
Abstract
To investigate the effect of a year of highly active antiretroviral therapy (HAART) on immune reconstruction and cytokine production in HIV/AIDS patients, 35 AIDS patients were recruited for HAART treatment and 35 healthy volunteers were assigned as controls. The dynamic changes in HIV load, blood T cell subset counts, as well as interleukin (IL)-12, interferon (IFN)-γ, and interferon-inducible protein-10 (IP-10) levels in AIDS patients were evaluated before HAART and at 6 and 12 months after therapy. Our results revealed that HIV virus load in HIV/AIDS patients was reduced below the detectable limit after patients received 6 months of HAART. CD3+CD4+, CD4+CD45RA+62L+, and CD4+CD45RO+ T cells were found to be significantly decreased in HIV/AIDS patients compared to the healthy controls, but increased after HAART. CD3+CD8+ and CD8+CD38+ cells were found to be increased in HIV/AIDS patients but decreased after HAART. Plasma IL-12 and IFN-γ levels were lower but IP-10 level was higher in AIDS patients compared to controls. HAART significantly improved IL-12 and IFN- γ levels but reduced IP-10 level in AIDS patients (p<0.01). CD4+CD45RA+62L+ and CD4+CD45RO+ T cells were positively correlated with plasma IL-12/IFN-γ levels (p<0.05), but negatively correlated with plasma IP-10 level. However, CD3+CD8+ cells were negatively correlated with plasma IL-12 and IFN-γ levels, but positively correlated with IP-10 level (p<0.05). HAART benefits HIV/AIDS patients by not only inhibiting virus replication but also by contributing to immune reconstruction, such as restoring subsets of T cells and adjusting cytokine production in HIV/AIDS patients.
Introduction
A
Numerous studies have demonstrated that HAART significantly increases CD4+ T cell percentage, CD4+ T cell count, and CD4+/CD8+ T cell ratio while decreasing the CD8+ T cell count. 4 However, it is commonly observed that some patients with significant restoration of CD4+ T cells still developed drug resistance and have a poor prognosis. 5 This observation implies that the number of CD4+ and CD8+ T cells may not be an accurate indicator of the reconstitution of the immune system in AIDS patients who received HAART. Recently, the number of central memory cells (CD4+CD45RA–) among the CD4+ T cells and the activated CD8+ T cells (CD8+ CD38+) is believed to be a better indicator of immune restoration in patients who received HAART than the absolute number of CD4+ and CD8+ T cells alone. 6 Moreover, the study by Vigano et al. demonstrated that CD4+CD45RA+CD62L+ (naive) and CD4+CD45RO+ (memory) T cells were increased after HAART with a greater increase in naive T cells compared to memory T cells. 7 In particular, a high CD38+ ratio seems to be an early sign of noncompliance and/or the development of drug resistance. 2 However, how HAART regulates T cell subtypes and their functions is still unclear.
Interleukin (IL)-12 has been shown to exert a potent immunostimulatory effect on certain helper T cells as well as on cytotoxic T lymphocytes (Tc) and natural killer (NK) cells. 8 IL-12 also stimulates lymphocytes and NK cells to secrete interferon (IFN)-γ. 9 Chronic HIV infection decreases the production of IL-12 and IFN-γ. 10 Importantly, IL-12 was able to stimulate the differentiation of Th0 cells into Th1 cells and increase Th1 cell activity. 11 Interferon-inducible protein-10 (IP-10) is a newly discovered chemotactic factor, which can be produced by various cells. IP-10 can activate Th1 cells and macrophages. 12 Moreover, IP-10 has potent chemotactic activities and predominantly targets activated T lymphocytes and NK cells. 13 Although the changes in IL-12, IFN-γ, and IP-10 concentrations in AIDS patients who received HAART have been reported, their dynamic changes as well as their correlations with CD4+ and CD8+ T cell subsets in HAART-treated AIDS patients have rarely been reported.
In this study we observed the dynamic changes in CD4+ and CD8+ T cells subsets and IL-12, IFN-γ, and IP-10 levels in HAART-treated HIV/AIDS patients before therapy and at month 6 and 12 after therapy. We further analyzed the correlations of CD4+ and CD8+ T cells subsets with IL-12, IFN-γ, and IP-10 levels after HAART.
