
Abstract
We sought to determine the pattern of resistance-associated mutations (RAMs) among HIV-1-infected children failing first-line antiretroviral therapy (ART) and ascertain their response to second-line regimens in 48 weeks of follow-up. The design involved a cohort study within an HIV care program. We studied records of 142 children on ART with virological failure to first-line ART and switched to second-line ART with prior genotypic resistance testing. The pattern of RAMs was determined in frequency runs and the factors associated with accumulation of≥3 thymidine analogue mutations (TAMs) and K103N were determined using multivariate logistic models. Changes in weight, height, CD4, and viral load at weeks 24 and 48 after switch to second-line therapy were determined using descriptive statistics. The children were mean age 10.9±4.6 years and 55.6% were male. The commonest nucleoside reverse transcriptase inhibitor (NRTI) RAM was M184V in 129/142 (90.8%) children. TAMs,≥3 TAMs, 69 insertion complex, K65R/N, and Q151M were observed in 43.0%, 10.6%, 18.3%, 2.8%, and 2.1% of the children, respectively. The commonest nonnucleoside reverse transcriptase inhibitor (NNRTI) RAM was K103N in 72/142 (50.7%) children. The starting ART regimen was associated with accumulation of both≥3 TAMs (p=0.046) and K103N (p<0.0001), while a history of poor adherence was associated with K103N accumulation (p=0.0388). After 24 weeks and 48 weeks of follow-up on lopinavir-ritonavir based second-line ART, 86/108 (79.6%) and 84.5% (87/103) of the children had viral loads<400 copies/ml, respectively. The mean CD4 absolute count increased by 173 cells/μl and 267cells/μl at weeks 24 and 48, respectively. Increments were also observed in mean weight (1.6 kg and 4.3 kg) and height (1.8 cm and 5.8 cm) at weeks 24 and 48, respectively. Multiple RAMs were observed among HIV-1-infected children with virological failure on first-line ART with M184V and K103N most frequent. The children responded favorably to boosted PI-based second-line ART.
Introduction
T
Many countries in sub-Saharan Africa have rolled out ART to HIV-infected adults and children, with Uganda being among the pioneering countries. 1,2 In March 2011, 22,798 Ugandan children were reported to be on ART. 3 Many of these children are at risk of developing antiretroviral drug resistance. Studies in ART-naive children are limited, but reports from adult studies indicate that primary viral resistance to ARVs is becoming a major problem in Uganda and other sub-Saharan countries. 4,5 Among ART-experienced HIV-infected children studies have reported the emergence of resistance-associated mutations to nucleoside reverse transcriptase inhibitors (NRTIs), nonnucleoside reverse transcriptase inhibitors (NNRTIs), and protease inhibitors (PIs). 6 –12
In the absence of individual viral resistance information, the World Health Organization (WHO) guidelines are what most national programs in sub-Saharan Africa follow to initiate and switch ART in HIV-infected children. 13 These guidelines recommend NRTI and NNRTI combination first-line ART and boosted PI-based second-line therapy when the first-line regimens fail. There are limited data on resistance-associated mutations among HIV-infected children failing such first-line ART and response to the second-line regimens in sub-Saharan Africa.
We set out to determine the pattern of antiretroviral drug resistance-associated mutations (RAMs) among HIV-1-infected Uganda children failing first-line therapy and investigate how these mutations would relate to the WHO recommended second-line ART regimens. We also followed up the children on second-line regimens for 48 weeks to ascertain the clinical, immunological, and virological response to the therapy.
Materials and Methods
We conducted a chart and database review of children who ever received ART at the Joint Clinical Research Centre (JCRC), Kampala from January 2004 to December 2010 under the general access treatment program supported by the President's Emergency Plan For AIDS Relief (PEPFAR) and Clinton Health Access Initiative (CHAI). We selected 142 children who had been switched to second-line ART after development of virological failure to their first-line regimens and had switched after genotypic resistance testing. We assessed the resistance profiles of these children at switch to second-line therapy, as well as the immunological and virological response to the second-line regimens at weeks 24 and 48 postswitch. Figure 1 shows how these children were selected.
