
Abstract
The reduction of risk of non-AIDS events after combined antiretroviral therapy (cART) initiation and the crude incidence rate (CIR) of these events in patients who control the viral load without cART (controllers) in a cohort of 574 antiretroviral-naive patients with a baseline CD4 T cell count above 500 cells/mm3 were assessed. Non-AIDS severe events were defined as a first admission to the hospital due to non-AIDS-defining malignancies, cardiovascular, neuropsychiatric, liver-related, or end-stage renal disease events. Potential determinants of non-AIDS/death events were studied using Cox regression models. Eighty-five non-AIDS/death events occurred during 6,062 persons-years of follow-up (PYFU) with a CIR of 1.4 per 100 PYFU. Factors associated with non-AIDS/death event were age (HR 3.4; 95% CI: 1.6–6.9), nadir CD4 below 350 cells/mm3 (HR 2.5; 95% CI: 1.4–4.6), and a last determination of viral load above the median (HR 1.9; 95% CI: 1.0–3.3). The CIR of non-AIDS/death events was 2.1 and 1.8 per 100 PYFU before and after cART in patients who started cART (n=446). A reduction of CIR of non-AIDS events after cART initiation was observed only in patients with a nadir of CD4 above 350 cells/mm3 (2.5 vs. 0.6 per 100 PYFU, p=0.004, and remained stable after cART in patients with a median nadir of CD4 below 350 cells/mm3. CIR was similar in elite, viremic, and noncontrollers (1.1, 1.0, and 1.5 per 100 PYFU, respectively, p=0.25). Reduction of CIR of non-AIDS events after cART initiation depends on nadir CD4 T cell count. Most of the controllers patients had a CIR similar to noncontrollers. These data support the early initiation of cART in HIV-infected patients.
Introduction
I
In fact, it has been reported in the SMART study 22 that patients who discontinued cART had a higher risk of non-AIDS events and death than patients who continued with medication. It is also known that patients who started cART with a high level of CD4 T cell count had a lower risk of death than patients who delay the initiation of medication. 23,24 However, it is not known whether the reduction of the risk of the appearance of new non-AIDS events with ART depends on the level of immunosuppression reached. In addition, although these studies 23,24 suggest that cART should be started early, clinical data supporting therapy for nonprogressors and elite controllers are lacking. 25 To address these questions, we studied a cohort of 574 antiretroviral-naive patients with a CD4 T cell count above 500 cells/mm3 followed-up for a median of 10 years.
Materials and Methods
Patients
A cohort of 675 HIV patients with a baseline CD4 T cell count above 500 cells/mm3 from a University Hospital in Barcelona was followed-up from January 1996 to December 2011. Inclusion criteria were patients followed-up longer than 1 year with all CD4 T cell count determinations above 500 cells/mm3 in the first year of follow-up. All reasons patients were admitted to the hospital were registered in a database and confirmed in patient clinical files. We selected admission to the hospital as the criterion of severity. Non-AIDS severe clinical events were defined as a first admission to the hospital due to non-AIDS-defining malignancies, cardiovascular, neuropsychiatric, liver-related, or end-stage renal disease events. All admissions for other reasons were recorded but excluded from the analysis. An AIDS severe clinical event was defined as any AIDS-associated event registered in the patient file. Deaths were collected from the National Death Register. The following data were collected: age, gender, risk factor for acquisition of HIV infection, coinfection with hepatitis C or B virus, known duration of HIV infection, type of cART, and date of initiation of cART and death. CD4 and CD8 T cell count and viral load were collected at the following time points: baseline, nadir/peak (respectively), date of event, the last determination before cART initiation, and the last determination. The study was approved by the institutional ethical review board.
