
Abstract
Several microbicides, including nonoxynol-9 (N-9) and cellulose sulfate (CS), looked promising during early trials but failed in efficacy trials. We aimed to identify Phase I mucosal safety endpoints that might explain that failure. In a blinded, randomized, parallel trial, 60 healthy premenopausal sexually abstinent women applied Universal HEC placebo, 6% CS or 4% N-9 gel twice daily for 13½ days. Endpoints included immune biomarkers in cervicovaginal lavage (CVL) and endocervical cytobrushes, inflammatory infiltrates in vaginal biopsies, epithelial integrity by naked eye, colposcopy, and histology, CVL anti-HIV activity, vaginal microflora, pH, and adverse events. Twenty women enrolled per group. Soluble/cellular markers were similar with CS and placebo, except secretory leukocyte protease inhibitor (SLPI) levels decreased in CVL, and CD3+ and CD45+ cells increased in biopsies after CS use. Increases in interleukin (IL)-8, IL-1, IL-1RA, and myeloperoxidase (MPO) and decreases in SLPI were significant with N-9. CVL anti-HIV activity was significantly higher during CS use compared to N-9 or placebo. CS users tended to have a higher prevalence of intermediate Nugent score, Escherichia coli, and Enterococcus and fewer gram-negative rods. Most Nugent scores diagnostic for bacterial vaginosis were in N-9 users. All cases of histological inflammation or deep epithelial disruption occurred in N-9 users. While the surfactant N-9 showed obvious biochemical and histological signs of inflammation, more subtle changes, including depression of SLPI, tissue influx of CD45+ and CD3+ cells, and subclinical microflora shifts were associated with CS use and may help to explain the clinical failure of nonsurfactant microbicides.
Introduction
V
Several microbicide candidates looked promising during preclinical evaluation but failed in efficacy trials: nonoxynol-9 (N-9), 2 –7 Carraguard, 8 BufferGel, 9 PRO 2000, 10 and cellulose sulfate (CS). 11 –19 CS did not prevent, and, when frequently used, may have increased the risk of HIV acquisition. 20,21 N-9, also when used frequently, raised the risk of HIV infection. 7 The first promising results for a microbicide came from the CAPRISA 004 study, in which tenofovir (TFV) 1% vaginal gel used before and after heterosexual intercourse was found to be 39% effective in reducing a woman's risk of becoming infected with HIV and, unexpectedly, 51% effective in preventing genital herpes infections. 22 A subsequent trial of vaginal TFV 1% gel with a different population and a daily dosing regimen [the Microbicide Trials Network's Vaginal and Oral Interventions to Control the Epidemic (VOICE) trial] did not show efficacy likely due to poor adherence. 23 A pivotal Phase III HIV prevention study with pericoital dosing, the Follow-on African Consortium for Tenofovir Studies (FACTS 001), is underway to confirm the findings from CAPRISA 004.
Product development would be greatly enhanced if candidates that might fail to prevent HIV transmission could be detected earlier in the process. Safety endpoints in Phase I trials of microbicide candidates have included epithelial disruption, changes in microflora and vaginal immunity [soluble markers, cellular markers, antimicrobial activity in cervicovaginal lavage (CVL)], and the presence of inflammation on biopsy. The purpose of the present study was to reevaluate these endpoints using two products with known failure in Phase II/III trials representing both a detergent-based product (N-9) and a nondetergent product (CS), in the hope of identifying safety signals that could have predicted the lack of clinical efficacy.
Materials and Methods
Ethics statement
This study conformed to the principles of the Declaration of Helsinki. The participants took part voluntarily and signed informed consent forms. The study was reviewed and approved by each site's institutional review board.
Study design and endpoints
This was a CONRAD-sponsored and monitored, blinded, randomized, placebo-controlled study in 60 healthy, sexually abstinent women [30 in each of two centers: Eastern Virginia Medical School (EVMS), Norfolk, VA, and the University of Pittsburgh/Magee-Womens Hospital, Pittsburgh, PA].
