
Abstract
Cross-sectional prevalence studies based on immunoassays that discriminate between recent and long-term infections, such as the BED assay, have been widely used to estimate HIV incidence. However, individuals receiving highly active antiretroviral therapy tend to have lower BED levels and are associated with a higher risk for being mistakenly classified as recent infections. To assess the effect of short-term antenatal zidovudine (ZDV) and single-dose nevirapine (sdNVP) on the BED levels in HIV-1C infection, we measured longitudinal BED normalized optical density (OD-n) levels using stored plasma samples collected prenatally and postnatally from 159 pregnant HIV-infected women in Botswana who participated in the randomized clinical Mother-to-Child-Prevention study, the Mashi study. All women received ZDV from 34 weeks gestation through delivery and were randomized to receive either sdNVP or placebo during labor. Among 159 subjects, the OD-n levels decreased from baseline to delivery in 93 subjects (p=0.039), suggesting that short-course ZDV may decrease OD-n levels. sdNVP at delivery did not affect longitudinal BED OD-n levels postdelivery. However, sdNVP appeared to modify the association between CD4 count at delivery and OD-n levels postdelivery. When estimating HIV incidence with the BED assay, special care may be required regarding women who received short-term ZDV for prevention of mother-to-child transmission.
A
The BED assay 5 detects increasing levels of anti-HIV immunoglobulin G (IgG) after seroconversion and classifies HIV-1 individuals as recently infected depending on whether a normalized absorbance reading lies below or above a preset normalized optical density (OD-n) cutoff point. BED testing has very high reproducibility 6 and has been used worldwide to estimate HIV incidence, both in general populations and in high-risk groups. 7 However, when tested with the BED assay, some individuals remain nonreactive indefinitely, yielding false recent results. 8 –10 Ignoring this leads to an overestimate of HIV incidence. 11 –13
Being mistakenly classified as a recent infection is especially common when BED assays are applied to individuals receiving highly active antiretroviral therapy (HAART). Marinda et al. 14 reported an increase in false recent rates from 11.2% before HAART to 17%, 25%, 38%, and 56% at 0.5, 1, 1.5, and 2 years, respectively, after HAART initiation in subjects from South Africa with predominantly subtype C infection. Laeyendecker et al. 15 found that >2 years of HAART was significantly associated with misclassification using the BED assay in men who have sex with men from the United States who were likely to be infected with subtype B HIV. Laeyendecker et al. 16 estimated that the odds of misclassification with the BED assay among patients who were taking HAART was 1.91 of that among those who were not taking HAART in subjects from Eastern African countries where subtypes A and D are prevalent and those from Southern African countries where subtype C is prevalent. One possible explanation is that HIV-specific IgG levels decrease with viral load suppression due to HAART.
HIV is the leading cause of death in women of reproductive age around the world. 17 In 2010, around 390,000 children became infected with HIV, mainly through mother-to-child transmission. 18 More than 90% of children living with HIV reside in sub-Saharan Africa. 18 In resource-limited settings, most of the prevention of mother-to-child transmission (pMTCT) has focused on World Health Organization (WHO) 2006 recommendation 19 on zidovudine (ZDV) and single-dose nevirapine (sdNVP) at the time of labor.
The effect of HAART on BED OD-n levels has led to recommendations on excluding subjects receiving HAART for viral suppression in the cross-sectional survey for estimating HIV incidence. 8 However, to our knowledge, the effect of short course ZDV and sdNVP for pMTCT on BED OD-n levels has not been examined. In this article, we aim to evaluate the effect of ZDV and sdNVP on BED OD-n levels. We also evaluate the effect of CD4 cell count and HIV-1 plasma viral load on BED OD-n levels.
