
Abstract
Research supports the theory that the chronic infectious response occurring in periodontal disease may have a role as a risk modifier of systemic diseases. This study assessed the impact of HIV-associated chronic periodontitis treatment on systemic HIV-related markers (CD4 T lymphocytes cell counts and HIV viral load). Fifteen HIV patients presenting chronic periodontitis [at least eight sites presenting a probing depth (PD) >4 mm and bleeding] were included in this study. Patients received full mouth periodontal treatment with an ultrasonic device and supragingival plaque control. Medical (CD4 cell counts and HIV load) as well as periodontal clinical parameters [probing pocket depth (PPD), clinical attachment level (CAL)] were assessed at baseline and 3 and 6 months after treatment. ANOVA/Tukey and Pearson's correlation tests were used for statistical analysis (α=5%). The results showed that PPD reduction and CAL gain were statistically significant at 3 and 6 months after periodontal therapy (p<0.05). At 6 months, CAL gain was 0.6±0.5 mm and PPD reduction was 0.7±0.5 mm. At the same time, a statistically significant increase in CD4 cell counts could be seen after the third month (p<0.05) and sixth month (p<0.05). Moreover, at 6 months, the relationship between the improvement in clinical parameters, i.e., PPD reduction, and the number of TCD4 lymphocytes could be highlighted. This was shown as the greater the PPD reduction, the greater the increase in TCD4 cells (r=0.68, p=0.02). These data suggest that periodontitis treatment could be associated with an improvement in medical conditions in HIV subjects.
Introduction
B
Since the beginning of the AIDS epidemic, periodontal disease was described as one of the oral manifestations of HIV infection. 2 Periodontal pathology associated with HIV-infected patients can be classified into three distinct categories: (1) linear gingival erythema; (2) necrotizing ulcerative periodontal diseases, including necrotizing ulcerative gingivitis, necrotizing ulcerative periodontitis, and necrotizing ulcerative stomatitis; and (3) enhanced progression of chronic adult periodontitis. 3 Currently, it is accepted that periodontal disease in HIV patients is the same as that presented in non-HIV-infected patients. 4 However, immunosuppressed patients can exhibit a rapid onset and progression of the disease, depending on their immunological status. 5 Actually, researchers have been focused on determining the features, prevalence, microbiology, and host response characteristics of periodontal disease in HIV patients, especially as modified during the highly active antiretroviral therapy (HAART) era. 6
HAART has become a standard treatment for HIV infection, enrolling several medications for HIV control. It induces a marked reduction in viral load and an increase in the CD4 T cell count, leading to a decline in the morbidity and mortality of HIV-infected subjects. 7,8 Interestingly, along with numerous studies suggesting an impact of periodontal disease on systemic diseases, such as atherosclerosis, bacterial endocarditis, cardiovascular disease, diabetes mellitus, respiratory disorders, and complications of pregnancy, 9 –13 other coinfections in HIV individuals have been suggested to depreciate systemic health. It is established that chronic immune activation associated with coinfection by non-HIV pathogens (e.g., Pneumocystis jiroveci, Mycobacterium tuberculosis, and herpesviruses) 14 –16 is a critical factor that influences the severity and progression of AIDS and HAART failure, as well as the reduction in survival rate and increase in the risk of HIV transmission in HIV patients. 17
In this vein, it has recently been hypothesized that oral infections, including chronic periodontitis, could be involved in the pathway of HIV reactivation. Cross-sectional studies correlate the presence of well-established Gram-negative periodontal pathogens and inflammatory markers of periodontal destruction (metalloproteinases, interferon-γ, and prostaglandin-2) with higher virus load. 18 At the same time, some oral pathogens and inflammatory mediators could elicit and trigger HIV reactivation in monocytes/macrophages, dendritic cells, and T cells. 17,19 This knowledge permits the hypothesis that periodontal disease could be associated with the most severe HIV conditions, such as higher viral load and CD4 T lymphocyte reduction. However, this association has not yet been well studied. Based on this, the present study assessed whether medical conditions (i.e., viral load and CD4 T counts) in HIV-associated chronic periodontitis subjects could be improved after antiinfective periodontal treatment.
Materials and Methods
Study design
This study was designed as a controlled study to correlate the clinical outcomes of periodontitis treatment of HIV patients and the CD4 T lymphocyte levels and HIV viral load. The study was approved by the Ethics Committee of Paulista University (221/10).