Women were evaluated before, during, and after 13½ consecutive days of twice-daily vaginal applications of either the Universal HEC (hydroxyethylcellulose) Placebo, 24 4% N-9 gel (Conceptrol), or 6% CS for the following parameters:
1. Soluble markers of inflammation in the CVL supernatant;
2. Cellular markers of inflammation in the CVL cell pellet and cervical cytobrush samples;
3. Inflammatory infiltrates in biopsied vaginal tissues;
4. Urogenital microflora (vaginal pH, Nugent scores, wet mounts, dipstick urinalyses, urine cultures, and semiquantitative cultures of Lactobacillus H2O2 + , Lactobacillus H2O2 − , Escherichia coli, Candida, Gardnerella vaginalis, Staphylococcus aureus, Enterococcus, anaerobic gram-negative rods, Ureaplasma, and Mycoplasma);
5. Epithelial integrity based on naked eye examination, colposcopy, and histology;
6. Antiviral activity in the CVL after in vivo exposure to product; and
7. Adverse events (AEs)
Participants were women aged 18–50 years, not pregnant or breastfeeding, in good health with regular menstrual cycles, willing to abstain from intravaginal product use and vaginal activity during the study, protected from pregnancy by sterilization of either partner, and not using hormonal contraception or an intrauterine device (IUD). Symptomatic vaginal or urinary tract infection, a positive test for Trichomonas vaginalis, Neisseria gonorrhoea, or Chlamydia trachomatis, or an abnormal Pap test at screening, or use of systemic corticosteroid therapy or antibiotic, antifungal, or antiviral drugs just prior to enrollment were exclusion criteria. Each volunteer was seen in six visits across two menstrual cycles (Fig. 1): Visit 1 (screening), Visit 2 (in the luteal phase, about 14 days after menses ended, in Cycle 1), Visit 3 (just after menses ended in Cycle 2; product dispensed), Visit 4 (day after 13th use), Visit 5 (day after last use, approximately matched by cycle day with Visit 2), and Visit 6 (3 days after last use).
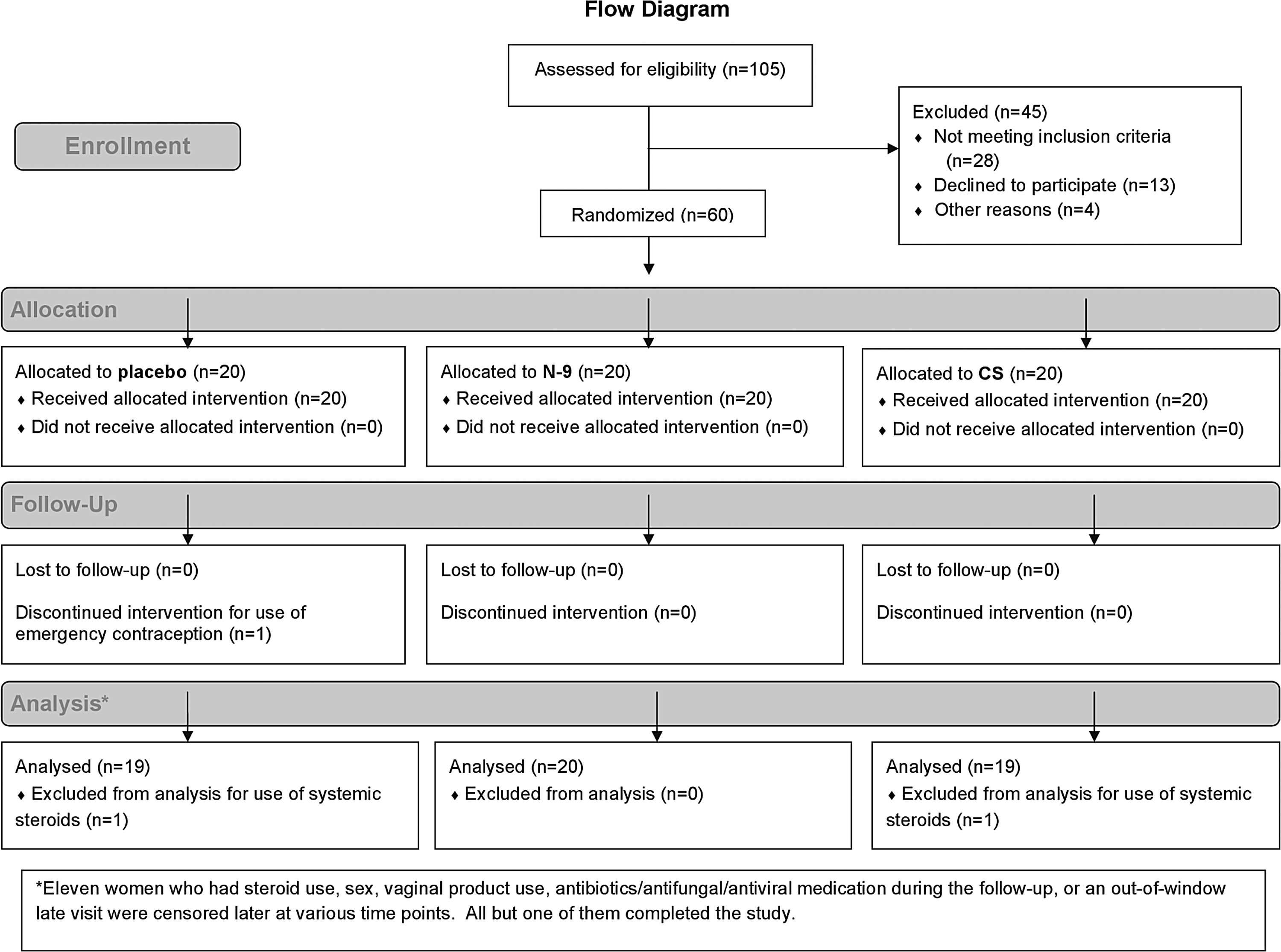
Flow diagram of study enrollment.