Plasma samples were collected during the Mashi study, 20,21 a 2×2 factorial randomized clinical trial of 1,200 HIV-infected pregnant women in Botswana, enrolled between March 2001 and October 2003, to assess the equivalence of maternal short-term ZDV plus sdNVP at labor versus ZDV alone (placebo instead of sdNVP) for pMTCT. All women received ZDV from 34 weeks gestation through delivery and were randomized to receive either sdNVP or placebo during labor. The design and main results of this study have been reported elsewhere. 20 –22
To assess the effect of ZDV and/or sdNVP on the BED levels, we considered only samples drawn before initiation of HAART in eligible women. Furthermore, we included only subjects with samples at appropriate time points to allow assessment of longitudinal trajectories. Therefore, we first restricted our attention to subjects with specimens drawn at the following time points: (1) enrollment, (2) during the first 3 days following the birth of the infant, and (3) at least one additional time point within 12 months following the birth of the infant. A total of 176 women with 812 specimen records were identified to meet these criteria through electronic specimen inventory list. Among these 812 specimen records, 65 specimens were not available for testing for BED, either because all the aliquots had been used for previous research purposes or because the quality of the specimens had deteriorated over time during storage. BED OD-n results were obtained for 747 samples from 176 women. Among these 747 results, 10 were suspected as outliers because they produced values that appeared to fall outside of a reasonable range when compared to preceding and subsequent values obtained from the same subjects and available amount of specimen did not allow retesting, therefore these values were removed from the main analysis. Additional sensitivity analyses including these 10 values were performed to assess the robustness of the conclusions to inclusion or exclusion of these 10 values; the results were consistent and yielded the same conclusions (data not shown, available upon request).
Although 737 OD-n values from 176 women were available, 17 women no longer had OD-n results at appropriate time points that allowed us to assess the longitudinal change from baseline to delivery and postdelivery changes; among these 17 women, one did not have an OD-n result at entry, 14 had no OD-n results within 3 days following the birth of the infant, and two no longer had a postdelivery OD-n result within 12 months. The final inclusion criteria for subjects included in our analysis were subjects with available BED OD-n results at the following time points: (1) enrollment, (2) during the first 3 days following the birth of the infant, and (3) at least one additional time point within 12 months following the birth of the infant. A total of 159 women met these criteria, among whom 92 were from the placebo arm and 67 were from the NVP arm. Figure 1 provides a diagram of the selection process for all the subjects who were included in the current analysis from the Mashi trial.
