
Abstract
There are scarce data about the use of a dual therapy with lamivudine plus a ritonavir-boosted protease inhibitor (PI/r) as simplification strategy. We performed a retrospective cohort study of 44 HIV-infected patients on suppressive triple therapy PI/r-based HAART, HBV negative, who discontinued one nucleoside analogue (NA) due to toxicity, and continued dual therapy with lamivudine plus the PI/r. The median time of HIV infection was 18.6 years, and CD4+ count nadir was 150 cells/μl (6–470). They had received a mean of four regimens before (2–20), and 55% had a previous AIDS diagnosis. In eight cases, a previous resistance test showed two to seven secondary mutations in the protease gene, without resistance to the PI/r. The 184V mutation was not observed, but previous failure with a lamivudine-including regimen had been observed in four patients (9%). At baseline, patients had viral suppression (<50 copies/ml) for a median time of 794 days (235–2344), while receiving atazanavir/r in five cases, lopinavir/r in 14, and darunavir/r in 25. They discontinued mainly tenofovir (19, 43%) and didanosine (15, 34%). During 101.5 patient-years of follow-up, only two patients failed (5%), because of incomplete adherence. CD4+ count increase at 48 weeks was 55 cells/μl. No new adverse events were observed, although total cholesterol and triglycerides increased significantly during the first 6 months after simplification. In conclusion, dual therapy with lamivudine plus a boosted PI was safe and effective as simplification strategy in patients with toxicity to NA. This combination could be an alternative to mono or triple therapy in hard-to-treat patients.
Introduction
S
Several studies 4 –6 have shown that some PI/r in monotherapy could be an alternative for the maintenance of virological suppression. However, monotherapy was less effective in case of previous virological failure, or in patients with a low nadir CD4+ count. 7 Therefore, HIV treatment guidelines consider monotherapy as an alternative strategy for patients, virologically suppressed and without previous virological failure, who had toxicity or intolerance to NA. However, in the clinical setting, the management of patients could be more complex. Those developing toxicity could have limited options, because of previous failure, a low nadir CD4+ count, or intolerance to several drugs. In these patients, PI/r-based monotherapy could be a risky strategy. 8 Recently, preliminary data of a dual regimen with boosted atazanavir and lamivudine have been reported. 9 We add here the results of simplification to lamivudine plus a PI/r in the clinical setting, in patients with toxicity or intolerance to NA, as an intermediate strategy between mono and triple therapy.
Materials and Methods
This was a retrospective cohort study performed at the HIV Unit of the Ramon y Cajal Hospital. This is a university outpatient facility, located in Madrid, Spain, and specializes in providing primary and advanced care to adults living with HIV/AIDS. At the time of this study, approximately 2,400 patients were being followed at our HIV unit. All those HIV-infected patients, HBV negative, receiving an effective antiretroviral treatment including two NAs plus a PI/r who discontinued one nucleoside due to toxicity from January 2008 to December 2011, continuing therapy with lamivudine plus the same PI/r, were included. Sex, age, risk practice for HIV infection, prior AIDS diagnosis, nadir and baseline CD4+cell count, time on HAART, resistance tests, and previous lines of treatment were collected from the clinical history.
As clinical routine, subjects were followed after 4 weeks of simplifying therapy and every 12 weeks thereafter. At each visit, routine laboratory tests were performed. Analyses included a complete blood count; CD4 cell count; plasma HIV-1 RNA levels, glucose, triglycerides, cholesterol (total, low-, and high-density lipoprotein); and tests of liver and kidney function (serum creatinine and glomerular filtration rate—eGFR—by MDRD equation).
The primary outcome measure was the proportion of patients without virological failure at 48 weeks. Secondary endpoints included toxicity, changes in CD4+ count, and average change in serum lipid levels and renal parameters from baseline to week 48. Patient's end of follow-up was considered the date of regimen change or, if continued, until July 31, 2012.
The proportion of patients with HIV RNA levels lower than the limit of quantification was summarized using an intent-to-treat analysis, with changes in therapy considered as failure. Comparisons were performed using the Fisher exact test and χ2 test for categorical variables. A paired Student's t-test was used to descriptively assess the change in serum lipid values and renal parameters. All p values were two-tailed and a value of less than 0.05 was considered significant.
Results
Since January 2008, 44 patients changed to this combination as simplification strategy, and 40 had more than 48 weeks of follow-up. Baseline characteristics of the patients included in the study are shown in Table 1. Patients had received a mean of four (2–20) lines of antiretroviral treatment before effective HAART based in darunavir/r (25 patients), lopinavir/r (14 patients), or atazanavir/r (five cases), mostly as their second or third protease inhibitor-based combination. Prior to dual therapy, the nucleoside analogues used in combination with lamivudine were tenofovir (19, 43%), didanosine (15, 34%), zidovudine (5, 11%), abacavir (3, 7%), and stavudine (2, 5%). The main causes for discontinuing NA were renal toxicity in 18 cases (41%), lipodystrophy in 18 cases, and gastrointestinal disturbance in five patients. Of note, there were eight patients who had a previous genotypic resistance test available. Protease inhibitor-associated mutations were detected in the eight subjects (from two to seven mutations, 77I and 93L being the most frequent, and 48I and 82A in one case). There was no resistance to PI/r they were receiving, as expected. Reverse transcriptase mutations were detected in five subjects: conferring resistance to nonnucleoside analogues in four patients, and to NAs in five cases (TAMs in the five cases, with the presence of 210W in two patients). The 184V mutation was not observed, but previous failure with a lamivudine-including regimen was collected from the history in four patients (9%).