Materials and Methods
Case selection
Patients
Thirty-five HIV-1/AIDS patients (13 females and 22 males) with an average age of 40±9.8 years were recruited at the Hunan Provincial Center for Disease Control and Prevention from January 2010 to January 2011. Thirty-five healthy volunteers who were screened as HIV negative (15 females and 20 males) with an average age of 33±15 years were recruited at the same time as uninfected controls. All AIDS patients were diagnosed according to the “AIDS Diagnose and Treatment Guidelines” (National Ministry of Health, China, 2006). All patients were confirmed to be HIV-1 positive with CD4+ T cells lower than 350/mm3, liver and kidney function in the normal range, and no hypertension, coronary disease, diabetes, stroke, opportunistic infections (including tuberculosis and other pathogenic infections), or malignant tumor. All recruited HIV/AIDS patients were antiviral drug-naive. This study was approved by the Ethics Committee of Central South University. Signed informed consent forms were obtained from all subjects who participated in the study.
HARRT regimen
All 35 AIDS patients were treated with the conventional HARRT regimen: zidovudine, 0.3 g per dose, twice per day; lamivudine, 0.3 g per dose, once per day; and nevirapine, 0.2 g per dose, once per day and changed to twice per day 2 weeks later if no side effects were observed. However, three patients were changed from nevirapine to efavirenz (EFV), 0.6 g per dose, once per night in week 4 due to side effects.
Follow-up visits
Patients were scheduled for routine clinic visits. Peripheral blood (PB) viral load examination, T lymphocyte and subset amount, IL-12, IFN-γ, and IP-10 levels were tested every 6 months up to a year.
Endpoints
The primary endpoints are the amount of peripheral blood CD4+ and CD8+ T cells, and their subsets, and the levels of peripheral blood IL-12, IFN-γ, and IP-10.
Laboratory tests
Sample collection
Eight milliliters of fasting blood was collected in an anticoagulant tube from each subject. Plasma and peripheral blood mononuclear cells (PBMCs) were separated with lymphocyte separation reagents. Plasma was frozen at –80°C.
FACS analysis of T cell subsets
Two- to three-color flow cytometry was applied to quantify T helper cells (Th, CD3+CD4+), naive Th (CD4+CD45RA+62L+), and memory Th (CD4+CD45RA−) cell subsets, as well as cytotoxic T cells (Tc, CD3+CD8+) and the activated Tc (CD8+ CD38+) cell subset in fresh blood samples. T lymphocytes and their subsets were identified using Bitest or Tritest kit (BD Biosciences, San Jose, CA) by following the manufacturer's manual. The absolute counts (cells/μl) of lymphocytes in erythrocyte lysed whole blood were determined by flow cytometry as previously described. 14
ELISA detection of IL-12, IFN-γ and IP-10
Plasma IL-12, IFN-γ, and IP-10 levels were detected by ELISA kit (Bio-Rad Laboratories, Richmond, CA). Sample absorbance was obtained with a microplate reader, and data were analyzed with CurveExpert 1.3 software (Microsoft, Redmond, WA).
Statistical Analysis
Data were analyzed using the SPSS 13.0 software, and the results were shown as mean plus or minus standard error of the mean. Groups were compared using the independent sample matching t test, while the Spearman rank test was used for correlation analysis. A p<0.05 was considered statistically significant.
Results
HAART effectively reduced the viral load in HIV/AIDS patients
Before HAART treatment, serum HIV-RNA copy was 4.62±1.09×106 copies/ml detected by real time PCR. Six and 12 months after HAART treatment, the HIV-RNA copies dropped below the detectable limit (data not shown), which confirmed the successful inhibition of HIV viral replication in the patients under HAART treatment.
HAART does not affect liver or kidney function in patients
Liver function as evaluated by serum ALT and TB levels was comparable between HIV/AIDS patients and controls (Fig. 1a). HAART did not affect liver function in HIV/AIDS patients over 12 months after treatment when tested at months 6 and 12 although 3 out of the 35 patients showed symptoms of decreased appetite and rash early during treatment, and the symptoms disappeared after they were switched from nevirapine (NVP) to EFV. Kidney function as evaluated by serum BUN and CR levels was also within the normal range in HIV/AIDS patients before or after HAART treatment as compared to controls (Fig. 1b). These results suggested that HAART has no significant effect on liver or kidney functions.