Statistical analysis
Severe non-AIDS and AIDS events occurring during the follow-up time were recorded as mentioned above and the incidence rates were calculated as the number of events per 100 person-years of follow-up (PYFU). Admissions to the hospital for recurrences of the same diagnosis were excluded. Potential determinants of clinical events were studied using Cox regression models. Dependent variables of the model were non-AIDS/death and AIDS/death events. A univariate analysis was performed and selected those significant variables to be included in a multivariate analysis using a stepwise forward (Wald) method. Those patients with more than one non-AIDS event were censored at their first event for the multivariate analysis. A subanalysis considering the events in addition to the patients was performed to determine what risk factors were found in those patients with two events or more. In those patients who started cART (n=446), a subanalysis comparing the incidence rate in the periods before and after cART initiation both adjusting or not for nadir CD4 T cell count was performed. In this subgroup of patients who had cART, factors associated with non-AIDS events during the period off and on cART were also analyzed separately using Cox regression models. Elite controllers, viremic controllers, and noncontrollers were defined as patients with a baseline viral load below the detectable level, from the undetectable level to 2,000 copies/ml, and above 2,000 copies/ml maintained for at least the first year of follow-up without cART, respectively. These patients had to have at least three determinations to be considered controllers.
Results
Clinical characteristics of patients
Six hundred and seventy-five patients with a baseline CD4 T cell count above 500 cells/mm3 have had a first appointment in the daycare center of our university hospital since 1996; 101 were excluded for the analysis, 40 due to lack of baseline data, and 61 were lost before 1 year of follow-up. Therefore, 574 patients were analyzed with a median (range) follow-up of 10 years (1–15) and contributed 6,062 PYFU to the non-AIDS/death and AIDS/death events analysis. Characteristics of the patients are shown in Table 1. Most of the patients were men (80%) who have sex with men (MSM, 57%) and were a median age of 43 years old. Twenty-eight percent were coinfected by hepatitis C and 5% with hepatitis B. Seventy-eight percent started cART during follow-up (63% with a protease inhibitor-sparing regimen). The median baseline CD4 T cell count was 630 cells/mm3 and the median viral load was 4 log10 copies/ml.
Median (IQR).
n (%).
cART, combined antiretroviral therapy; PI, protease inhibitors.
Non-AIDS, AIDS events, and death in the cohort
One hundred and eight-two patients out of 574 (32%) were admitted to the hospital 541 times (a median of three admissions per patient) with 288 diagnoses not related to AIDS and 48 related to AIDS. The most frequent reasons to be admitted were chirurgical interventions or traumatic problems (35%), followed by infections (including sexually transmitted diseases) (27%), non-AIDS-defining malignancies (11.5%), and cardiovascular events (7%).
Table 2 shows the diagnoses at admission to the hospital due to non-AIDS or AIDS events. Eighty-five non-AIDS events occurred during 6,062 persons-years of follow-up in 57 patients with a crude incidence rate (CIR) of 1.4 per 100 PYFU [95% confidence interval (CI) 1.1–1.7]. The most common were non-AIDS-defining malignancies (39%), cardiovascular (23%) events, and neuropsychiatric events (20%). Forty-eight AIDS events occurred during follow-up in 47 patients; the CIR was 0.8 per 100 PYFU [95% confidence interval (CI) 0.6–1.1]. The most common AIDS event was pulmonary tuberculosis (32%).
Factors associated with non-AIDS/death events and AIDS/death events in the univariate and multivariate analysis are shown in Table 3. CD8 T cell count at baseline, date of event, the last determination before cART initiation, and the last determination were also assessed and were not associated with non-AIDS/death events and AIDS/death events in the univariate and multivariate analysis (data not shown). Factors independently associated with the occurrence of a first non-AIDS/death event were age at baseline (HR 3.4; 95% CI: 1.6–6.9, p=0.001), a nadir CD4 below 350 cells/mm3 (HR 2.5; 95% CI: 1.4–4.6, p=0.003), and a last determination of viral load above the median (HR 1.9; 95% CI: 1.01–3.3, p=0.02).
Patients were classified according to median value: reference categories were value above the median in all the variables related to CD4 T cell count and value below the median in age and variables related to viral load.
The reference category was women.
The reference category was nonhomosexual.
The reference category was protease inhibitor containing regimen.
In patients who started antiretroviral therapy, n=446, these variables were not introduced in the multivariate analysis. All significant variables in the univariate model have been introduced in the multivariate model, but only the p values of the significant variables have been shown.
cART, combined antiretroviral therapy; CD4, CD4 T cell count (cells/mm3); VL, viral load (copies/ml).