IDU, intravenous drug user; HAART, highly active antiretroviral therapy; NA, nucleoside analogue; GI, gastrointestinal.
At week 48, only two out of 40 patients (5%), receiving lopinavir and darunavir, had virological failure, defined as an increase in HIV RNA >50 copies/ml at two consecutive determinations. They presented an HIV RNA level of 266 and 320 copies/ml after 27 and 141 days on treatment, respectively. These failures could not be attributed to resistance to PI/r, since they did not have a previous failure with a PI, and had suboptimal adherence by self-report and pharmacy count. Moreover, for an accumulated time of follow-up of 101.5 patient-years (median time on dual therapy, 802 days, range 187–1,889), there were no more cases of virological failure. The mean increase in CD4+ count at 48 weeks was 55 cells/μl (from 403 to 458 cells/liter). No drug-related adverse events or treatment discontinuation were observed during follow-up.
The evolution of fasting lipid parameters is shown in Fig. 1. Compared with baseline, at week 24 we observed a significant increase in mean total cholesterol (from 180 to 246 mg/dl; p=0.007) and triglycerides (from 166 to 195 mg/dl; p=0.01), with a plateau or even small improvement in lipid levels after week 24. High-density lipoprotein (HDL)-cholesterol did not show significant changes during follow-up. There was a mild, not statistically significant, improvement of renal parameters after NA discontinuation. The mean serum creatinine was 1.07 mg/dl at baseline and 0.97 mg/dl at 48 weeks (p=0.4). Also, there was a mild increase in the mean eGFR from 74.2 to 83.8 ml/min (p=0.37). Indeed, for patients changing because of renal toxicity, creatinine mean levels decreased from 1.32 to 1.16 mg/dl (p=0.18), and mean eGFR rose from 68.4 to 88.5 ml/min at the end of follow-up (p=0.2).
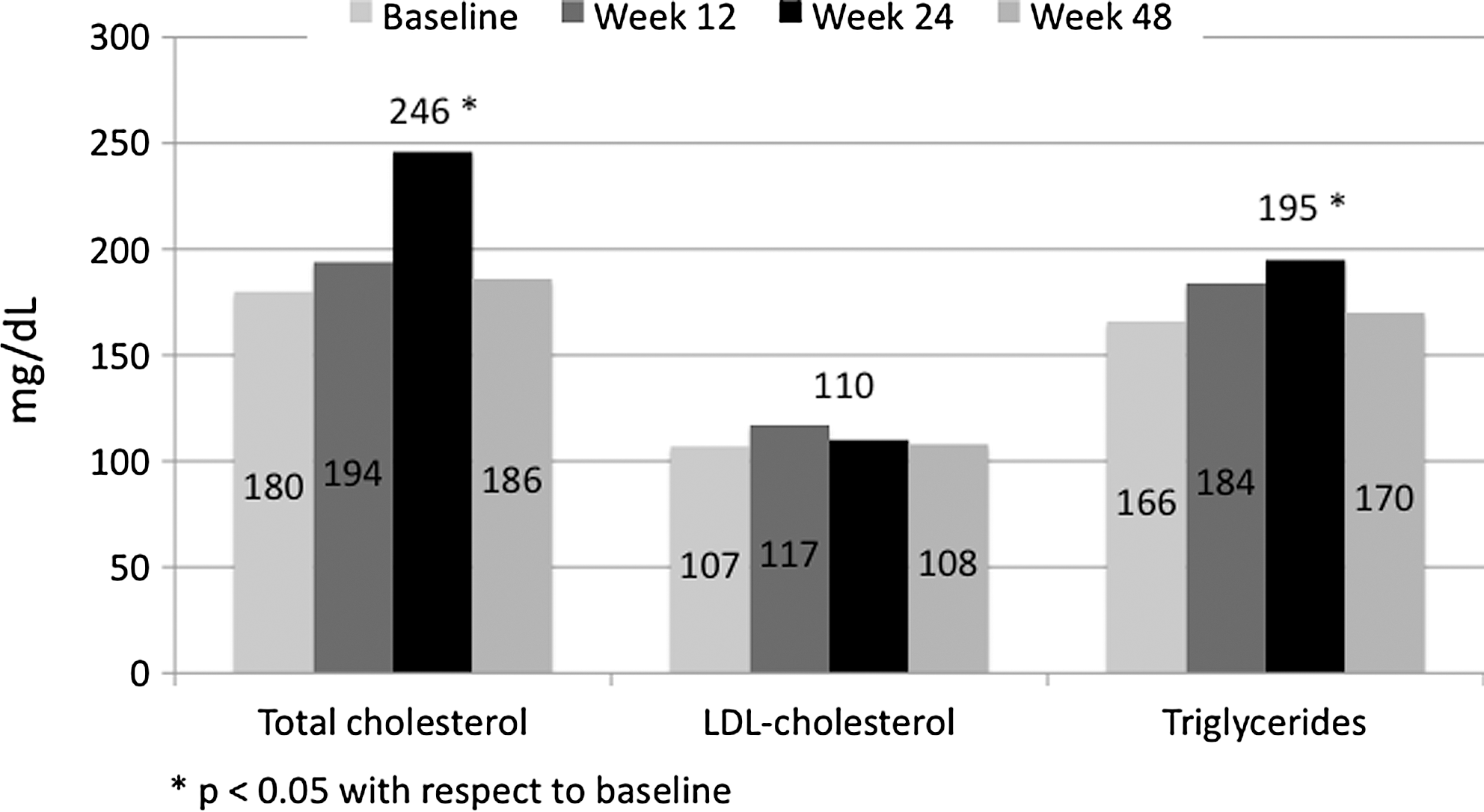
Mean fasting cholesterol, low-density lipoprotein (LDL)-cholesterol, and triglycerides at baseline and at week 48 for patients receiving lamivudine plus a ritonavir-boosted protease inhibitor (PI/r), after discontinuation of a nucleoside analogue.
Discussion
Our study is, to our knowledge, the first to demonstrate that the use of a dual therapy with lamivudine plus a PI/r in the clinical setting is safe and effective if it is necessary to discontinue one NA. In this small study, including pretreated patients with NA intolerance, 95% of patients had plasma HIV RNA levels below 50 copies/ml after 48 weeks, and there were no more cases of virological failure in a follow-up that lasted for more than 2 years.
To date, simplification strategies have been based on the replacement for a different antiretroviral drug 10 –13 with the subsequent risk of new adverse events, of virological failure in patients who had previously received suboptimal treatments, 14 and with the stress associated with the initiation of a new regimen. 15 However, simplification to dual therapy in patients who were already tolerating the drugs was associated with the absence of adverse events, as expected.