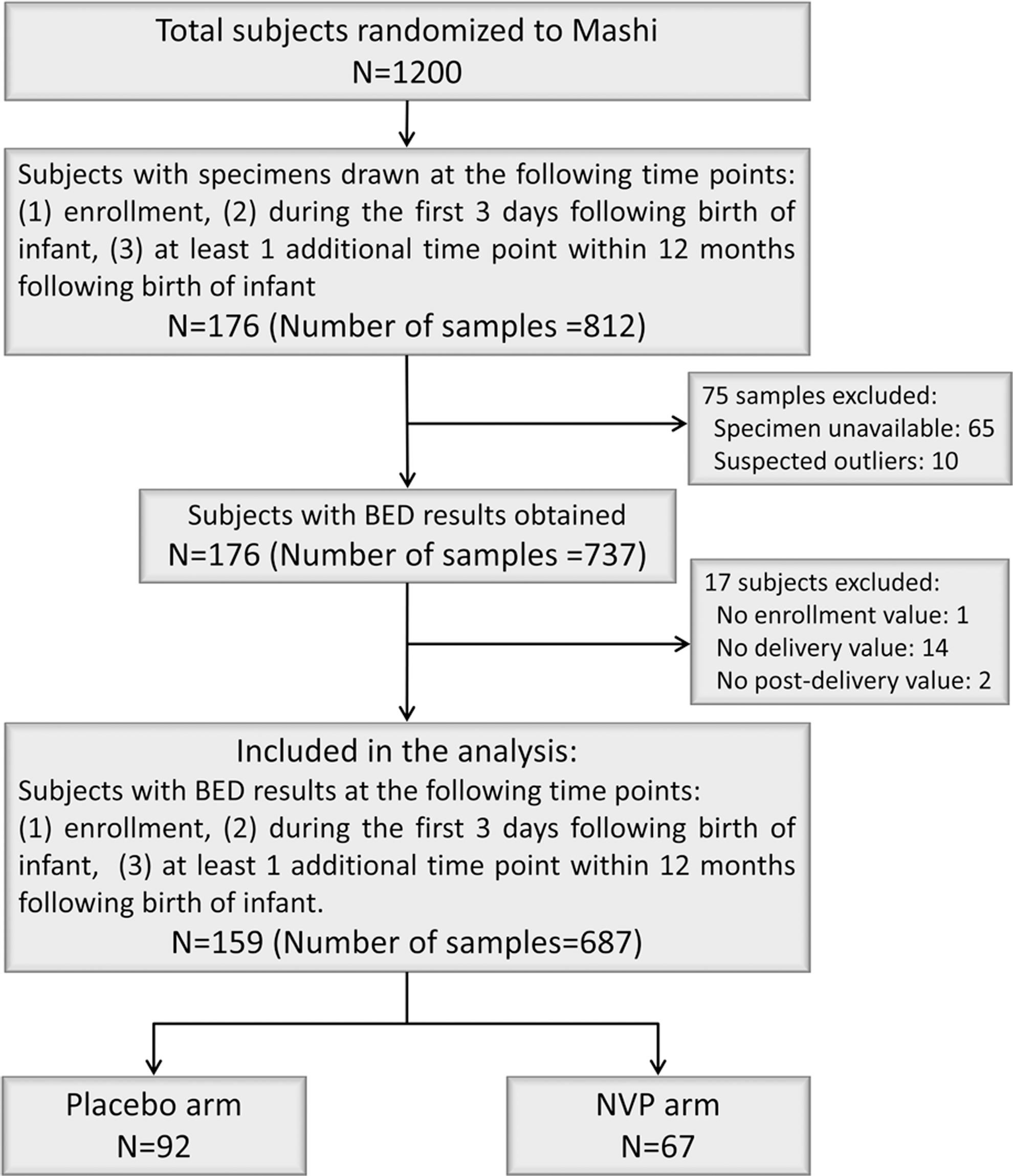
Diagram of the selection process for subjects included in the current analysis.
Plasma samples were tested by BED, measuring change in anti-IgG activity relative to total IgG. The Calypte Aware BED HIV-1 Incidence Assay (Calypte Biomedical Corporation, Portland, OR) was used, according to the manufacturer's recommendations. Demographic data, HIV-1 RNA load, and CD4 count results were obtained from the Mashi study.
All analyses were performed using SAS (SAS Institute, Inc., Cary, NC) and R (version 2.13 or higher). Associations were examined using Spearman correlations. The BED OD-n level for the specimen with date on or before, and closest to, the randomization date was used as the baseline. The BED OD-n levels at delivery (after receiving short-course ZDV) and at baseline (prior to receiving short-course ZDV) were compared using the Sign test. Regression models were used to assess the effects of baseline CD4 count and viral load on changes in BED OD-n levels from baseline to delivery. The OD-n levels for subjects in the NVP group and in the placebo group were compared using the Wilcoxon rank-sum test. To examine the effect of sdNVP at delivery on OD-n levels postdelivery, we fitted mixed effect models to account for repeated measurements for subjects over time. We also assessed whether HIV RNA levels and CD4 count at delivery modify the effect of sdNVP on OD-n levels by including appropriate interaction terms in the model. All tests were two-sided with 5% significance level.
Results are based on a total of 687 samples, from 159 women, with ages ranging from 23 to 29 years old. The number of samples per subject ranged from three to eight, with a median of five. Characteristics of the subjects included in the current analysis at baseline and at delivery, overall and by treatment groups, are presented in Table 1. Age, CD4 count, and HIV-1 RNA levels were similar for subjects randomized to the NVP group and the placebo group at baseline. At delivery, the HIV-1 RNA levels were also similar between the two treatment groups, while the CD4 counts appeared to be slightly higher in the NVP group than in the placebo group. Characteristics of all Mashi subjects at baseline and at delivery are also presented. Age, CD4 count, and HIV-1 RNA levels were comparable for those 159 subjects included in the current analysis and all Mashi subjects, with subjects in the subsample having slightly higher CD4 counts and lower HIV-1 RNA levels. No substantial differences in these characteristics were seen between two treatment groups, or between the subsample and the full sample.
