosexual AI to HIV transmission among women is not known but could have significant implications for the usage, safety, and delivery mechanisms of vaginal and rectal microbicides and other HIV prevention modalities. A modeling exercise by Boily et al. 73 shows that even low levels of unprotected AI (5%) can reduce the effectiveness of vaginal microbicide interventions in heterosexual populations by 17–39% over 25 years.
Priority scientific research questions identified by the participants included the following:
1. Are there age-related and anatomic, physiological, or hormonal differences between the male and female anal tracts and, if so, how do they influence transmission risk?
2. What is the prevalence, frequency, and relationship characteristics and dynamics of unprotected AI and its contribution to HIV acquisition? What proportion is forced and how does this influence the severity of injuries and the likelihood of unprotected intercourse?
3. What are the implications of heterosexual anal sex for dual usage, safety considerations, and delivery mechanisms for rectal and vaginal microbicides?
Data Collection and Measurement Challenges and Opportunities
The Greentree Meeting identified four key data collection and measurement challenges and opportunities that must be addressed in order to expand the knowledge base in the critical areas of research noted above:
▪
▪
▪
▪
Sexual Violence, Genitoanal Injury, and HIV: Implications for Policy and Practice
Heterosexual transmission accounts for the largest proportion of HIV prevalence worldwide: approximately 23.5 of the 34.2 million people currently living with HIV are believed to have acquired it through heterosexual intercourse. But the shift of epidemic monitoring from prevalent infections to incidence has focused attention and resources on the smallest subpopulations with the highest proportion of new HIV cases. In epidemiological models, these “key populations” typically refer to sex workers, people who inject drugs, and men who have sex with men, although the term also applies to others at highest risk of HIV exposure in a specific setting. 45,74 –77,g In contrast, very little is known about the epidemiological or social risk factors that drive “heterosexual transmission,” a term that is often and misleadingly characterized as “low-risk.” In model estimates of incidence and prevalence, heterosexual transmission is in fact a highly aggregated category of risk and exposure that reveals very little about who is most at risk or why and often includes people who are bisexual in their practices (if not their identity). Epidemic models define the population sexual structure according to a number of behaviorally defined risk groups, e.g., “low-risk” heterosexual refers to men and women reporting only one sexual partner in the year preceding the survey from which size estimates were obtained. 74,h In this context, risk is not differentiated by the type of sexual interaction (vaginal or anal), age-related characteristics, or age discrepancy in relationships (e.g., child sexual assault or early marriage), or the use of force (e.g., incest, gang rape, conflict-related rape), or relational typologies (e.g., survival sex, levirate marriage, polygamy, monogamy).
As a mode of exposure—i.e., a biological pathway for viral transmission—the genitoanal injuries that result from sexual transmission—forced and consensual—may help explain the significant underestimation of per-sex-act probabilities associated with heterosexual transmission and the disproportionate rates of infection among young women as compared to young men. Research, policy and practice must give greater attention to the interaction between the physiological and social cofactors that increase the vulnerability of young adolescent women, and to the potential impact of sexual violence prevention on reducing HIV incidence within and across different subpopulations.
The Greentree Meeting proposed three priority directions for policy and practice:
Conclusions
The contribution of sexual violence and genitoanal injury to HIV transmission and acquisition has not yet been fully understood or integrated into the global AIDS response, even though it plays a potentially significant role in the development of HIV epidemics, particularly among young women. Causal pathways between sexual violence and genitoanal injury and HIV infection are complex, and involve a range of biological, behavioral, and social factors that must be explored simultaneously. Participants at the Greentree Scientific Research Planning Meeting identified a robust agenda for interdisciplinary research, cognizant of its applications to program and policy, that should be pursued imminently.