As some patients had more than one event, also analyzed were the results when considering the total events in addition to the patients. The same factors and baseline CD4 T cell count (HR 1.8; 95% CI: 1.2–2.9, p=0.008) were associated with the occurrence of any non-AIDS/death event. In addition, the result indicating that the median nadir CD4 T cell count was the value delineating the risk for non-AIDS events could also suggest that it was linked to patient management. It could be argued that the patients included early had a CD4 nadir below 350 due to the recommendations at that time and that these patients are also those with the longer infection and treatment duration and more toxic cART. By contrast, patients with a nadir over 350 are probably those treated recently, with a shorter duration of known infection and treatment, with friendlier cART. This was closely evaluated to avoid any confounding factors. First, we adjusted the multivariate model by known duration of HIV infection and the factors associated independently with non-AIDS event/death did not change (data not shown).
Second, the known duration of HIV infection was similar between those patients with a CD4 nadir below or above the median [median (IQR) years 11.5 (7–16) vs. 11 (6–15), respectively, p=0.28]. Third, the median (IQR) date of initiation of cART was similar between both groups [September 2004 (January 1998 to October 2008) vs. June 2002 (December 1997 to March 2009), for patients with a nadir CD4 below and above the median, respectively]. Fourth, the type of cART [as defined as a protease inhibitor (PI)-containing or -sparing regimen] was similar between both groups, p=0.46. Finally, the time on cART was also similar [median (IQR) years 5 (2–11) vs. 5.5 (2–11.2), for patients with a nadir CD4 below and above the median, respectively, p=0.8].
Factors independently associated with AIDS/death events were male gender, hepatitis C coinfection, a last determination of CD4 T cell count below the median, and a peak viral load above the median.
Non-AIDS/death events in patients who started cART
A subanalysis of the incidence rate in those patients who started cART in the periods before and after cART initiation was performed (n=446) (Fig. 1). The median (IQR) time of initiation of cART relative to baseline was 40 months (22–68). The CIR was 2.1 (95% CI 1.6–2.9) and 1.8 (95% CI 1.3–2.4) per 100 PYFU before and after cART, respectively (p=0.16). Thereafter, the patients were classified according to the median nadir of CD4 (350 cells/mm3). In those patients with a nadir below the median the CIR was 2.0 (95% CI 1.6–2.8) and 2.5 (95% CI 1.9–3.2) per 100 PYFU before and after cART, respectively (p=0.34); however, in patients with a nadir above the median the CIR was 2.5 (95% CI 1.9–3.2) and 0.6 (95% CI 0.3–1.0) per 100 PYFU before and after cART, respectively (p<0.0001). Factors independently associated with the occurrence of a first non-AIDS/death event in patients who started cART were the same for the whole cohort (data not shown). CD4 T cell count immediately before cART initiation or last determination of CD4 T cell count were not statistically different between those patients who have or did not have non-AIDS events. However, patients with a nadir CD4 T cell count below 350 cells/mm3 had a CD4 T cell count immediately before cART initiation and a last determination of CD4 significantly lower than patients with a nadir CD4 T cell count above 350 cells/mm3 [median (IQR) CD4 T cell count before cART 348 cells/mm3 (271–493) vs. 511 cells/mm3 (442–670), p<0.001, and a CD4 T cell count at the last determination of 510 cells/mm3 (387–722) vs. 753 cells/mm3 (583–988), p<0.001, respectively].