Naked eye genital tract examinations, colposcopies, CVLs using 10 ml of normal saline, Nugent scores, semiquantitative vaginal cultures, and vaginal pH measurements were performed at Visits 3 (baseline), 4, 5, and 6, as previously described. 12 Vaginal biopsies and endocervical cytobrush specimens were obtained at Visits 2 (baseline) and 5 as previously described. 25 Adverse events were assessed throughout follow-up. Although participants were to refrain from coitus, a test for seminal fluid was performed at visits at which CVLs were collected because seminal fluid can affect assays of microbicidal activity. 26 The clinical sites processed the CVLs by centrifuging and freezing the supernatant at −80°C for biomarker assessment while preserving the cell pellet for immunocytochemistry as previously described. 1
The Universal HEC Placebo (ReProtect, Baltimore, MD) is a water-based gel containing HEC, sodium chloride, sorbic acid, and sodium hydroxide. It was developed for use as an inert comparator in clinical trials of vaginal microbicides and was designed to be nonreactive and to approximate the physical properties of candidate active products. 24
CS (Patheon, Mississauga, Ontario) 6% (60 mg/g) is formulated in a water base with benzyl alcohol, glycerin, sorbitol, and carbomer.
Conceptrol (Ortho-McNeil Pharmaceutical Corp., Raritan, NJ) contains 4% N-9 in a base containing lactic acid, methyl paraben, povidone, propylene glycol, purified water, sodium carboxymethyl cellulose, sorbic acid, and sorbitol solution.
Placebo and CS were packaged in identical 3.5 ml single-use applicators. Due to the high cost of repackaging Conceptrol, it was provided as commercially supplied in 3.0-ml single-use applicators very similar to those used for the placebo and CS. Overwraps were identical for all three products. Participants were instructed to insert one applicator of their assigned gel twice daily, at bedtime and after her first urination upon arising for the day, beginning the evening of Visit 3 and ending the evening before Visit 5, for a total of 27 doses. Product use, menses, and adverse events were recorded in a study diary.
FHI 360 biostatisticians used the random permuted blocks method to generate random allocation sequences using a verified SAS program (SAS Institute, Cary, NC). Treatment assignments were made according to these allocation sequences in a 1:1:1 ratio and were concealed within sealed envelopes until the moment of randomization. Participants were enrolled by clinic staff at the two sites. The participants, investigators, analysts, and other study staff were masked to treatment assignment.
Statistical methods
Biostatistical analysis was performed by FHI 360. All participants except those with no follow-up data or with protocol violations affecting measurements (e.g., steroid use) contributed to the analysis. Data obtained after steroid use or a positive test for semen, from out-of-window visits, and after antibiotic use (for microflora), were excluded.
Most objectives were evaluated descriptively. Due to nonnormal distributions, statistical comparisons between product groups on change scores (follow-up visit minus baseline) were conducted using nonparametric tests, specifically Exact Kruskal–Wallis or Mann–Whitney–Wilcoxon tests, with Monte Carlo estimation. In general, between-group comparisons are not reported unless the overall test (across all groups) was significant at alpha=0.05.
Sample size was not based on statistical considerations but on what could be feasibly accomplished in a Phase I trial of this type. All p-values are two-tailed, unadjusted for multiple analysis given the exploratory, hypothesis-generating nature of the study. Statistical tests are exploratory; results should be interpreted cautiously in light of the large number of tests and low statistical power.
Laboratory methods
Gram stains and semiquantitative cultures were assessed at Dr. Sharon Hillier's laboratory as described previously. 27,28 Semiquantitative growth was correlated to quantitative log growth with 1+corresponding to 102–104 colony forming units (CFUs), 2+= 105, 3+= 106, and 4+= 107–108. 29
Prior to anti-HIV-1 assaying, the CVL supernatants were γ-irradiated. 30 Anti-HIV-1 activity was assayed at Dr. Charlene Dezzutti's laboratory in 1:8 diluted CVLs using an established TZM-bl reporter cell line as previously described. 31 CVL toxicity to the TZM-bl cells was measured in parallel cultures using CellTiter-Glo (Promega). HIV-1 infectivity was determined for each CVL as a percent of the HIV-1-only control. BaL was purchased from Advanced Biotechnologies, Inc. (Columbia, MD). LAI was grown in PM1 cells. Viral titers were determined using the Reed Muench method. 32 Infection with HIV-1 was measured in TZM-bl cells by BrightGlo (Promega) per the manufacturer's instructions. 31 Percent inhibition is calculated by correcting for background luminescence (cells only) and comparing treatment to the HIV-1 only control.