NVP, nevirapine; IQR, interquartile range.
Figure 2 plots individual OD-n levels over time by treatment group (NVP versus placebo), with delivery time chosen as time 0. Figure 3 provides boxplots of BED OD-n levels at baseline, delivery, and 1, 6, and 12 months after delivery. The median time from study entry to delivery was 1.3 months (IQR: 1.0–1.6 months). At baseline, BED OD-n levels negatively correlated with CD4 count (r=−0.22, p=0.006), and appeared to be positively correlated with HIV RNA levels (r=0.12), but did not reach statistical significance (p=0.14).
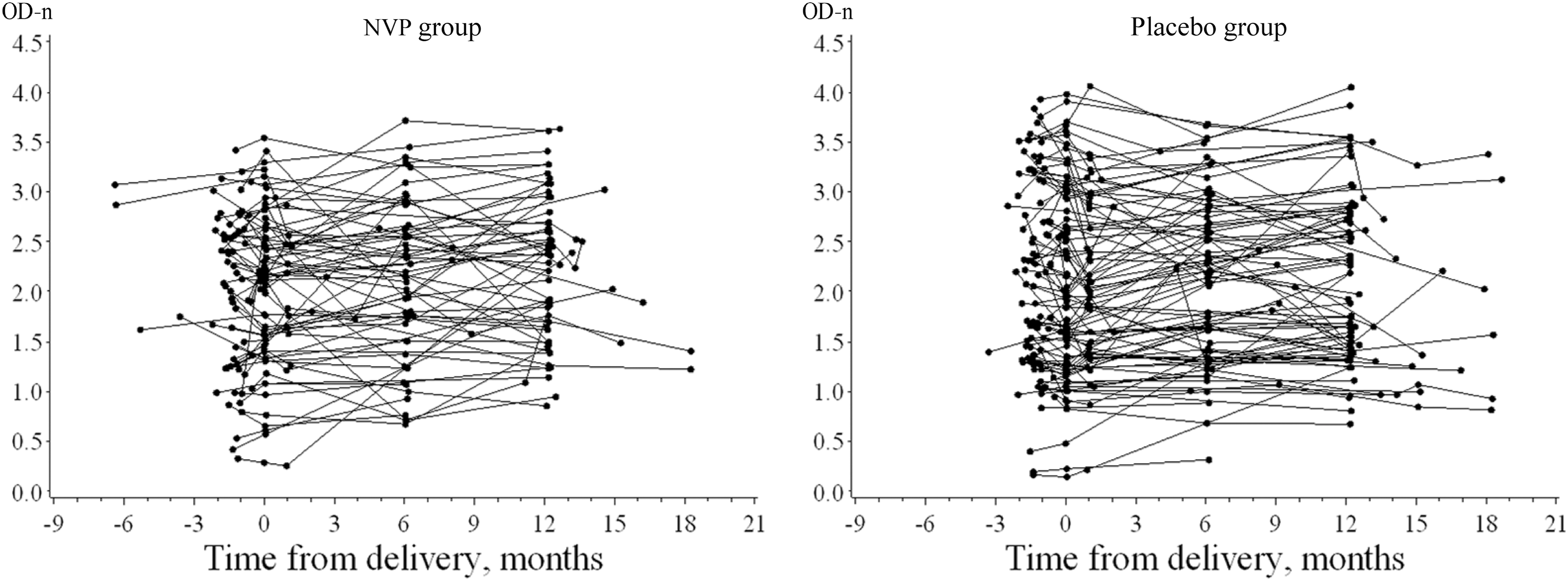
Individual optical density (OD-n) levels over time, by treatment group.