Population screening
Potential patients were selected from those referred to the Center for Study and Care of Special Patients (CEAPE), Paulista University, SP, Brazil. The study inclusion criteria were (1) diagnosis of periodontitis 4 ; (2) HIV-positive status (ELISA/Western blot); (3) at least eight sites presenting a probing pocket depth (PPD) ≥4 mm with bleeding on probing, associated with a radiographic bone loss; and (4) those who had experienced HAART for more than 3 years with no change of dose or medication protocols. Patients who (1) were pregnant or lactating; (2) were suffering from any other systemic diseases (cardiovascular, diabetes, and others); (3) had received antimicrobials or opportunistic infection prophylaxis in the previous 6 months; (4) were taking long-term antiinflammatory drugs; (5) had received a course of periodontal treatment within the past 6 months; and (6) were not able to provide consent to participate in the study or did not accept the proposed treatment plan were excluded from the study.
Medical parameters
All patients selected were evaluated with regard to their gender, age, skin color, exposure category, smoking behavior, CD4 T lymphocyte cell counts, and HIV viral load at baseline and at 3 and 6 months after therapy.
Clinical parameters
All clinical parameters were assessed before periodontal therapy (baseline) and at 3 and 6 months afterward by a single calibrated examiner (intraclass correlation=94%) using a manual probe (PCP15-Hu-friedy, Chicago, IL).
The following clinical parameters were evaluated: probing pocket depth (PPD), a measurement of the distance from the bottom of a pocket to the gingival margin, and clinical attachment level (CAL), the distance from the bottom of the pocket to the enamel-cement junction.
Pre-treatment
All of the subjects attended motivational sessions and received oral hygiene instructions to ensure that they could maintain a proper level of oral hygiene before starting other treatment. During these sessions, a case presentation was given to subjects related to the specific features of HIV infection and periodontal disease.
Non-surgical periodontal treatment
The periodontally involved teeth of all participants were treated using an ultrasonic scaler (Cavitron, Dentsply, York, PA) with subgingival tips (FSI-SLI, Dentsply).
The first treatment occurred in January 2011 and examinations ended in August 2012. Recall visits occurred weekly during the first month and monthly until the sixth month. During these appointments, a supragingival prophylaxis session was performed and oral hygiene instructions were reinforced.
Data management and statistical analysis
The statistical analysis involved this Per Protocol population (subjects who completed the follow-up). The null hypothesis tested was that HIV-associated periodontitis treatment did not promote additional benefits to the CD4 T lymphocyte level and HIV viral load. To test this hypothesis, SAS 9.02 and Bioestat 5.0 programs were used.
The experimental unit of the present study was the patient. For clinical parameters, repeated-measures of analysis of variance (ANOVA) were used to detect intragroup differences in clinical parameters (PPD, CAL). When a statistical difference was found, the difference was determined using the Tukey method. To address the relationship between periodontal clinical change and systemic HIV-markers, Pearson's correlation test was used. An experimental level of significance was determined to be 5%.
Results
Demographic characteristics at baseline
The mean age of the 15 study participants at baseline was 45.7±5.2; 66.6% of them were male and 73.3% declared that they were white. In total, 73.3% of subjects declared themselves to be homosexual and 33.3% were smokers.
Clinical and systemic markers
Table 1 demonstrates that the reduction in PPD and gain in CAL, as well as plaque index, were statistically significant at months 3 and 6 after periodontal therapy (p<0.05). By the sixth month, Cal gain was 0.6±0.5 mm and PPD reduction was 0.7±0.5 mm.
Paired Student's t test (p<0.05).
PPD, probing pocket depth; CAL, clinical attachment level.
Moreover, the CD4 lymphocyte count also presented the same trend. A statistically significant increase in CD4 counts could be seen at 3 months (p<0.05) and at 6 months (p<0.05). Regarding viral load, an inverse trend was noted. HIV counts numerically decreased at 3 and 6 months; none of the subjects presented detectable levels of HIV at 6 months. This reduction achieved a borderline p-value of 0.17 at 6 months. In Fig. 1, it is possible to see that all subjects presented a similar trend in reduced PPD values and increased CD4 count throughout the study period, reinforcing the impact of periodontal condition improvement in systemic health.