The following biomarkers of inflammation were measured by ELISA in CVLs by Dr. Raina Fichorova's laboratory as previously described 33,34 : proinflammatory mediators interleukin (IL)-1α, IL-1β, IL-6, IL-8, and myeloperoxidase (MPO), and antiinflammatory protective mediators secretory leukocyte protease inhibitor (SLPI), and IL-1 receptor antagonist (IL-1RA). All assays were from R&D Systems (Minneapolis, MN), except IL-1α (Pierce Endogen, Rockford, IL) and MPO (Assay Designs, Ann Arbor, MI).
Immune cell markers (CD45, CD3, CD68, and NF-κB) were assessed in the CVL pellets, cytobrush specimens, and cervicovaginal tissues by Dr. Gustavo Doncel's laboratory using immunochemistry techniques as previously described. 1,34 Briefly, CVL and cytobrush cell pellets were isolated, resuspended, and counted using a Neubauer's chamber. Cells were spotted on eight-well slides, air dried, fixed in methanol, and stored frozen. Later, they were immunostained using anti-CD45 and CD68 monoclonal antibodies (Zymed Laboratories, Inc., San Francisco, CA), anti-CD3 monoclonal antibody (Leica Biosystems Newcastle Ltd., Newcastle upon Tyne, UK), and anti-NF-κB monoclonal antibody [Chemicon (now Millipore), Temecula, CA]. After incubation, cells were washed and further incubated with Super Sensitive Detection System (Biogenex, Napa, CA). The slides were then stained with Fast Red substrate and chromogen (Dako, Carpinteria, CA), washed, and mounted. Positively stained cells appear red and were counted from different areas (∼200 cells per slide) under an E800 Nikon microscope. The number of cells recovered in cytobrushes was lower than expected, so only CD45+ cells were used in the statistical analysis.
Vaginal tissues were fixed in buffered formalin and embedded in paraffin for histopathological and immunohistochemical evaluation. For immunostaining, slides were deparaffinized, dehydrated, and rehydrated followed by antigen retrieval in citrate buffer (pH 6.2) at 95°C for 30 min. They were then cooled down and washed with phosphate-buffered saline (PBS). To prevent nonspecific binding, 1.5% normal horse serum was used. This was followed by incubation with specific antibodies overnight at 4°C. Thereafter, secondary reactions followed either the Biogenex or ABC recommended protocols. The antigen was localized by incubation with either AEC chromogen (ScyTek labs, Logan, UT) or Fast red substrate and chromogen (Dako, Carpinteria, CA). Positively stained cells were counted using an E800 Nikon microscope and expressed as number of cells/mm2.
Results
Sixty participants were enrolled between December 20, 2007 and May 22, 2008, and the last participant was exited on July 5, 2008 (Fig. 2). All completed the study except one participant in the placebo group who was discontinued early for use of emergency contraception. Two (one in the placebo group and one in the CS group) were completely excluded from analysis for using oral steroids prior to randomization. Of the 58 in the analysis, three with positive semen tests contributed data up to the visit with the positive test.