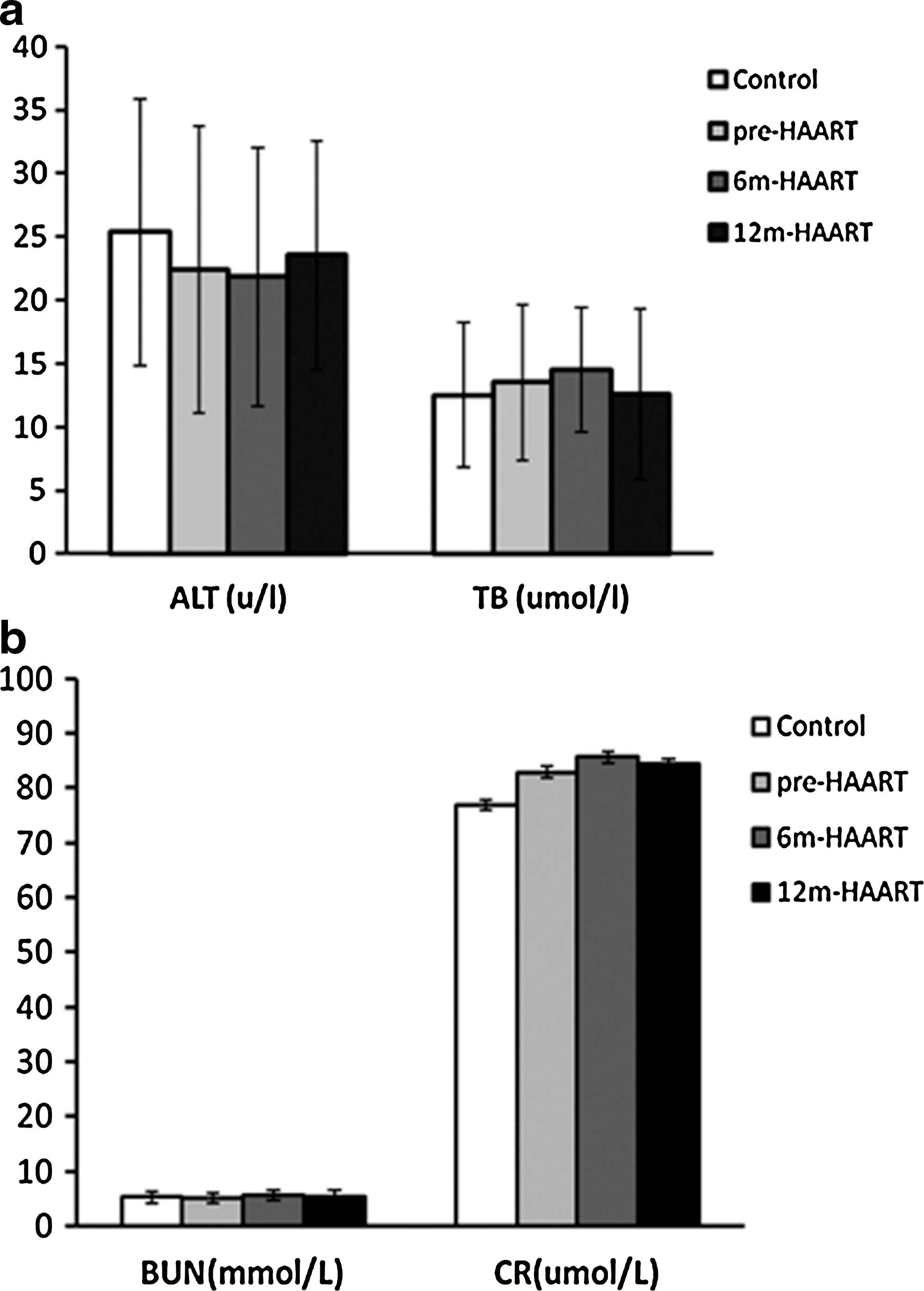
Comparison of liver and kidney function between HIV/AIDS patients and control.