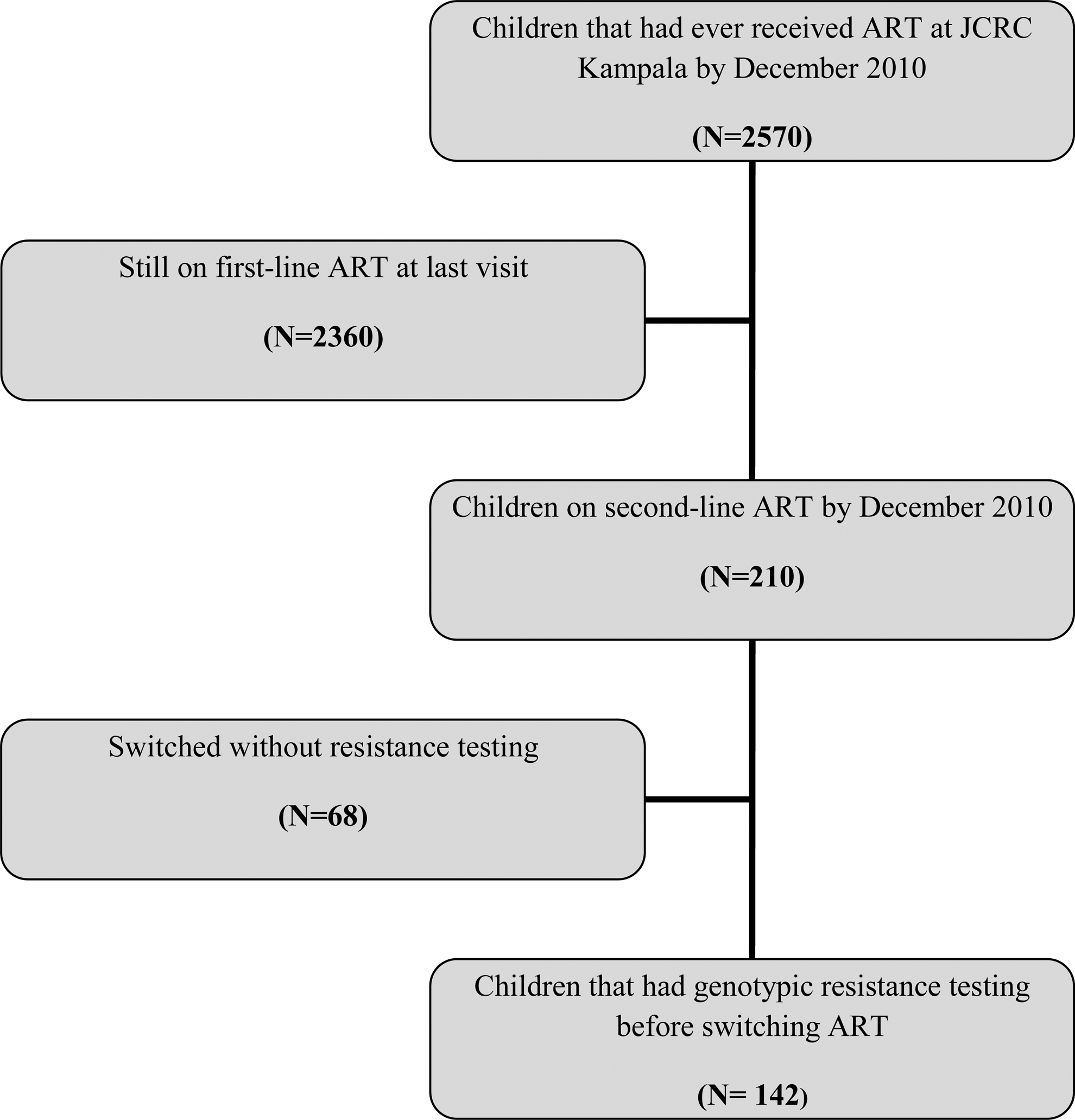
Flow chart showing how the study participants were selected.