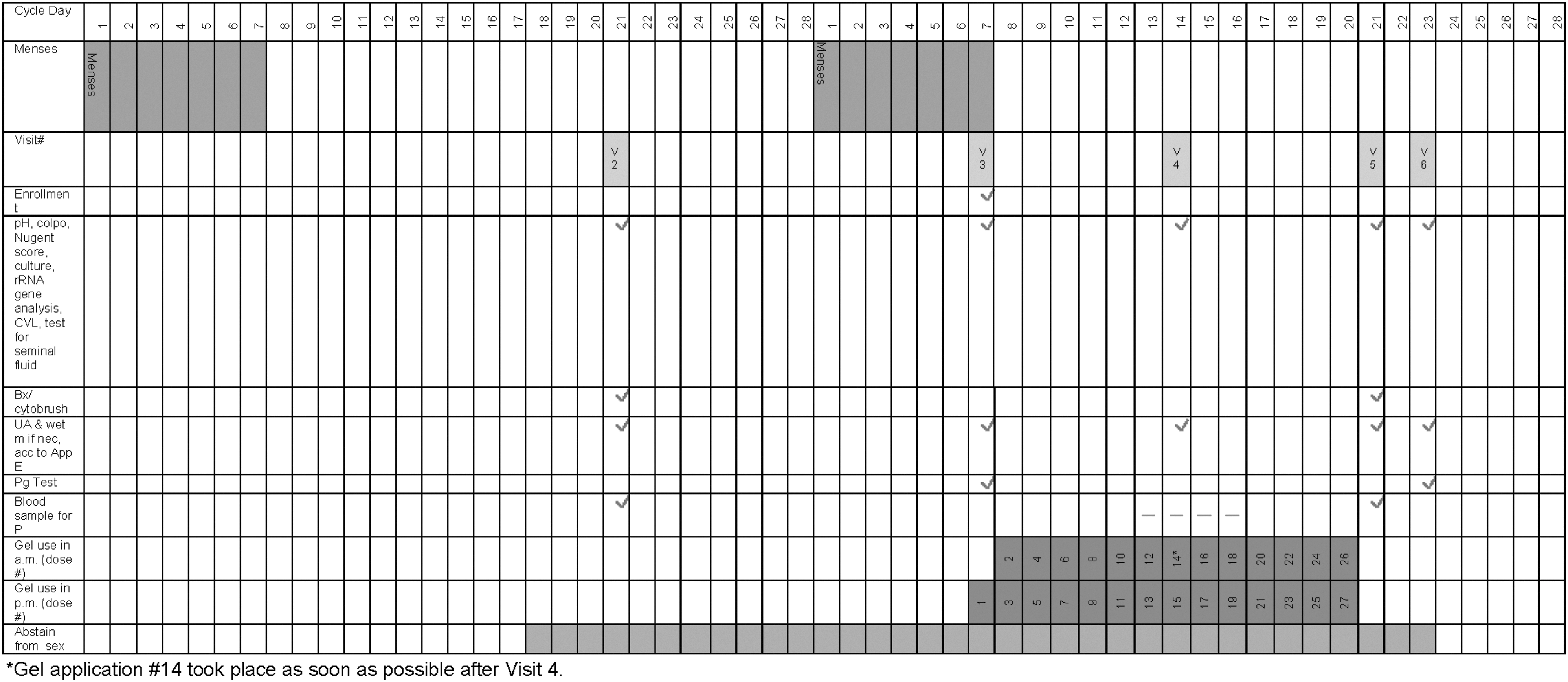
Schedule of visits, starting with visit 2, for women enrolled in a clinical safety trial of 13½ days use of cellulose sulfate, nonoxynol-9, or the Universal HEC placebo. The example is for a woman with 28-day cycles and 7-day menses.
Participants were 21–50 years old (mean=34.9), about 50% white and 40% black, with a mean education of 14.4 years. Eighty percent had ever been pregnant. Demographics are shown in Table 1.
CS, cellulose sulfate; N-9, nonoxynol-9.
Most participants (90–95% across groups) reported using at least 24 of the 27 applicators.
Soluble markers of inflammation
CS use induced a pattern of change from baseline not significantly different from that of HEC placebo with three exceptions (Table 2 and Supplementary Table S1; Supplementary Data are available online at
CS, cellulose sulfate; N-9, nonoxygenol-9; SLPI, secretory leukocyte protease inhibitor; IL, interleukin; MPO, myeloperoxidase.
N-9 use induced a different pattern, showing a tendency toward an increase in the proinflammatory mediators IL-1α, IL-1β, IL-8, and MPO on all visits, all being significantly different from placebo on Visit 4 and IL-1α different from placebo on all visits. Similar to CS use, N-9 use was associated with depressed SLPI throughout the study, which was significantly different from placebo only during dosing. The IL-1RA-to-IL-1 (α+β) ratio showed the strongest depression in the N-9 users at Visit 4 and remained negative despite the tendency toward increasing IL-1RA at Visits 5 and 6. IL-1RA increased in the N-9 group and decreased in the placebo group with the difference being statistically significant at Visit 5. The N-9 group was significantly different from the CS group for most parameters at Visits 4 and 5, and for three parameters at Visit 6, with generally fewer proinflammatory changes in the CS group.
Immune cell markers in the CVL cell pellet and in cytobrush specimens and epithelium of biopsied vaginal tissue
In cell pellets, CS use induced a pattern of change from baseline in immune cell markers similar to placebo with the following exceptions (Table 3 and Supplementary Table S2): (1) At Visit 4 the median ratio of CD45+ cells (leukocytes) to CD45+ cells at baseline was significantly higher for placebo than CS, reflecting a marked drop in the number of CD45+ cells in the CS group; and (2) at Visit 5, CD45+ and CD68+ cells dropped in the CS group but increased in the placebo group. N-9 use generally induced a pattern of immune cells more suggestive of inflammation than CS or placebo. CD45+ cells were increased at Visits 4 and 6, in comparison with placebo, but the difference was statistically significant only at Visit 4. There was a greater increase in epithelial cells expressing the proinflammatory transcription factor NF-κB in the N-9 group at Visits 4 and 5, but this difference was statistically significant only when compared to CS. There were no statistical differences among the groups in the change in CD3+ T cells in the CVL cell pellets.