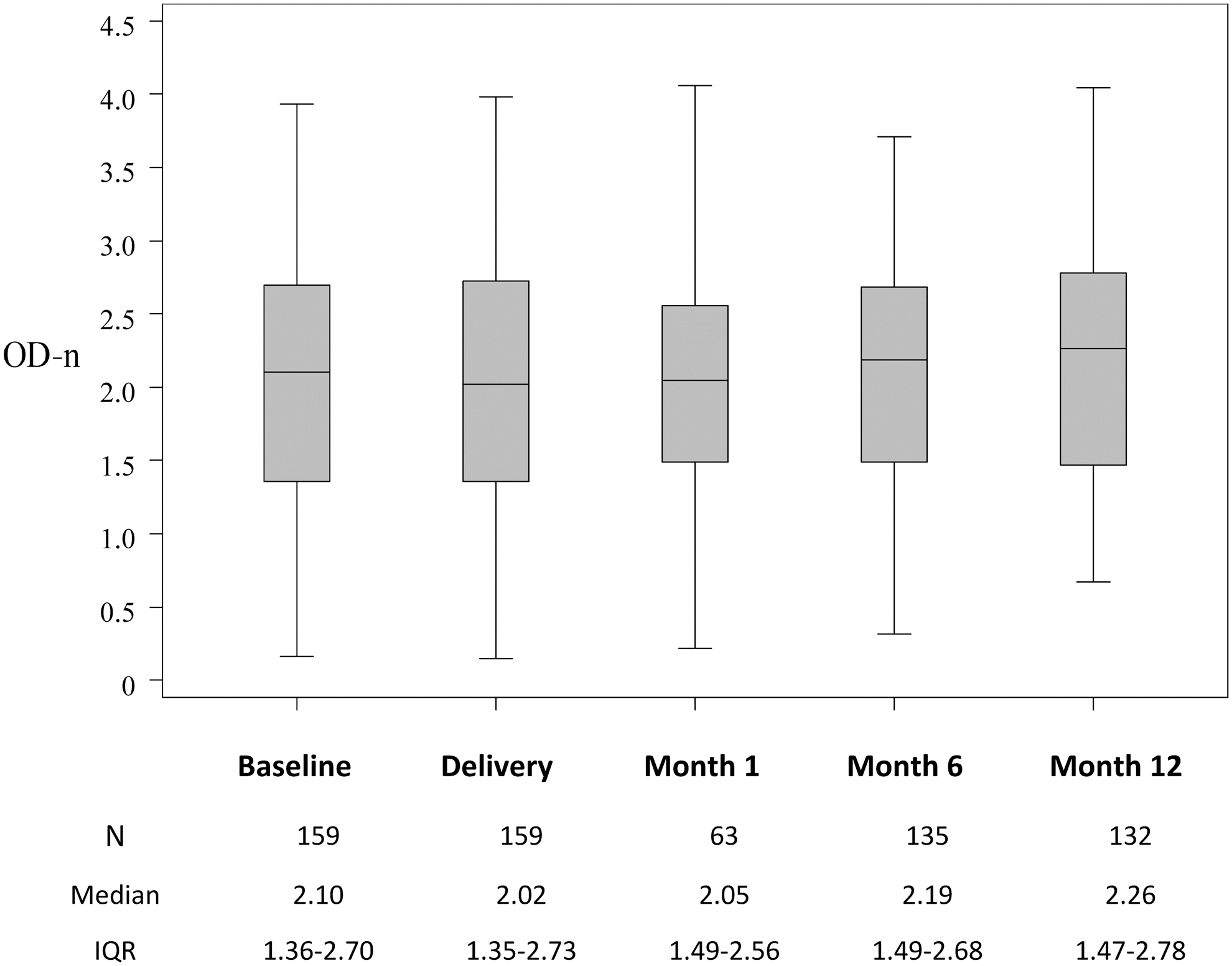
Boxplots of OD-n levels over time.
After receiving short-course ZDV, among 159 subjects, the OD-n levels decreased from baseline to delivery in 93 (58%) subjects (median change −0.034; p=0.039), suggesting that short-course ZDV may decrease OD-n levels. HIV RNA levels significantly decreased (median change −0.69 log10, p<0.0001) and CD4 count significantly increased (median change 61, p<0.0001) while on short-term ZDV. HIV RNA levels and/or CD4 cell counts at baseline did not appear to be predictive of the likelihood of having decreasing BED levels, through either univariate models (all p>0.8) or multivariate models (all p>0.6).