Study setting
The study was carried out at JCRC Kampala, which houses the headquarters of this HIV care and research institution with both adult and pediatric populations. Children registered under the PEPFAR and CHAI-supported general access program received free services, such as ART, opportunistic infections prophylactic medication, adherence counseling, routine laboratory monitoring tests, and nutritional supplements. The criteria for ART initiation and switching were by the WHO guidelines for ART initiation in infants and children. 13 When results of resistance testing were available, they would be taken into consideration at the time of switching to second-line therapy. Among the routine laboratory monitoring tests performed were CD4 cell count and CD4 percentages every 6 months, plasma HIV-1 (RNA) viral load annually, and genotypic resistance testing when needed.
Genotypic resistance profiles
Genotypic resistance testing was done where the attending physician suspected ART failure, usually for patients with viral loads>2000 copies/ml, as this was the threshold beyond which mutations could be detected in the laboratory. The genotypic resistance sequencing was done using in house primers. The sequences were edited using Bio-Edit Sequence Alignment Editor (Version 7.0.5) and analyzed using the HIV drug resistance database of Stanford University. 14 Drug resistance mutations were assessed using the 2011 updated International AIDS Society (IAS)–USA list of the drug resistance mutations in HIV-1. 15 The drug classes evaluated included NRTIs, NNRTIs, and PIs. Drug susceptibility for each patient was categorized as susceptible, potential low-level resistance, low-level resistance, intermediate resistance, or high-level resistance using the Stanford algorithm. 14
Statistical analysis
We extracted the children's demographic and treatment information from their medical records at the clinic using a standard tool. This information included their gender, age at time of assessment, duration on first-line antiretroviral medication, their initial treatment regimen, history of poor adherence, and whether they were exposed to the use of prevention of mother-to-child transmission of HIV (PMTCT) medications. Also extracted were the weight, height, CD4 count and percentage, and viral load at baseline, week 24, and week 48 after switch to second-line ART. Using the same tool, the genotypic resistance profiles were reviewed to ascertain the HIV subtype and the drug resistance-associated mutations. The overall aim of this investigation was to describe the RAMs in children failing first-line ART and ascertain the short-term response to second-line regimens. We achieved this by constructing frequency runs of the most commonly identified NRTI and NNRTI RAMs. For continuous variables that followed a normal distribution, we generated and present their descriptive statistics. In secondary analyses, we investigated the factors associated with the accumulation of three or more thymidine analogue mutations (TAMs) and K103N mutations among the children. Included among TAMs were the following NRTI RAMs: M41L, D67N, K70R, L210W, T215Y/F, and K219Q/E. We achieved this in univariable logistic models with the demographic and treatment characteristics as the independent variables. We also constructed a multivariable model to explain the joint demographic and treatment factors associated with detecting the K103N mutation using the backward elimination algorithm. All factors that had achieved a statistical p-value cut-off of 0.2 were considered eligible to be included in the model.
The weight, height, CD4, and viral load changes from baseline to weeks 24 and 48 were determined using descriptive statistics. Univariable logistic models were used to investigate the factors associated with achieving a viral load of<400 copies per ml at week 24.
All statistical analyses were performed using the Stata 11/IC (Stata Inc., Texas) software, all statistical inferential framework was based on the 5% error level, and all presented p-values were based on two-tailed tests.
Results
Of 2,570 children who were cumulatively provided with ART at JCRC Kampala on the general access treatment program between January 2004 and December 2010, 210 (8.2%) failed first-line ART and were switched to second-line ART, and of these 142 (67%) had genotypic testing results. These were included in this investigation (Fig. 1). The mean age of the 142 children at the time of the investigation was 10.9±4.6 years; all had been on treatment for the past 5.9±2.0 years; 79 (55.6%) were male; 49/103 (47.6%) and 45/103 (43.7%) had HIV-1 subtype D and A, respectively; 82 (57.8%) and 51 (35.9%) started on nevirapine (NVP) and efavirenz (EFV)-based ART regimens respectively (Table 1); 70/138 (50.7%), 64/138 (46.4%), and 4/138 (2.9%) were initiated on stavudine (d4T), zidovudine (AZT), and abacavir (ABC)-containing regimens, respectively; and all had lamivudine (3TC) in their initial regimen.
