
Abstract
We estimated the impact of loss to follow-up (LTFU) on the mortality rate among HIV-1-infected patients in Curaçao. A total of 214 therapy-naive HIV-1-infected patients aged 15 years or older upon entering into HIV care between January 2005 and July 2009 were included. Persons who discontinued follow-up for more than 365 days were defined as LTFU and traced with the aim of registering their vital status. If no personal contact could be made, data were matched with the Curaçao National Death Registry. Mortality rates were estimated before and after starting combination antiretroviral therapy (cART). We used log-rank tests to compare survival rates among patients LTFU and patients who experienced continuous follow-up. Pre-cART mortality in patients LTFU was similar to pre-cART mortality in those with continuous follow-up (p=0.79). All pre-cART deaths occurred within 6 months after entry. Low CD4 cell count was predictive of a shorter time to death after entry. Adjusting for those who were LTFU, the mortality rate after starting cART increased from 4.3 to 5.5 per 100 person years of observation (p=0.06). Mortality after starting cART was highest in the first 2 months after starting cART, especially for those who had late disease stage. Mortality rates were lower in patients with continuous follow-up compared to LTFUs (p<0.001). Mortality rates in HIV-1-infected patients who have started cART in Curaçao are underestimated as a result of inefficient patient administration combined with people starting cART at a very late disease stage. Monitoring HIV treatment could help in reducing the risk of LTFU and may improve the effect of treatment.
Introduction
L
The Caribbean region has the second highest prevalence of HIV-1 infection in the world. 4 The proportion of LTFUs in HIV-1-infected patients treated with cART varies substantially throughout the region. 5 –12 There is a lack of published data on rates of LTFU for HIV-1-infected patients receiving pre-cART care and on the vital status of HIV-1-infected patients defined as LTFU. Consequently, the survival outcomes of Caribbean cohorts are often estimated using the results of African studies. 7,13
Previously, we have shown that 10% of patients who started cART became LTFU 5 and that the incidence of intermittent care before starting cART was 25.4 per 100 person years of observation (PYO), while it was 6.1 per 100 PYO after they started cART. 14 In this article, we describe the impact of LTFU and patient tracing on mortality rates of HIV-1-infected patients from Curaçao before and after the start of cART.
Materials and Methods
Setting and study population
Curaçao has a population of 140,000 and an estimated HIV prevalence of 0.62% to 1.05% among adults. 15 The St. Elisabeth Hospital in Willemstad is the sole provider of HIV-related care. cART has been available since 1996 and is distributed by the hospital pharmacy. Centralized registration and monitoring of HIV-infected individuals treated in Curaçao began in January 2005, in collaboration with the Dutch HIV Monitoring Foundation [Stichting HIV Monitoring (SHM)]. 16
We included all HIV-1-infected patients older than 15 years who were therapy-naive and received HIV-related care in Curaçao for the first time between January 2005 and July 2009. We defined HIV-related care as any outpatient visit to a physician treating HIV, an inpatient admission to the St. Elisabeth hospital, a measurement of CD4 cell count, or an HIV RNA viral load determination. We defined patients who had received HIV-related care at least once before July 2009, who were not known to be dead prior to July 2010, and who had no HIV-related care contacts between July 2009 and July 2010 as LTFU. We used contact information collected at clinical enrollment to trace patients, who were LTFU, to determine whether they were still alive or are known to have died. If we could not contact the patient or a contact person, we reviewed the national death registry for the patient's details. We defined patients we could not confirm to be alive or dead as “true-LTFU.”
We defined cART as at least two nucleoside reverse transcriptase inhibitors combined with at least one protease inhibitor and/or nonnucleoside reverse transcriptase inhibitor or at least three nucleoside reverse transcriptase inhibitors including abacavir or tenofovir. We defined pre-cART care as any HIV-related care before starting cART. Patients who started cART on the same date as their first HIV-related care did not receive any pre-cART care. We defined on-cART care as any HIV-related care after a patient started cART, regardless of whether he or she was actually taking antiretroviral medication.
Statistical analysis
We expressed mortality rates as the number of deaths per 100 PYO. We obtained confidence intervals and tested whether differences between groups were statistically significant using the chi-squared distribution. For pre-cART care, we defined PYO as the time in years between the first contact with HIV-related care and the patient starting cART or dying or the last contact with the patient before July 2010 if the patient did not die or start cART. For on-cART care, we defined PYO as the time in years between the patient starting cART and the patient dying or the last contact with the patient before July 2010 if the patient did not die.