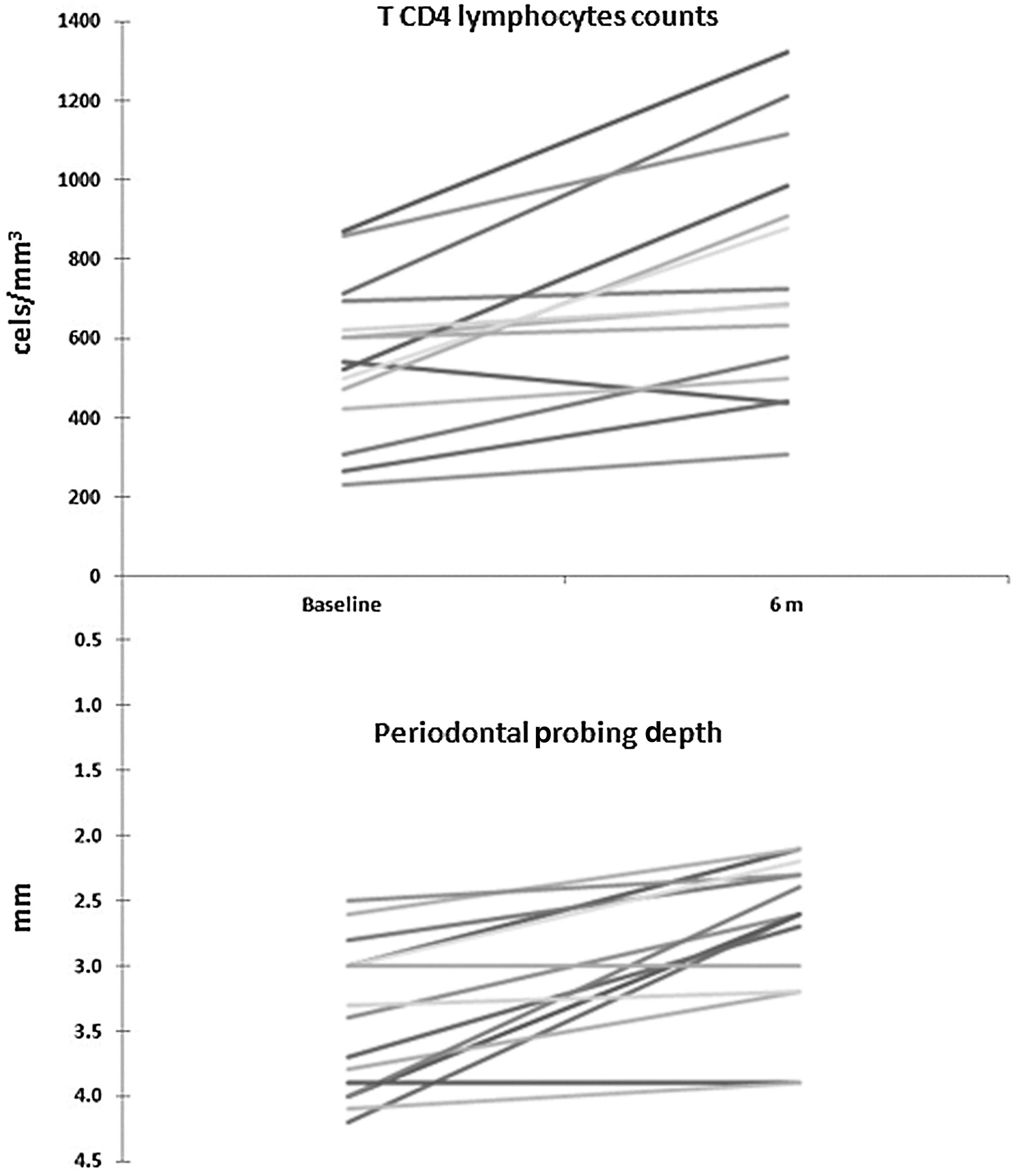
Individual values of CD4 T cell counts (cells/mm3) and periodontal probing depth (mm) at baseline and 6 months.
Figure 2 highlights the relationship between the improvement in clinical parameters, i.e., PPD reduction, and the number of CD4 T lymphocytes. With a greater PPD reduction, a larger increase in TCD4 cells occurs (r=0.68, p=0.02).