PMTCT, prevention of mother-to-child transmission; NVP, neviripine; EFV, efavirenz; NRTI, nucleoside reverse transcriptase inhibitor.
NRTI resistance-associated mutations
Table 2 contains a list of all NRTI and NNRTI mutations detected among the participating children. Only 5/142 (3.5%) of the children who failed first-line ART and had resistance testing done did not have any NRTI RAMs. The commonest NRTI RAM was M184V, which was detected among 129/142 (90.8%) children, and in 41/142 (28.9%) children it was the only identified NRTI RAM.
Other commonly observed NRTI RAMs were the TAMs: T215Y/F (n=61; 43.0%), K219Q/E (n=35; 24.6%), D67N (n=32; 22.5%), and K70R (n=30; 21.1%) (Table 2). Three or more TAMs were observed among 15/142 (10.6%) of the children (Table 1).
The K65R/N mutation was observed in only 4/142 (2.8%) children while the Q151M was identified in only 3/142 (2.1%) children. On the other hand 69 insertion complex (T69N/D) was frequently observed (26/142; 18.3%).
Children initiated on d4T-containing regimens were 70% less likely to accumulate≥3 TAMs than those initiated on ZDV-containing regimens, OR: 0.30, 95% CI: 0.09 to 0.98, p=0.046.
We also observed a borderline significant association between age of the child and accumulating≥3 TAMs, where each additional year was associated with an 11% reduction [odds ratio (OR): 0.89, 95% confidence interval (CI): 0.79 to 1.01] in the odds of accumulating≥3 TAMs (p=0.0558). No other demographic and treatment factor was significantly associated with accumulation of≥3 TAMs (Table 3).
NNRTI resistance-associated mutations
Among the children who had resistance testing done, only 2/142 (1.4%) did not have any NNRTI RAM. The most commonly observed NNRTI RAM was K103N in 72/142 (50.7%) of the children and in 15/142 (10.6%) children it was the only identified NNRTI RAM. G109A/S and Y181C were also commonly observed in 45/142 (31.7%) and 33/142 (23.2%) children, respectively. Other commonly observed NNRTI RAMs were K101E/H/P (n=29; 20.4%) and P225H (n=20; 14.1%) (Table 2).
The starting first-line ART regimen (p<0.0001) and history of poor adherence (p=0.0388) were independently significantly associated with accumulation of K103N, whereas age (p=0.0552) and prior exposure to drugs for prevention of mother-to-child transmission of HIV (PMTCT) (p=0.0632) had a borderline significant association with K103N accumulation (Table 3). When adjusted for history of poor adherence, age, and prior exposure to drugs for PMTCT, children initiated on EFV-based regimens were almost six times more likely (adjusted OR: 5.56, 95% CI: 2.28 to 13.60), p=0.0002) to accumulate K103N when compared to those initiated on NVP-based regimens (Table 3). On the contrary, the Y181C mutation was observed in 26/29 (89.7%) children whose initial regimen was nevirapine based, and not at all among children whose initial regimen was efavirenz based (p<0.0001). Of note there was no significant difference observed between the proportions of children with a history of poor adherence among children initiated on EFV-based versus NVP-based regimens (p=0.878).
PI resistance-associated mutations
Twelve children had resistance testing done for PIs and of these two had PI resistance-associated mutations. One child had a single L23I, which is an accessory mutation. 14 The other child had D30N, M46I, I54V, V82A, and N88D, as well as multiple NRTI RAMs including several TAMs. She had been referred to the JCRC with a history of multiple ARV drug exposure over a 10-year period and poor adherence.