We performed sensitivity analyses to determine how patients, who were untraceable, influenced the mortality rates. In the best case scenario, we assumed that all untraceable patients were still alive on 1 July 2010. In the worst case scenario, we assumed that all untraceable patients died the day after their last visit. We used Kaplan–Meier curves and log-rank tests to assess differences in mortality between the groups of patients who were traced to be alive or dead on July 1, 2010 and those who were LTFU but were found to be dead or alive. We analyzed differences between patients with known vital status and untraceable patients using Fisher's exact tests for categorical variables, Mann–Whitney U tests for continuous variables, and Poisson tests for rates.
For patients with known vital status, we examined univariate relationships between the time from entry into care to death and gender, place of birth, age at entry into care, AIDS at entry into care, and CD4 cell count at entry into care and the start of cART using Cox regression models. In our calculation of PYO and Cox regression models, we followed patients until they died. If we did not observe that a patient had died, we generally censored them on the date of their last visit to the clinic before database closure. However, we censored patients LTFU and traced to be alive on the date on which contact was made.
Results
Between January 2005 and July 2009, a total of 214 patients aged over 15 years received HIV-related care for the first time in Curaçao. Of these, 135 (63%) were male, 156 (75%) had become infected with HIV due to heterosexual contact, and 150 (71%) were born in Curaçao. At the time of their first contact with HIV-related care, 14 (7%) had a current AIDS-defining condition, 12 (22% of women aged 15 to 45 years) were pregnant, and 50 (37%) had a CD4 cell count less than 200 and a median CD4 count of 302 cells/mm3 [interquartile range (IQR), 106 to 472]. As of July 2010, 60 (28%) patients had received only pre-cART care, 44 (21%) only on-cART care, and 110 (51%) both pre-cART and on-cART care. Hence, we report on 170 patients who received pre-cART care and 154 patients who received on-cART care.
Pre-cART care
As of July 2010, 29 (17%) of the 170 patients who had received pre-cART care were still receiving pre-cART care, 110 (65%) had started cART, eight (5%) had died without starting cART, and 23 (14%) were LTFU before starting cART. The median time between the start of HIV-related care and the last incidence of HIV-related care for those who were LTFU was 50 days (IQR 0–122). Of the 23 patients who were LTFU before starting cART, we traced 17 (74%) to be alive and one (4%) to have died. Five (22%) patients were untraceable (true-LTFU), of whom three were reported to have emigrated from Curaçao. We present the characteristics of the patients in Table 1. Of patients who were true-LTFU before starting cART 80% were born outside Curaçao and 60% female and tended to be younger with a median age of 35 years (IQR, 31–45).
Percentage of women of childbearing age (15–45 years).
LTFU, lost to follow-up; True-LTFU, true lost to follow-up; cART,combination antiretroviral therapy; IQR, interquartile range; AIDS, acquired immunodeficiency syndrome.
Prior to tracing, we knew that 139 patients were alive and eight were dead following 121 PYO before starting cART. We traced 17 patients, who were LTFU, to be alive and one to be dead following 48 years of PYO. This results in a mortality rate of 6.6 (95% confidence interval 2.9 to 13.0) deaths per 100 PYO among patients with known vital status and 5.6 (95% CI 0.1 to 31.0) deaths per 100 PYO among patients LTFU (rate ratio=3.2, p-value=0.45). The proportion of patients alive 1 year after entry into care with known vital status was 0.93 (95% CI 0.87 to 0.97) and who were traced was 0.94 (95% CI 0.67 to 0.99) (log-rank p=0.79). We present the results of the Cox regression analyses between the time to death and gender, place of birth, age, CD4 cell count at entry into care, and AIDS at entry into care in Table 2. The only significant variable to have an association with the time to death was CD4 cell count at entry into care.
LTFU, lost to follow-up; True-LTFU, true lost to follow-up; cART, combination antiretroviral therapy; HR, hazard ratio; MSM, men having sex with men; AIDS, acquired immunodeficiency syndrome; CI, confidence interval.
After tracing, the vital status for 165 persons was known and a total of nine persons were known to have died during 173 PYO, resulting in an updated mortality rate of 5.2 (95% CI 2.37 to 9.87) per 100 PYO. In the best case scenario of the sensitivity analysis, nine patients died following 187 PYO, resulting in an overall mortality rate of 4.8 (95% CI 2.2 to 9.1) per 100 PYO. In the worst case scenario, 14 patients died following 175 PYO, resulting in an overall mortality rate of 8.0 (95% CI 4.4 to 13.4) per 100 PYO.