We then examined the effect of sdNVP on OD-n levels. Figure 4 presents the mean BED OD-n levels with 95% confidence intervals at baseline, delivery, and 1, 6, and 12 months after delivery, separately for subjects in the NVP group and in the placebo group. Because sdNVP was given during labor, we restricted our analyses to BED OD-n levels at and after delivery. The OD-n levels at delivery, changes from delivery at 1 month, 6 month, and 12 month were similar between the NVP group and the placebo group (Table 2, all p>0.4). Mixed-effect modeling revealed that sdNVP did not have an effect on either the average of all BED levels postdelivery (p=0.83) or the trajectories of these values (p=0.45). However, sdNVP appeared to modify the association between CD4 count at delivery and OD-n levels postdelivery (p=0.01). In the placebo group, we observed a positive association between CD4 count at delivery and OD-n levels postdelivery (p=0.028), controlling for HIV-1 RNA levels and OD-n levels at delivery; this association was no longer seen in the NVP group (p=0.14). Higher HIV-1 RNA levels at delivery were associated with higher average OD-n levels postdelivery (p=0.0013), independently of OD-n levels at delivery and CD4 count at delivery.
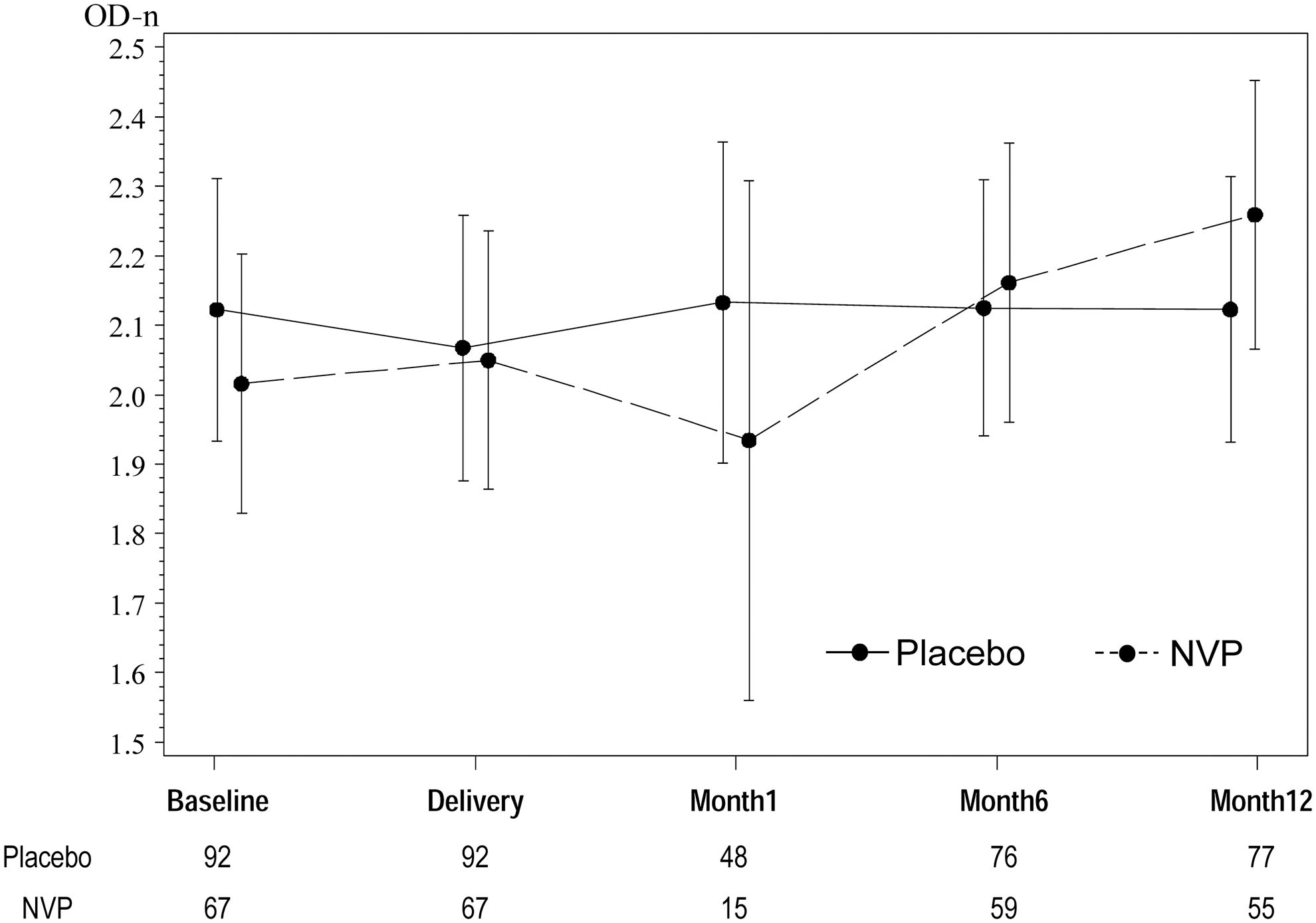
Mean and 95% confidence intervals for OD-n levels over time, by treatment group.