Response to second-line antiretroviral regimens
All second-line regimens were boosted PI based (lopinavir-ritonavir; LPVr), with the most frequently chosen regimens being AZT/3TC/DDI/LPVr (n=42), ABC/DDI/LPVr (n=31), AZT/3TC/LPVr (n=15), and AZT/3TC/TDF/LPVr (n=13). Of 129 children with the M184V mutation, 80 (62.0%) had 3TC maintained in their second-line regimens and another 10 (7.8%) were put on emtricitabine (FTC)-containing regimens. Four children (2.8%) were lost to follow-up and 6 (4.2%) were transferred out to other treatment centers; no child is known to have died in the 48 weeks of follow-up. The remaining children responded well to the second-line regimens as shown by the favorable mean weight, height, CD4 count (%), and viral load at weeks 24 and 48 (Table 4). The mean CD4 absolute count increments were 173 cells/μl and 267cells/μl at weeks 24 and 48, respectively (Table 4). After 24 weeks and 48 weeks of follow-up, the proportions of children with viral loads<400 copies/ml were 86/108 (79.6%) and 87/103 (84.5%), respectively.
Mean (standard deviation).
A marginally significant difference was observed between the proportion of children in whom 3TC/FTC was maintained in the second-line regimens with a viral load of<400 copies/ml at week 48 [57/71 (80.3%)] compared to 31/33 (93.9%) among those in whom 3TC/FTC was not maintained, p=0.072. At week 24, the difference was less significant where 76.3% (58/76) of children in whom 3TC/FTC was maintained in second-line regimens had viral loads<400 copies/ml compared to 85.3% (29/34) of children in whom 3TC/FTC was not maintained with viral loads<400 copies/ml, p=0.285. Furthermore, there was no statistical difference between the proportions of children with the M184V mutant virus versus those with the wild-type 184 virus, with viral loads<400 copies/ml at week 24 [83/105 (79.1%) versus 5/6 (83.3%), p=0.801] or at week 48 [81/97 (83.5%) versus 8/8 (100%), p=0.212].
Children with a history of poor adherence were 97% less likely to achieve a viral load of<400 copies per ml when compared to those whose adherence was optimal, OR=0.03, 95% CI: 0.007, 0.111, p<0.0001. No other demographic and treatment factor was significantly associated with failure to achieve a viral load of<400 copies per ml (data not shown).
Discussion
Viral resistance to ARVs in the setting of limited drug options such as sub-Saharan Africa warrants an insight into the pattern of RAMs among children failing first-line ART to guide second-line ART choices. In this study, we found that 98.6% of HIV-1-infected children with virological failure to first-line ART had at least one RAM, with M184V and K103N being the most commonly observed NRTI and NNRTI RAM, respectively; TAMs and the 69 insertion complex were observed in 43.0% and 18% of the children, respectively, but the K65R/N and Q151M were rare. As expected, the children responded well to PI-based second-line ART regimens.
This pattern of RAMs among children with virological failure on reverse transcriptase-based therapy is consistent with previous findings in Central African Republic, Tanzania, Brazil, China, Thailand, and earlier in Uganda. 7,10, 16 –19 However, we observed a much higher frequency of the 69 insertion complex, which is associated with resistance to all NRTIs currently approved by the US FDA 20 when present with one or more TAMs at codons 41, 210, or 215. 15 This together with the observed high rate of accumulation of TAMs is of particular concern regarding the role of the NRTI backbone in second-line regimens, still recommended by WHO. 13 On a positive note, the K65R mutation, which is associated with reduced susceptibility to abacavir (ABC) and tenofovir (TDF) as well as didanosine (DDI) and d4T, 15 was rare, contrary to what was observed earlier in Nigeria 21 and South Africa. 22 Over 95% of the children in our study started with AZT or d4T and since WHO recommends ABC or TDF as part of second-line ART for these children, 13 it is expected that such ABC/TDF-containing regimens would be efficacious. Furthermore, the multi-NRTI resistance Q151M 14,15 was also rarely observed in our study.
The M184V mutation, which is associated with resistance to 3TC and FTC, when present with TAMs increases ABC resistance 15,23 further compromising the usefulness of ABC in second-line regimens, but it appears to delay or prevent the emergence of TAMs. 15, 24 This explains why 3TC was maintained in most of the second-line regimens of the children in our study. However, in the 48 weeks of follow-up, we did not observe an added benefit in terms of viral suppression of maintaining 3TC in the second-line regimens. On the contrary, though marginally significant, at week 48 a greater proportion of children in whom 3TC was not maintained (94%) had viral loads<400 copies/ml when compared to those in whom 3TC was maintained (80%).