On-cART care
A total of 154 patients started cART. Of these, 98 (64%) were male; their median age at the start of cART was 43 years (IQR, 35–52) and their median CD4 count was 158 (IQR, 63–244) cells/ml. As of July 2010, 117 (77%) were still receiving on-cART care, six (4%) had transferred to one of the treatment centers in the Netherlands and were alive, 14 (9%) had died, and 17 (11%) were LTFU. The median time between the start of cART and the last incidence of HIV-related care for those who were LTFU was 132 days (IQR 0–272 days). Of the 17 patients, who were LTFU, we traced seven (41%) to be alive and four (24%) to have died. Six (35%) patients were untraceable (true-LTFU), of whom two were reported to have emigrated from Curaçao. We present the characteristics of the patients in Table 3.
Percentage of women of childbearing age (15–45 years).
LTFU, lost to follow-up; True-LTFU, true lost to follow-up; cART, combination antiretroviral therapy; IQR, interquartile range; AIDS, acquired immunodeficiency syndrome.
Prior to tracing, we knew that 123 patients were alive and 14 were dead following 307 years of PYO. We traced seven patients to be alive and four to be dead following 22 years of PYO. This resulted in a mortality rate of 4.6 (95% CI 2.5 to 7.7) deaths per 100 PYO among patients with known vital status and 18.2 (95% CI 5.0 to 46.6) deaths per 100 PYO among patients LTFU (rate ratio=0.25, p-value=0.06). Kaplan–Meier curves for survival during the first year after the start of cART are given in Fig. 1. The proportion of patients alive 1 year after the start of cART with known vital status was 0.94 (95% CI 0.88 to 0.97) and who were traced was 0.60 (95% CI 0.25 to 0.83) (log-rank p<0.01). We present the results of the Cox regression analyses between the time to death and gender, place of birth, age, CD4 cell count at entry into care, and AIDS at entry into care in Table 2. The only significant variable with a relationship to the time to death was AIDS at entry into care.
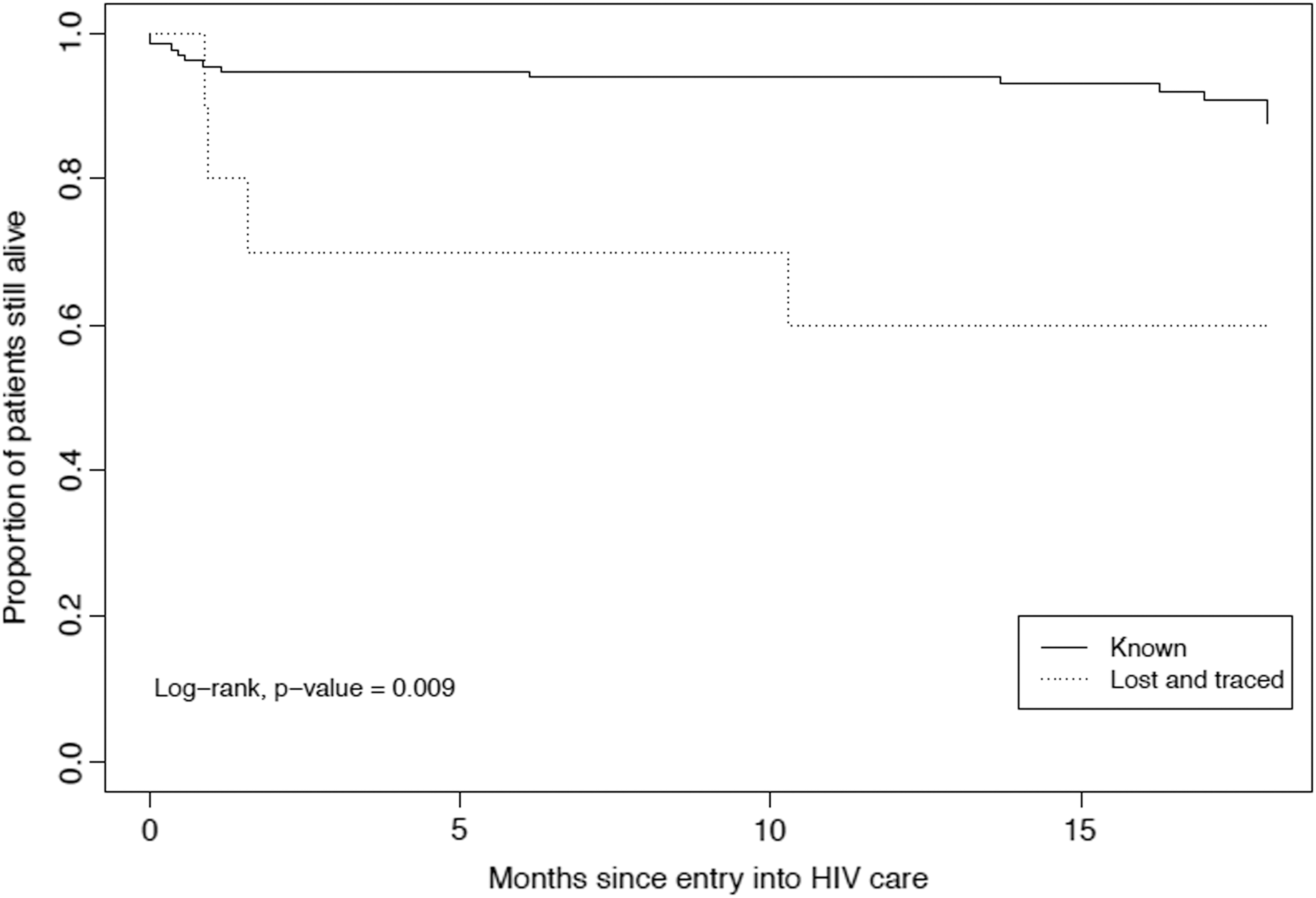
Proportion of patients alive before (continuous line) and after tracing (dotted line) of the patients who have started combined antiretroviral therapy (cART) over time.
After tracing, the vital status for 144 persons was known and a total of 18 persons were known to have died during 329 PYO, resulting in a corrected mortality rate of 5.5 (95% CI 3.2 to 8.6) per 100 PYO. In the best case scenario of the sensitivity analysis, 18 patients died following 343 PYO, resulting in an overall mortality rate of 5.2 (95% CI 3.1 to 8.3) per 100 PYO. In the worst case scenario, 24 patients died following 331 PYO resulting in an overall mortality rate of 7.3 (95% CI 4.6 to 10.8) per 100 PYO.
Discussion