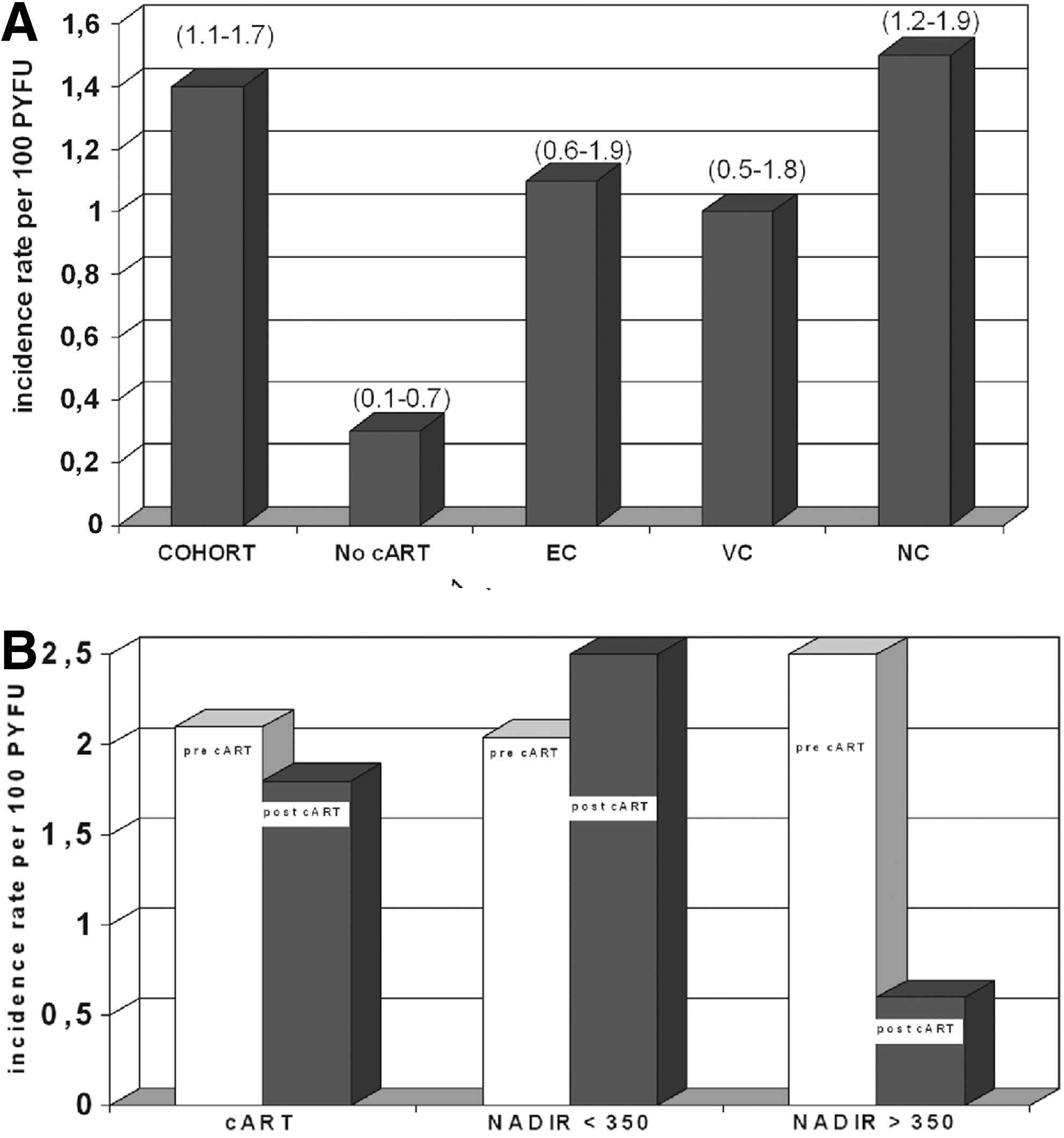
Crude incidence rate of non-AIDS events in the cohort.
Finally, the CIR of non-AIDS events was very low in all patients who did not have an indication to start cART, 0.3 (95% CI 0.1–0.7) per 100 PYFU.