Wilcoxon rank-sum p-value.
We estimated a linear slope for each patient to measure the linear trends in OD-n levels as a function of time (in months) since delivery. The OD-n slopes within the placebo group ranged from −0.10 to 0.34, with median 0.005 [IQR: (−0.01, 0.03)]. The OD-n slopes within the NVP group ranged from −0.08 to 0.19, with median 0.007 [IQR: (−0.02, 0.04)]. Consistent with the results from the random effect models, no statistically significant differences in the slopes between the two groups were seen (p=0.86); that is, sdNVP did not affect the linear trends in OD-n levels postdelivery. There were 29 (43%) subjects with flat or negative OD-n slopes within the NVP group and 36 (39%) subjects with flat or negative OD-n slopes within the placebo group. This difference did not reach statistical significance (p=0.63). However, the association between OD-n slopes after delivery and CD4 count at delivery differed by treatment group (p=0.005). As illustrated in Fig. 5, within the placebo group, higher CD4 count at delivery was significantly associated with larger OD-n slopes (p=0.0002). However, this association disappeared within the NVP group (p=0.86).
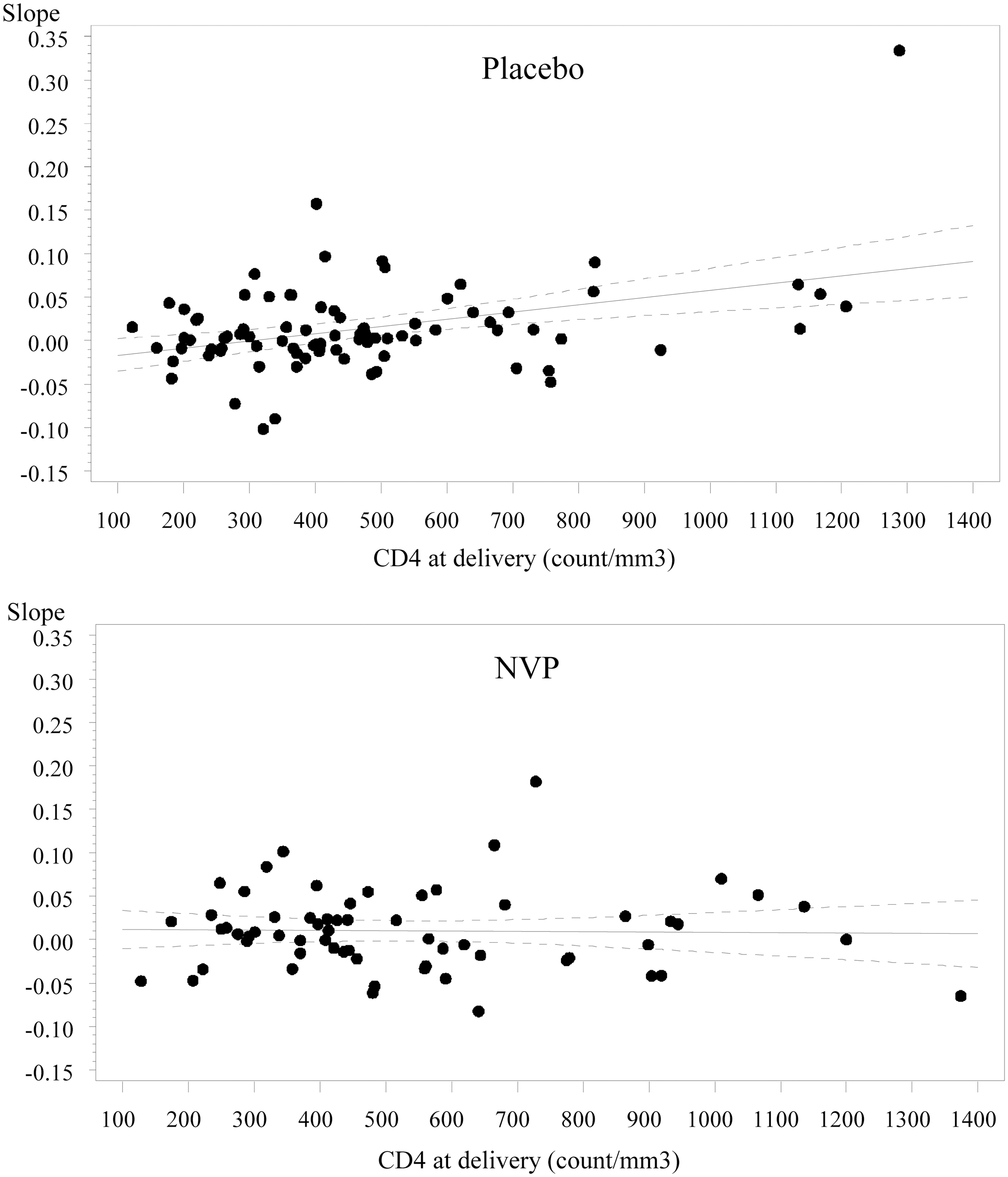
Trajectories of OD-n levels postdelivery versus CD4 count, by treatment group.
Using samples from the Mashi study of pregnant HIV-infected women in Botswana, we found that BED immunoassay results were decreased by short-term ZDV. While sdNVP did not affect the average and trajectory of OD-n levels postdelivery, it appeared to modify the association between CD4 count at delivery and OD-n levels postdelivery. Although our study population consists of pregnant women only, results for BED optical density were found to be similar for women who are pregnant and those who are not. 23