In vaginal biopsies taken at Visit 5 (Table 4 and Supplementary Table S3), CS use was associated with an increase from baseline in intraepithelial CD45+ and CD3+ cells that was statistically significant compared with the placebo group, in which there was a decrease. Unexpectedly, there was a reduction in the number of intraepithelial CD45+ cells in the N-9 group; however, this was not significantly different from placebo or CS.
Antiviral activity of the CVL supernatant after exposure to product
Baseline CVLs did not suppress HIV-1 infectivity in any group (Table 5). Midway through dosing, the infectivity of HIV-1LAI and HIV-1BaL was significantly lower in the presence of the CVL from CS users as compared with that from N-9 or placebo users. The infectivity of HIV-1LAI was also significantly lower in the presence of the CVL from N-9 users than from placebo users. Three days after dosing, no anti-HIV activity was noted in both treatment groups suggesting no drug remained. Cell viability was high (>90%) in all three groups, although it was slightly decreased in the CS and N-9 groups as compared to placebo at Visit 4 and in the CS group at Visit 6.
Percentage inhibition above 100% indicates greater HIV infection compared to the control, while values below 100% indicate less HIV infection compared to the control.
Urogenital microflora (vaginal pH, Nugent scores, semiquantitative vaginal cultures, wet mounts, dipstick urinalyses, and urine cultures)
The largest changes from baseline in pH were in the N-9 group, with increases of 0.9 units at Visit 4 and 0.8 at Visit 5 (Table 6 and Supplementary Table S4). A 0.3 unit increase was seen in the CS group at Visit 4 that was significantly different from placebo.
Although several subjects had Nugent scores diagnostic for bacterial vaginosis (BV) across various study visits (most commonly in the N-9 group), only one placebo subject had clinically diagnosed BV (Table 7).
Baseline is visit 3 unless data are missing, in which case it is visit 2.
Gram stains were batched and run at the end of the study; a normal Nugent score was not an entry criterion. Women with two out of four Amsel's criteria at visit 1, 2, or 3 were not enrolled.
There were few significant differences among groups in change from baseline in semiquantitative cultures (data not shown). E. coli increased by 2.5 and 2.0 points in the CS group (Visits 4 and 5), which was significantly greater than the change in the placebo group (p=0.0046 and 0.0134, respectively). Enterococcus increased by 1.0 point on Visit 5 in the CS group, which was significantly greater than the change in the placebo group as well as the N-9 group (p=0.0085 and 0.0036, respectively). An ad hoc analysis showed no correlation between CD3+ and CD45+ in tissue and E. coli or Enterococcus in the semiquantitative cultures.
Gram-negative rods decreased by 0.5 points in the CS group and increased by 1 point in the N-9 group at Visit 4 but did not change in the placebo group (p=0.0138 and 0.0065; N-9 vs. placebo, CS, respectively); no significant differences were seen at Visits 5 or 6. At Visit 6, the Mycoplasma score decreased from baseline in the CS group but increased in the N-9 group (p=0.0096).
There were two abnormal wet mounts at follow-up: one diagnostic of BV (placebo group) and one diagnostic of candidiasis (CS group) at Visit 5. There was one abnormal urine dipstick result along with a positive urine culture in one woman (Visit 4, N-9 group).
Epithelial integrity based on colposcopy and histology
The largest numbers of colposcopic findings and proportion of women with colposcopic findings were in the N-9 group (Supplementary Table S5). The difference in the proportion of women with findings in the N-9 group (47.4%) and the placebo group (11.8%) was statistically significant at Visit 4 (p=0.031). During follow-up most of the findings were on the cervix and involved erythema, petechiae/ecchymoses, or peeling in that approximate order. There were no colposcopically observed deep epithelial disruptions during dosing (Visit 4), two on the day after dosing (Visit 5, both in the N-9 group), and one in each group 3 days after dosing (Visit 6).
Four of the five histologically abnormal findings, all four histological findings of inflammation, and both histological findings of deep epithelial disruption after product use were in the N-9 group, with none in the CS group (Supplementary Table S6).
Overall agreement between colposcopy and histology was good (88.1% of biopsies), with disagreement most common (9.5% of biopsies) due to normal pathology in an area with a clinical finding.
Adverse Events (AEs)
The most common genital AEs were pruritus and metrorrhagia (data not shown). The largest proportion of women reporting product-related genital AEs was seen midway through dosing (Visit 4) in all groups (N9, 35.0%; CS, 31.6%; placebo, 15.8%).