The K103N mutation that confers high level resistance to NVP and EFV is not associated with resistance to etravirine (ETR) or rilpivirine (RPV) if occurring singly. However, the clinical utility of these two drugs is reduced by the occurrence of mutations that were significantly observed in our study including L100I, K101P, E138A/G/K/Q, V179L, Y181C/I/V, H221Y, and M230L, especially if occurring in combination. 15 Therefore before considering using ETR or RPV in ART-experienced children with virological failure and prior exposure to NVP or EFV, a resistance profile should be obtained.
The accumulation of three or more TAMs, which increases the chances of high level resistance to d4T and AZT as well as contributing resistance to many of the other NRTIs, 14 and of K103N was observed to be associated with the first-line ART regimen the child started with. A history of poor adherence was associated with an accumulation of K103N and poor virological response to second-line regimens. The effect of a history of poor adherence on the accumulation of mutations is not surprising given that it has been widely observed. 25 –27
Studies comparing EFV and NVP have either found EFV-based regimens to be more efficacious 28,29 or have shown similar immunological and virological outcomes 30 –32 ; K103N has been identified more among efavirenz-based regimens and Y181C with nevirapine-based regimens. 28 A recent study in Botswana found children on EFV-based regimens to be less adherent to their regimens when compared to those on NVP-based regimens, 33 although this was not observed in our study. We found that the children whose starting ART regimen was EFV based were six times more likely to develop K103N and 55% less likely to have three or more TAMs when compared to those who started on an NVP-based regimen, and that the Y181C was identified only in children with prior NVP exposure and not at all among the children with prior EFV exposure. This reaffirms that both EFV- and NVP-based regimens should continue to be provided as NNRTI options for first-line ART in national programs.
After 24 weeks and 48 weeks of follow-up of the children on boosted PI (LPVr)-based second-line regimens, 80% and 85% of the children had viral loads<400 copies/ml, respectively. This is very favorable response and reassuring given the high level of TAMs that were observed. However, it should be noted that these children were switched with knowledge of their individual resistance profiles. Similar results were obtained in a Chinese study. 34
Although this was an observational study and the study population was not chosen at random, it provides an insight into the RAMS expected among HIV-1-infected children failing WHO-recommended first-line ART regimens and the short-term response to boosted PI-based therapy. Another limitation of the study is that the threshold for performance of resistance testing, which is 2000 copies, was rather high. This could have led to a greater accumulation of RAMs.
In conclusion, we observed multiple NRTI and NNRTI mutations among HIV-1-infected children failing first-line ART, with a potential to limit the usefulness of the NRTI class of drugs for second-line ART as recommended by WHO. Fortunately boosted PI-containing second-line regimens remain effective during this short-term follow-up. Virological monitoring needs to be promoted in resource-limited settings to identify treatment failure early and switch therapy before several mutations are accumulated, thereby preserving subsequent treatment options. Furthermore, care should be taken when choosing between AZT and d4T or between EFV and NVP to constitute a first-line ART regimen and optimal adherence to ART should be ensured to prevent the accumulation of RAMS.
Footnotes
Acknowledgments
The authors would like to thank the management and staff of JCRC, Kampala for their support of this operational research, and in particular the following staff of the pediatric and laboratory departments: Eva Natukunda, Rosette Keishanyu, Philip Apugulu, Ruth Nandugwa, Ruth Sendi, Wilfred Opilo, Annet Nandudu, Judith Byaruhanga, Sam Ssenyonjo, Charity Musiime, Priscilla Kyobutungi, Asia Namusoke, Paul Oronon, Immaculate Kyosaba, Peter Erimu, James Nkalubo, John Okiror, Fred Kyeyune, Hannah Nanyonjo, Leonard Bagenda, Stanley Bulime, Godfrey Pimundu, Lydia Nakiire, Jonathan Mwesigwa, Martin Katuramu, Lincoln Mugarura, and Peter Awio. We also thank the Case Western Reserve University for their support of the resistance testing laboratory. Drugs and laboratory tests were provided to children with funding from USAID with support from PEPFAR as well as CHAI.
Author Disclosure Statement
No competing financial interests exist.