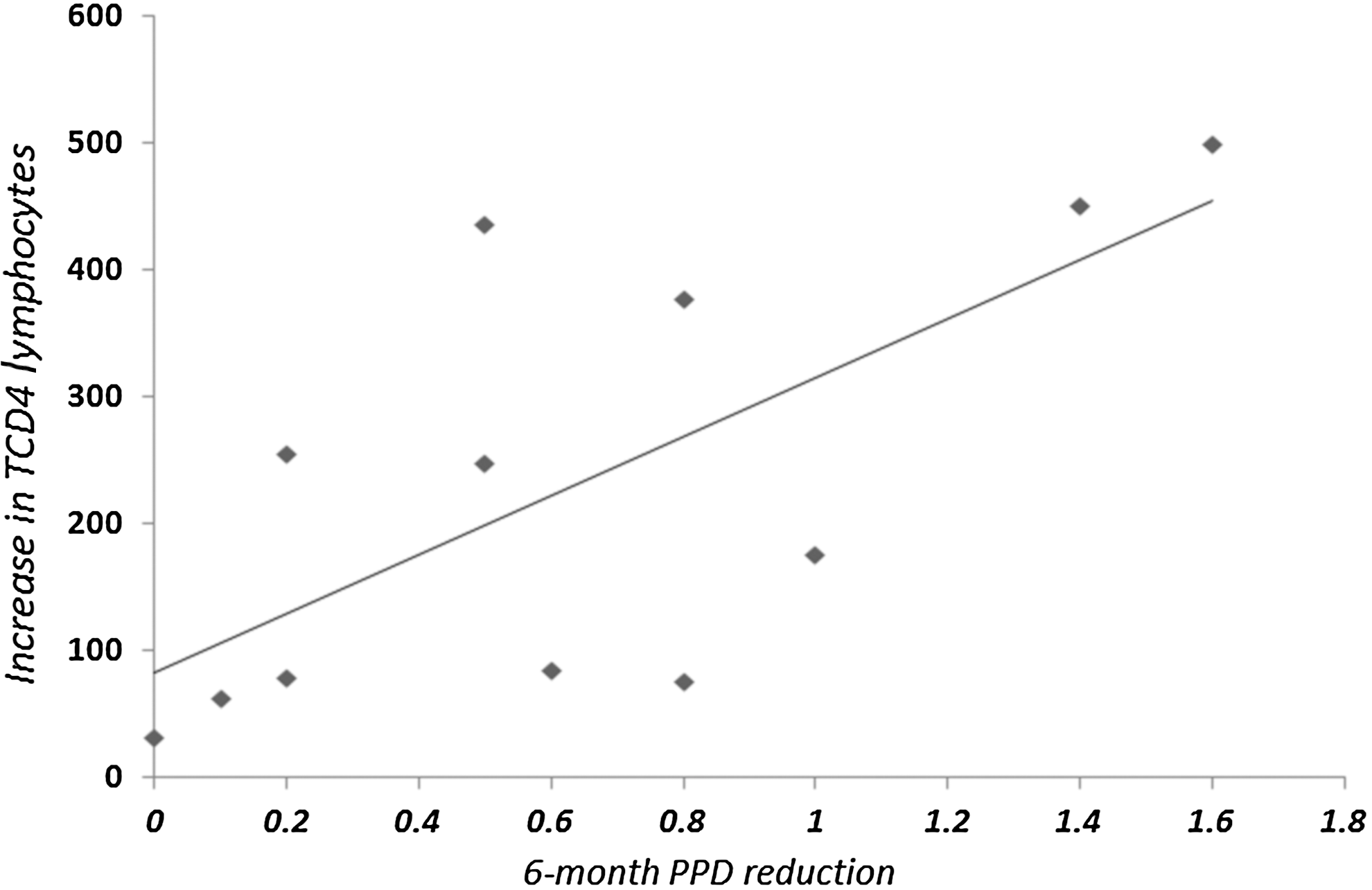
Correlation between probing pocket depth (PPD) reduction and increase of CD4 T lymphocytes at 6 months.
Discussion
During the past decade, the potential association between periodontal disease and systemic disorders has generated substantial interest. Recent studies support the theory that the chronic infectious response occurring in periodontal disease may have a role as a risk modifier of systemic diseases, including atherosclerosis, bacterial endocarditis, cardiovascular disease, diabetes mellitus, and respiratory disorders. 9 –13 The association with systemic diseases is related to the changes during the process of periodontal destruction. An altered release of inflammatory markers (metalloproteinases, interferon-γ, and prostaglandin-2) 18 and the presence of Gram-negative periodontal pathogens 19 may directly (by invasion of tissues and blood migration) or indirectly (by a systemic increase of inflammatory mediators) elicit systemic antibody responses, creating transient bacteremias, loading in distant tissues, and inducing pathological changes. 11,19
Based on this knowledge, some other clinical trials have tested whether antiinfective periodontal treatment could reduce the occurrence of adverse systemic effects. Periodontal treatment during pregnancy may reduce the preterm birth and low birth weight incidence, 20 reversing the disease process. In the same way, oral microbiota control was related to a reduction of the occurrence of nosocomial pneumonia and pulmonary diseases, 9 as well as noting that periodontal therapy could promote an improvement in glycemic control in type-2 diabetes mellitus subjects presenting with periodontal destruction. 12 With this in mind, the present data evaluated whether HIV-associated periodontitis treatment could improve the systemic HIV-related markers (CD4 T lymphocytes count and HIV load), as the presence of periodontal infection has recently been related to negative events related to HIV conditions. It was observed that there was a statistically significant increase in CD4 T counts and a total reduction in viral load, which is undetectable in all patients (the range of detectable virus differs somewhat for each test; the lowest level of detection generally is 40–75 copies/ml, but does not indicate the absence or clearance of virus in the body). Moreover, a direct correlation between CD4 T counts and PPD reduction could be detected, showing a clear improvement in this systemic marker of HIV condition with periodontal infection resolution.