The main limitation of our study was the lack of a control group, especially patients receiving monotherapy. Therefore, we cannot demonstrate that our regimen could be better than the use of a PI/r alone, considering that four of our patients had previously failed in a lamivudine-containing regimen. Multiple clinical trials have shown good results of monotherapy in maintaining virological suppression. 16,17 However, this strategy seems to be slightly less effective over time than triple therapy, as shown by several meta-analyses, especially in pretreated patients. 18 In our patients, the use of monotherapy was not the first option due to the characteristics of the patients, with a low CD4+ count nadir, and a high proportion of previous AIDS, in pretreated patients.
Additionally, the main reason for deciding to use dual therapy in our patients was the presence of renal alteration, due to the simultaneous presence of tenofovir and other concomitant factors for kidney toxicity, such as hypertension or diabetes. 19,20 Although in our patients the improvement was small after tenofovir withdrawal, suggesting the important role of these classical factors, there was no renal impairment during follow-up. Interestingly and in agreement with recent published data, 21 there was an initial increase in total cholesterol and triglycerides in patients who stopped taking tenofovir. This fact is not surprising, since the independent lipid-lowering effect of tenofovir has been shown in HIV patients and HIV-negative subjects treated with this drug. 22 –24 However, this worsening of lipid parameters reached a plateau with later mild improvement.
In conclusion, we present here the outcome of patients simplified to lamivudine plus PI/r dual therapy due to intolerance or toxicity, and who, a priori, were not suitable candidates for the use of monotherapy. Our study was retrospective and it includes only a small sample size, but despite its limitations we believe that this work provides information that would be useful in the clinical setting, increasing our arsenal of effective simplification strategies. Thus, our results could serve as proof of concept of the efficacy of lamivudine plus PI/r as simplification in HIV-infected, “hard to treat” patients.
Footnotes
Acknowledgments
We would like to thank Ana Abad for important contributions to database management. M.P. is a recipient of an official Rio Hortega predoctoral fellowship (CM09/00227). All research was conducted within the guidelines of ethical principles and local legislation.
Author Disclosure Statement
J.L.C. is an advisor to Janssen, Gilead, MSD, Boehringer, BMS, ViiV, and Abbott, is on the speaker's bureau of Janssen, Abbott, and Gilead, and has received grants and travel/meeting expenses from ViiV, Janssen, Abbott, and Gilead. S.M. is an advisor to, is on the speakers' bureau of, and has received research grants and travel/meeting expenses from MSD, BMS, Gilead, Janssen, Abbott, Roche, and Boehringer-Ingelheim. M.J.P.E. is an advisor to, is on the speaker's bureau of, and has received research grants and travel/meeting expenses from ViiV, Janssen, BMS, Abbott, and Gilead.