Consistent with previous studies, 10,24 we found that higher HIV-1 RNA levels were associated with higher OD-n levels. Because our study consists of only women, and all in their twenties, we were not able to assess the effect of age or gender on OD-n levels.
One limitation of this work is that in the current study, all women received short-term ZDV. The effect of ZDV was inferred by comparing it to the expected general increasing trend in OD-n levels in the absence of antiretroviral treatment and in early stage of HIV infection. It would be useful to compare the changes in BED levels to those who did not receive ZDV, although it might be infeasible.
In conclusion, our study suggests short-term ZDV, similar to HAART, 14 decreases BED levels in HIV-1 subtype C-infected pregnant women. Special care is needed when using the BED assay to estimate HIV incidence in order to reduce bias. We recommend an assessment of the exposure to ZDV or PMTCT drugs when estimating HIV incidence among pregnant women. While sdNVP at delivery did not appear to affect OD-n levels postdelivery among women who had exposure to ZDV, the modification effect of sdNVP on the association between CD4 count and OD-n levels calls for further investigation.
Footnotes
Acknowledgments
We thank the subjects, investigators, and staff who participated in the Mashi study. We also thank Dr. Mauro Schechter and a referee for their comments, which improved the article. We dedicate this article to our friend and colleague, Dr. Stephen W. Lagakos, who inspired the work and provided valuable insights into the design of this study. R.W. and D.P.'s work was supported by grant R01 AI 24643 from the National Institutes of Health. C.D.B.'s work was supported by grant R01 AI51164 from the National Institutes of Health. S.M.'s work was supported by the AIDS International Training and Research Program (AITRP).
Author Disclosure Statement
No competing financial interests exist.