During coinfections (in our focus, HIV-associated periodontitis), the activation of HIV-1-infected cells by different membrane receptors [toll-like receptors (TLRs) and cytokine receptors, costimulatory molecules, etc.] induces activation of the HIV-1 long terminal repeat (HIV-1 LTR) provirus with the consequent production of new virions. Activation of cell membrane receptors in HIV-1-infected cells turns on downstream signaling pathways, which leads to the activation of transcription factors with the ability to regulate not only pro-inflammatory genes but also HIV-1 LTR transcription and the production of new virions. TLR activation leads to the production of cytokines as well as the production of new HIV-1 virions. Pro-inflammatory cytokines produced by the HIV-infected cell itself in response to bacterial challenge, as well as cytokines from other cellular sources (e.g., T helper cells, natural killer cells, dendritic cells, epithelial cells, and fibroblasts) that are present in periodontal disease pathogenesis, might have the capacity to induce synergistic HIV viral production and reactivation. 17
Moreover, chronic oral infections, such as the periodontal disease investigated in the present study, may provide a risk to the maintenance of treatment success in HIV patients. The presence of chronic oral infections that undermines the integrity of oral epithelial barriers can trigger a response in local T cells, macrophages, and dendritic cells in gingival tissues. 17,19 Consequently, these chronic infections that are present in HIV-associated severe chronic periodontitis subjects being treated with HAART could contribute to HAART failure and the progression of acquired immunodeficiency syndrome. 17,19
Additionally, clinical evidence reveals a positive correlation between HIV viral load and oral infectious diseases, such as periodontal disease, hairy leukoplakia, and candidiasis. 18,21,22 However, the potential for oral pathogens to impact HIV cell reservoirs and induce HIV reactivation has not yet been delineated. 17 Evidence has suggested that the development and progression of several clinical syndromes in HIV infection are related to the degree of immunosuppression. 23 CD4 T counts and HIV viral load have been used as markers of immunosuppression and disease progression in HIV patients. Finally, based on these considerations, we present periodontal disease as an example of oral chronic infections that could have the ability to induce HIV exacerbation in HIV patients. Furthermore, the resolution of the inflammatory process could represent a tool to stop the depreciation of systemic health by periodontal disease. As seen, the present study confirms this plausibility once the periodontal treatment could be associated with an increase in CD4 T lymphocyte counts, which is a reliable marker of improvement in the general health of HIV subjects. In spite of positive results, some important considerations should be made regarding our study.
First, we had an ethical dilemma in including a control group, i.e., non-periodontal treatment or HIV patients without HAART, which normally characterizes a randomized clinical trial. However, the results in our population could represent the first step to future studies in order to confirm the role of periodontal health in systemic conditions of HIV individuals. Moreover, although all of the subjects included in our study were under HAART medication for more than 3 years, some of them did not achieve an appropriate HIV load or, especially, CD4 T cell counts. To not bias our results, we included only subjects receiving the same HAART protocol for at least 3 years, excluding any impact that this medication may have on our results. In summary, evidence showed that the reduction of inflammatory mediators and pathogenic microbiota associated with periodontal disease may lead to an improvement in the general health of patients. However, further investigation is required to confirm this, which would involve enrolling a larger population, and HIV patients with lower CD4 T cell counts (immunosuppression), in order to determine whether this treatment induces a significant improvement in general health and an improvement in the quality of life and survival of HIV patients. Therefore, in spite of the limitations of this study, it can be suggested that HIV-associated periodontitis treatment could be associated with an improvement in medical conditions in HIV subjects.
Footnotes
Acknowledgments
This study was supported by Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES-PROSUP).
Author Disclosure Statement
No competing financial interests exist.