HAART resulted in T cell subsets reconstitution in HIV/AIDS patients
The constitution of T cell subsets in HIV/AIDS patients was quite different from the healthy control group. CD3+CD4+, CD4+CD45RA+62L+, and CD4+CD45RO+ T cell counts were significantly lower, while CD3+CD8+ and CD3+CD38+ cell counts were significantly higher in HIV/AIDS patients compared to controls (Table 1, p<0.05). Six months of HAART significantly up-regulated the population of CD3+CD4+ and CD4+CD45RO+ cells, but not CD4+CD45RA+62L+ cells in the patients compared with their pretreatment values, probably due to the slow regeneration rate of CD4+CD45RA+62L+ cells. After 12 months of HAART treatment, CD3+CD4+, CD4+CD45RA+62L+, and CD4+CD45RO+ cells in the patients increased significantly compared to their pretreatment values (Table 1, p<0.05), although the counts were not completely restored compared to healthy controls (p<0.05). However, CD3+CD8+ and CD3+CD38+ cells were markedly increased in patients before HAART compared to controls (Table 1, p<0.05); 12 months of HAART treatment significantly reduced the population of CD3+CD8+ and CD3+CD38+ cells in HIV/AIDS patients compared to their pretreatment values (p<0.05), although the treatment did not completely normalize CD3+CD8+ and CD3+CD38+ cell counts (Table 1). We further analyzed the ratio of restoration of T cell subsets in AIDS patients after 12 months of HAART. The CD3+CD4+, CD4+CD45RA+62L+, and CD4+CD45RO+ cell counts in AIDS patients were 40.6%, 35.4%, and 47.9% of the counts in healthy control, while CD3+CD8+ and CD3+CD38+ cell counts were 1.43- and 2.05-fold of the counts in healthy controls. This suggested that the normalization of CD4+CD45RA+62L+ and CD3+CD38+ cell counts may more accurately reflect immune reconstruction after HAART.
p<0.05 vs. control, # p<0.05 vs. pre-HAART, † p<0.05 vs. pre-HAART.
HAART, highly active antiretroviral therapy; 6m, 6 months after; 12m, 12 months after.
Dynamic changes of cytokine IL-12, IFN-γ, and IP-10 before and after HAART
We also found that the plasma IL-12 and IFN-γ levels were significantly lower, while IP-10 was markedly higher in HIV/AIDS patients than in controls (Table 2, p<0.05). IL-12 and IFN-γ levels increased after 12 months of HAART treatment in HIV/AIDS patients compared to their pre-HAART levels (Table 2, p<0.05). The IP-10 level was found to be downregulated in HIV/AIDS patients after 12 months of HAART (Table 1, p<0.05), although the value was still higher than in normal controls.
p<0.05 vs. control, # p<0.05 vs. pre-HAART.
HAART, highly active antiretroviral therapy; 6m, 6 months after; 12m, 12 months after; IL, interleukin; IFN, interferon; IP-10, interferon-inducible protein-10.
Correlations between Plasma IL-12, IFN-γ, and IP-10 and T cell and T cell subsets in HIV/AIDS patients
Correlations between PB CD4+, CD8+, CD4+CD45RA+62L+, CD4+CD45RO+, and CD8+CD38+ cell counts and plasma IL-12, IFN-γ, and IP-10 were analyzed (Table 3). A more significant association between CD4+/CD8+ subsets and IL-12 and IFN-γ levels was observed before and 24 months post-HAART compared to the association between CD4+/CD8+ and IL-12 and IFN-γ levels. Regression analyses were accomplished by using viewpoint of treatment time and plasma IL-12 levels as the abscissa, respectively, and PB CD4+CD45RA+62L+, CD4+CD45RO+, and CD8+CD38+ cell counts as the ordinate (Fig. 2). We found that CD4+CD45RA+62L+ and CD4+CD45RO+ cell counts positively correlated with plasma IL-12 levels (p<0.05), while CD8+CD38+ cell count negatively correlated with plasma IL-12 and IFN-γ levels (p<0.01) (Fig. 2 and Table 3). Regression analyses were accomplished by using plasma IP-10 levels of patients who took HAART for 0, 6, and 12 months and healthy people as the abscissa, and PB CD4+CD45RA+62L+, CD4+CD45RO+, and CD8+CD38+ cell counts as the ordinate, respectively (Fig. 3). The CD8+CD38+ count after taking HAART for 0, 6, and 12 months was found to be positively correlated with plasma IP-10 levels (p<0.01), while CD4+CD45RA+62L+ and CD4+CD45RO+ cell counts were negatively correlated with plasma IP-10 levels (p<0.01) (Fig. 3 and Table 3).

Interleukin (IL)-12 level is correlated with T cell subset counts.

Interferon-inducible protein-10 (IP-10) level is correlated with T cell subset counts.
(0), before HAART; (12), 12-month after HAART.
Discussion
HAART is currently the primary treatment offered to HIV/AIDS patients. It can, to some degree, achieve immune reconstruction and slow progression of diseases caused by HIV by permanently inhibiting viral replication. This study shows that HIV/AIDS patients' total Th cells (CD4+ T cell), naive Th (CD4+CD45RA+62L+), and memory Th (CD4+CD45RO+) subtypes of Th cells decreased rapidly, which reflects the damage in their immune functions. However, HIV/AIDS patients' total Tc (CD8+ T cells) and the activated subtype of Tc cells (CD8+CD38+) increased compared to healthy controls, which means that they had abnormal immune activation. With HAART treatment prolonged, total Th, naive Th, and memory Th gradually increased, while Tc and activated Tc cells gradually decreased, which proves that HAART can, to some degree, achieve immune reconstruction and inhibit abnormal immune activation in HIV/AIDS patients.