Discussion
In this study, N-9 was clearly proinflammatory, as expected, 35 while CS was generally not proinflammatory and differed only minimally from placebo as previously shown in a Phase I study with a more limited set of inflammatory endpoints. 12 However, CS was associated with a decrease in the protective factor SLPI, a parameter not assessed in earlier CS studies. A similar effect was seen in early trials of other microbicide candidates later found in Phase III trials not to be effective. A single dose of N-9 did not cause significant changes in soluble mediators except for a decrease in SLPI 12 h after the dose. 35 However, in the same study, three doses of N-9 led to an obvious inflammatory condition indicated by significant increases in IL-1α/β, IL-8, MIP-1β, TNF-RII, and neutrophil elastase, as well as decreases in SLPI and the ratio of IL-1RA to IL-1. Another study of 3-day use of N-9 showed a reduction in SLPI compared with baseline, although a statistical comparison was not performed. 36
Other nonspecific broad-spectrum anti-HIV microbicide candidates including PRO 2000, BufferGel, and Carraguard, which were not effective at preventing HIV infection in clinical trials, also showed decreases in SLPI. 37 –39 Of note, in a 14-day study of the TFV vaginal gel, no significant effect was seen for a group of soluble mediators, including SLPI, although for statistical reasons a threshold p-value of <0.01 rather than <0.05 was used. 40 We have recently reported that a decrease in SLPI in cervical secretions was associated with subsequent HIV infection in a cohort of HIV-seronegative women at risk of acquiring the infection through heterosexual intercourse (unpublished data presented by Morrison et al. at CROI 2012 as Paper #1052, “Biomarkers of cervical inflammation and immunity associated with hormonal contraception, pregnancy and HIV-1 seroconversion”). Taken together, the current study and prior studies suggest that depression of SLPI may represent an early signal of compromised vaginal safety, especially when lower doses of detergent or less invasive products such as CS are applied.
Two published studies evaluated cellular markers. Three doses of N-9 were associated with an influx of polymorphonuclear neutrophils into the cervicovaginal secretions, as well as an increase in CD68+ cells. 35 VivaGel was associated with a trend toward an increased number of CD8+/CD69+ activated T cells after 7 days of twice-daily use, and a higher number of CD11+/DC-SIGN+ cells after 21 days of use. 41 In the present study, CS was associated with a decrease in CD45+ and CD68+ cells in the CVL cell pellet during dosing. Leukocyte trafficking into the vaginal lumen may have been impaired by CS. Alternatively, the decrease among CS users may have been due to cells being trapped and disrupted in the cell pellet by the gel.
In contrast, the median change from baseline in CD45+ and CD3+ cells in the vaginal epithelium among CS users was significantly greater than that of both placebo users and N-9 users. This increase in tissue leukocytes and T cells in particular suggests a possible increase in HIV susceptibility and may be another marker for future use, although the lack of effect of N-9 needs further investigation.
It cannot be entirely ruled out that the lack of increases in proinflammatory mediators after CS use was due to gel interference with the production of mucosal secretions in vivo. It has been demonstrated that other similar polyanions interfere with epithelial secretion of cervicovaginal innate and inflammatory factors. 42 The polyanionic microbicide compounds dextran sulfate and polystyrene sulfonate significantly inhibited cytokine mRNA and protein levels of proinflammatory (IL-8 and IL-1beta) and antiviral (beta interferon) cytokines following epithelial cell stimulation with TLR ligands Pam(3)CSK(4), MALP-2, or poly(I:C). These activities were associated with the sulfate/sulfonate moieties of the polyanionic compounds, since the unsulfated dextran control did not show any effects. In support of this notion in this study, inflammatory tissue infiltrates were observed in the CS group in the absence of increased proinflammatory markers in the CVL.
In a previous study, evaluation of antimicrobial activity was performed using CVLs collected after three doses of N-9. When they were incubated with HIV latently infected cells, there was an induction of HIV replication, which reached a maximum (about a 10-fold increase) in CVLs collected 60 h after N-9 administration. 35 Administration of PRO 2000 resulted in no loss of anti-HSV, anti-HIV, or antibacterial activity in the CVL. 37 In this study, antiviral testing suggested that CS retained its antiviral activity in the vaginal environment for at least 8–18 h after dosing and had no apparent detrimental effect on endogenous defenses after dosing was discontinued. A limitation of our study is that we did not measure CS levels in the CVLs. Antiviral activity was seen to persist in the vaginal environment of PRO 200037 and tenofovir 40 users; in those studies, levels of drug in the CVL were measured.