We have shown that a substantial proportion of HIV-1-infected patients in Curaçao become LTFU before and after starting cART. This study provides a description of LTFU and death before and after starting cART. In the on-cART patient group, patients who were LTFU were more likely to have died than patients who remained in active follow-up. However, patients who received pre-cART care and who were LTFU had mortality rates similar to those who remained in active follow-up.
A possible explanation for this is that patients who interrupt care before starting cART have less advanced disease stage and objectify fewer clinical symptoms than those who continue care as is shown by others. 14,17 Only limited data from sub-Saharan Africa on patient tracing before the start of cART have been published previously. 18 In addition, engagement in care before starting cART is crucial in planning a timely start of cART. 19,20
We also report that the mortality rate among patients who have already started cART is significantly higher for patients who have become LTFU than for those who receive regular HIV-related care. The rates of LTFU after starting cART and mortality in patients LTFU in our study were lower than reported in African settings. 21 –23 In a study carried out in France on pooled data on patients receiving pre-cART and on-cART care, the rate of LTFU was lower than in our study and the proportion of patients traced to have died was similar. 24
Possible limitations of our study were the small sample size, which may have limited the statistical power and made more sophisticated methods of analysis 25 –27 inappropriate, and the fact that some patients were untraceable, possibly leading to an underestimation 28 of mortality. However, we estimated the mortality rate in the best and worst case scenarios, providing a range for the true mortality rate, and described the entire HIV-1-positive population of one country from the moment of prospective data collection, hence minimizing selection bias.
In conclusion, we found that the mortality rate in HIV-1-infected patients who became LTFU after starting cART was higher than those who remained in care after starting cART. In Curaçao, we would underestimate mortality rates in HIV-1-infected patients who have started cART if we assume that those who are LTFU have the same mortality rate as those in active care. This may result from inefficient administration and late clinical presentation. Monitoring HIV treatment may help reduce the risk of LTFU and, hence at the population level, improve the effect of treatment. More studies to trace patients who have become LTFU in Caribbean settings are needed to establish actual local rates of mortality and the real outcomes of cART programs in this region.
Footnotes
Acknowledgments
The authors would like to thank Y.M. Ruys, K. Laurant, and H. Daal for support with data collection.
This study was supported by a grant from The Netherlands Antilles Foundation for Higher Education (NASKHO).
Author Disclosure Statement
No competing financial interests exist.