Previous reports revealed that the growth of CD4+ T cells during HAART is divided into two stages. 15,16 The first stage is mainly focused on the proliferation of memory Th, while there is little increase in naive Th cells. The second stage usually happens 2–3 months after HAART therapy, and it can last up to a year or longer. This stage is mainly focused on the proliferation of naive Th cells, while there is relatively little increase in memory Th cells. 15,16 In this study, the total Th, naive, and memory Th cells in the plasma were increased after 6 months of HAART (∼39%, ∼11%, and ∼48% increase compared to the baseline, respectively); significant differences were observed only in AIDS patients who received HAART for 12 months (∼70%, ∼107%, and ∼78% increase for total Th, naive Th, and memory Th, respectively, p<0.05). We hypothesized that the rapid increase in plasma memory Th cells after 6 months of HAART may be due to the redistribution of memory cells that remained in the lymphatic tissues, which can be quickly released into the blood stream, while the newly produced naive Th cells require more time to do so. 17
An interesting finding in this study is that the changes in IL-12 and IFN-γ correlated with changes in Th cells. IL-12 and IFN-γ belong to Th1 type cytokines. 10 IL-12 is a key regulator in cellular immunity, which can strengthen NK cells' viral response and promote the production of cytotoxic T lymphocytes. 9 A previous study demonstrated that plasma IL-12 level is related to inflammatory response induced by high viral load in AIDS patients. 11 Both IL-12 and IFN-γ have been demonstrated to play a pivotal role in resisting opportunistic infections in HIV/AIDS patients. 18
Our study demonstrated that IL-12 and IFN-γ levels were significantly lowered in HIV/AIDS patients, but HAART gradually increased their levels. However, no correlations between activated Tc cell counts and plasma IL-12 and IFN-γ levels were observed at baseline or 6 months after HAART. The only negative correlation was observed 12 months after HAART. It is unclear whether HAART can selectively inhibit abnormal immune activation. IL-12 also stimulates Th0 cells to differentiate into Th1 cells, and increase Th1 cells' activity. Our study showed significant correlations between IL-12 and IFN-γ levels and the number of Th, naive Th, and memory Th cells. This suggests that HAART may exert its role by stimulating cytokine production, and subsequently regulate Th cell differentiation and proliferation. We also noted that the correlation between naive Th, memory Th, and activated Tc cells and IL-12 and IFN-γ levels was more significant than total Th and Tc. This may suggest that Th/Tc subsets are better indicators of immune restoration in patients who received HAART than the absolute number of Th/Tc cells.
IP-10 is a newly discovered chemotactic factor of the CXC family. It is expressed in various cells, such as monocytes, endothelial cells, keratinocytes, and fibroblasts. IP-10 not only activates Th1 cells, but also stimulates activated T cells and macrophages to move to inflammatory sites. 10 However, changes in the concentration of IP-10 in different systems (e.g., blood, nervous system, spleen, and liver) are very different in response to inflammatory stimuli, such as viral infection (e.g., HCV infection). 11 The concentration of plasma IP-10 was found to be increased in HIV/AIDS patients compared to healthy controls, but its concentration rapidly decreased after HAART, which positively correlated with activated Tc cells. 19 Also, IL-12 and IFN-γ levels correlated with the number of Th cells and its subtypes. This further implies that HAART can inhibit abnormal immune activation and reduce inflammatory reactions.
In conclusion, dynamic changes in total Th, naive Th, memory Th, total Tc, and activated Tc cells were observed during HAART, but naive Th and activated Tc may be more accurate indices to evaluate immune reconstruction after HAART. Dynamic changes in IL-12, IFN-γ, and IP-10 levels and their correlations with T cell subsets were also observed, suggesting a key role of IL-12, IFN-γ, and IP-10 in immune reconstruction after HAART. Findings in this study might provide a deeper understanding of the whole picture of immune reconstruction after HAART and help find new methods of improving immune reconstruction and inhibiting abnormal immune activation in HIV/AIDS patients.
Footnotes
Author Disclosure Statement
No competing financial interests exist.