Using cell line readouts rather than tissue explants is a limitation since those assays do not cover the full spectrum of innate immunity regulation of HIV infectivity and replication that could be excreted by the soluble compartment of the cervicovaginal secretions. However, the TZM-bl assay provides a good assessment of virucidal agents such as N-9 and HIV entry inhibitors, e.g., CS, and thus served the purpose of evaluating the residual drug activity in the CVL. The data are presented as percentage control to standardize multiple replicates. Several publications demonstrate the utility of the TZM-bl assay for this work. 37,40,43 –46 The use of mucosal tissue is not reproducible or feasible to evaluate several hundred CVL samples.
The slight increase in vaginal pH among CS users may be attributed to the CS gel having a pH of 7.5 compared with 4.4 for placebo, but CS's limited buffering capacity makes it unlikely that it would significantly alkalinize vaginal pH, thus leaving the possibility that change resulted from subtle microflora changes.
In a 14-day study, CS use was associated with increases in E. coli compared with placebo. 12 In the present study, CS use was associated with increases in E. coli and Enterococcus. The reduction of SLPI and MPO after CS use may explain the relative overgrowth of E. coli and Enterococcus. The vaginal bacterial community composition and its relative abundance in this study were also characterized using pyrosequencing of barcoded 16S rRNA genes as part of a separate analysis. 47 Treatment with CS and N-9 led to a shift in the microbiota toward a state comprised of strict anaerobes and low numbers of Lactobacillus sp. This alteration in the vaginal microbiome may create an environment more conducive to HIV infection. Furthermore, CS may affect the bacterial colonization patterns via direct interactions with the vaginal epithelium, as suggested by a recent in vitro study. 48 In that study, CS selectively reduced epithelium-associated bacterial CFUs and, to a lesser extent, planktonic CFUs, most significantly affecting L. crispatus. Triggering only minor changes in sterile epithelial cultures, CS induced expression of innate immunity mediators in microflora-colonized epithelia, most significantly potentiating effects of bacteria causing BV, such as Prevotella bivia.
In previous studies, N-9 was associated with decreases in lactobacilli and increases in E. coli, Enterococcus, and anaerobic gram-negative rods. 49 –51 We found that N-9 was associated with increases in anaerobic gram-negative rods. The Universal HEC placebo was not associated in this study with changes from baseline in common vaginal flora and in agreement with the above-mentioned in vitro study of vaginal colonization contrasting the effects of HEC and CS. 52
More women with abnormal Nugent scores were seen in the N-9 group in this study and more women with intermediate Nugent scores were seen in CS group than the placebo group. Both abnormal and intermediate Nugent scores have been associated with a greater risk of HIV acquisition. This finding warrants further research. 52
Epithelial disruption has been seen fairly frequently among N-9 users but only rarely among users of other products. N-9 was associated with histological evidence of inflammation on biopsy in one study. 53 In the current study, N-9 was associated with more epithelial damage than CS and placebo, as evidenced by colposcopic and histological findings.
In summary, N-9 induced proinflammatory mediators and histological signs of inflammation and epithelial disruption in contrast to placebo and CS. CS had modest effects on some immune mediators but generally resembled the placebo. Importantly, CVLs from women using CS significantly reduced HIV-1 infection while CVLs from women using placebo or N-9 had no or limited activity.
Limitations of this study were its short duration, the absence of intercourse and accompanying physical trauma and effect of semen, 54 the lack of endometrial sampling, and the lack of tissue ex vivo infection data. Antiviral activity was not tested in the presence of semen and drug levels in the CVL were not obtained. It is possible that twice-daily exposure to the inactive ingredients in CS may have contributed to changes seen in some of these markers. All are Generally Regarded as Safe (GRAS) by the FDA and are used in other vaginal products, but their independent effects on these markers have not been studied. Finally, other factors involved in mucosal immunity of the genital tract were not studied, such as human defensins, two of which (HD5 and HD6) were found to antagonize the anti-HIV activity of CS in vitro, 55 and cell markers directly linked to HIV entry such CD4 and CCR5. 56
Although there are limitations to our findings, no prior studies have compared in a randomized fashion multiple clinical and laboratory tests using gels showing lack of efficacy and potential harm in Phase III trials, to better understand which markers are of benefit in the early study of a candidate vaginal microbicide. We found potentially useful markers of microbicide toxicity and possible clinical failure, specifically depression of SLPI, tissue influx of CD3+ and CD45+ cells, and subclinical vaginal microbiome changes including intermediate Nugent scores. Consideration should be given to these markers in early clinical testing of microbicides. Additional research should be done evaluating markers, especially when archived specimens taken prior to seroconversion are available from Phase III microbicide trials.
Conclusions
While the surfactant N-9 showed obvious biochemical and histological signs of inflammation, more subtle changes, including depression of SLPI, tissue influx of CD45+ and CD3+ cells, and subclinical microflora shifts were associated with CS use and may help to explain clinical failure of nonsurfactant microbicides.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.