Greentree Meeting Participants
Kathryn Anastos, Albert Einstein College of Medicine; Letitia Anderson, UN Action Against Sexual Violence in Conflict; Judy Auerbach, Independent Consultant; Marie-Claude Boily, Imperial College; Jacquelyn Campbell, Johns Hopkins University; Michele Decker, Johns Hopkins University; Khady Diouf, Brigham and Women's Hospital; Kristin Dunkle, Emory University; Anneka Ehrnst, Karolinska Institute; Aissatou Gaye-Diallo, Universite Cheikh Anta DIOP; Nancy Glass, Johns Hopkins University; Serigne Magueye Gueye, University Cheikh Anta DIOP; Catherine Hankins, Amsterdam Institute for Global Health and Development; Betsy Herold, Albert Einstein College of Medicine; Amelia Hoover Green, Drexel University; Thomas Hope, Northwestern University; Mazeda Hossain, London School of Hygiene and Tropical Medicine; Jantine Jacobi, UNAIDS and Global Coalition on Women and AIDS; Rowena Johnston, The American Foundation for AIDS Research; Charu Kaushic, McMaster University; Jennifer F. Klot, Social Science Research Council; Kathryn Laughon, University of Virginia; Souleymane Mboup, Universite Cheikh Anta Diop; Velda Mushangwe-Mtisi, University of Zimbabwe Medical School; Ragnhild Nordås, Peace Research Institute Oslo; Carel Pretorius, Futures Institute; Sengeziwe Sibeko, University of Oxford; Papa Salif Sow, University of Dakar; Christina Thobakgale, University of KwaZulu-Natal; Fulvia Veronese, National Institutes for Health; Charlotte Watts, London School of Hygiene and Tropical Medicine; Alex Welte, South African Centre for Epidemiological Modelling and Analysis, Stellenbosch University; Charles Wira, Dartmouth Medical School.
The authors would also like to recognize the following people who contributed to developing this agenda through personal communications:
Sally Blower, University of California, Los Angeles; Gina Brown, National Institutes for Health; Judith Bruce, Population Council; Cynthia Buckley, University of Illinois; Mardge Cohen, Stroger Hospital; Susan Cu-Uvin, Brown University; Berthilde Gahongayire, UNAIDS; Geoff Garnett, the Gates Foundation; Simon Gregson, Imperial College; Timothy Hallett, Imperial College; Gillian Holmes, UN Office for Disaster Risk Reduction; Quarraisha Abdool Karim, University of KwaZulu-Natal; Rupert Kaul, University of Toronto; Leo Kenny, UNAIDS; Alan Landay, Rush University Medical Center; Ahuka Ona Longombe, University of Kisangani and Panzi General Referral Hospital, Democratic Republic of Congo; Daniela Ligiero, President's Emergency Plan For AIDS Relief; Michele Moloney-Kitts, Together for Girls, UNAIDS; Nelly Mugo, International Clinical Research Center and Kenyatta National Hospital; Susan Newcomer, National Institutes for Health; Nawal M. Nour, Harvard Medical School; Melissa Robbiani, Population Council; Joseph Ruminjo, Engender Health; Samira Sami, (CDC); Barbara Shacklett, University of California, Davis; John Stover, Futures Institute; Nertila Tavanxhi, Marleen Temmerman, World Health Organization; Basia Tomczyk, CDC; Jim Turpin, National Institutes for Health; Ron Veazey, Tulane Medical School; Gilbert Wembodinga, Panzi General Referral Hospital, Democratic Republic of Congo.
Footnotes
Acknowledgments
Funding for this meeting was provided by the National Institutes of Health, Office of AIDS Research; UNAIDS, UN Action Against Sexual Violence in Armed Conflict and the Greentree Foundation. The authors wish to thank SSRC research assistants and meeting organizers, Miranda Berry, Patience Mungwari, and April Pei.
Author Disclosure Statement
No competing financial interests exist.
a
This meeting explored the physiological cofactors of sexual violence that increase the risk of HIV acquisition and progression among women and girls. Violence—sexual, verbal, and physical assault—can also be a consequence of disclosing HIV status.
b
It is recognized that different forms of sexual violence and exploitation take place among men and women, boys and girls. The focus of this meeting, however, was given to understanding the implications of genitoanal injury for HIV transmission risk, acquisition, and pathogenesis among girls and women in the context of both consensual and nonconsensual sex.
c
For example, during the conflict in eastern Congo, so many cases of traumatic fistula caused by systematic, violent gang rape were reported that the destruction of the vagina is now considered a war injury and is recorded by doctors as a crime of combat.
d
e
Although there is no standardized reporting, most genital injuries identified in nonconsensual sex occur in the posterior fourchette, hymen, labia minora, cervix, urethrea/periurethra, anus, vagina, and rectum.
f
For the purpose of this discussion, FGM/C was considered as an anatomic risk factor (rather than a form of sexual violence) that might exacerbate risks resulting from genital trauma.
g
Key populations are those that are key to the dynamics of the HIV epidemic in a geographic area and key to the response. Effective HIV prevention with respect to key populations is built on a foundation of meaningful engagement and involvement of these populations.
h
High-risk heterosexual refers to men and women reporting more than one sexual partner in the year preceding a given survey. The efficacy of reporting mechanisms of sexual violence vary considerably. It is less likely that a forced sexual encounter—which may pose a high risk of exposure—is included among the number of sexual partners that are self-reported by sexual assault survivors