Non-AIDS/death events in controllers
A subanalysis of the incidence rate in patients classified according to spontaneous control of viral replication during the first year of follow-up [elite controllers (n=64), viremic controllers (n=76), and noncontrollers (n=434)] was performed (Fig. 1). The CIR of non-AIDS events was 1.1 (95% CI 0.6–1.9), 1.0 (95% CI 0.5–1.8), and 1.5 (95% CI 1.2–1.9) per 100 PYFU, respectively (p=0.25). To study factors associated with non-AIDS/death events and influence of cART on CIR of non-AIDS events, elite and viremic controller groups were analyzed together. Factors independently associated with the occurrence of a first non-AIDS/death event in controllers were the same for the whole cohort (data not shown). In addition, the CIR of non-AIDS events was similar before and after cART initiation in controllers with a nadir CD4 T cell count below 350 cells/mm3, but dropped significantly in patients with a nadir CD4 T cell count above 350 cells/mm3 (no events were observed in these latter patients after cART initiation) (data not shown). The incidence of AIDS events was significantly lower in elite controllers and viremic controllers as compared with noncontrollers (data not shown) (p=0.03).
Thereafter, using a stricter definition, the patients were reclassified as elite controllers (n=25) or viremic controllers (n=22) only if they maintained a viral load below detectable levels or a viral load between detectable level and 2,000 copies/ml during the entire follow-up period. No patients reclassified as elite controllers with this criteria had a non-AIDS or AIDS event. The risk of non-AIDS events was significantly higher in those patients who did not control viremia during follow-up (n=39) than in those who controlled viremia below the detectable level (n=25) (HR 1.8; 95% CI: 1.4–2.2, p=0.01). Conversely, those patients reclassified as viremic controllers with the stricter definition maintained a similar CIR of non-AIDS events than those with only a low baseline viral load [1.0 (95% CI 0.1–3.2)].
Discussion
There are few studies describing non-AIDS events in cohorts of patients with a high level of CD4 T cell count. Some studies have shown an increased incidence of death 14 and non-AIDS events 2 in individuals with a CD4 T cell count above 350 cells/mm3 with uncontrolled viral replication. It is also known that patients who started cART with a high CD4 T cell count had a lower risk of death than patients who delay the initiation of medication. 23,24 However, factors predicting non-AIDS events in patients with a high CD4 T cell count have not been extensively analyzed. In addition, it is not known if the efficacy of cART in preventing the appearance of new non-AIDS events depends on the nadir of CD4 T cell count. It is also not known if the study of a cohort of antiretroviral-naive HIV-infected patients followed-up for a median of 10 years results in answers to some of these questions. We found that 78% of these patients started cART during the follow-up. The CIR of non-AIDS and AIDS events of these patients was similar to that previously reported. 2 As expected, factors independently associated with the occurrence of a first non-AIDS/death event were age at baseline, a nadir CD4 below 350 cells/mm3, and a last determination of viral load above the median. It could be argued that the time on cART, the known duration of HIV infection, or the change in the management of HIV infection with time and not the nadir CD4 could explain the difference. We have closely analyzed these parameters to exclude the bias. In addition, these same factors have already been described in more advanced patients 3,21,26 and support the initiation of cART even in patients with a high CD4 T cell count.
We found that factors independently associated with AIDS/death events were male gender, hepatitis C coinfection, a last determination of CD4 T cell count below the median, and a peak viral load above the median. In fact, some studies have demonstrated an association between hepatitis C infection and faster HIV disease progression. 27 In addition, the prognostic effect of viral load and CD4 T cell count on clinical progression to AIDS has been consistently reported, 28 even in patients with a high CD4 T cell count. 2
Regarding the CD4 T cell level at cART initiation and risk of non-AIDS events, Baker et al. 21 studied 1,397 patients who initiated ART and found that non-AIDS diseases were lowered by 14% for each 100 cells/mm3 higher latest CD4 T cell count. Therefore, starting cART with a high CD4 T cell count could prevent the appearance of new non-AIDS events. 23,24 It remains to be determined if, after starting cART, the CIR of non-AIDS events could decrease in those patients who delay cART initiation at a level found in patients who started medication with higher levels of CD4 T cells. We found that after cART initiation the CIR of non-AIDS events was about 4-fold higher in those patients who had a nadir CD4 T cell count below 350 cells/mm3 as compared with patients with a nadir above 350 cells/mm3. These data could suggest that there is a nonreturn point and that in the patients who delay cART initiation the CIR of non-AIDS events will be maintained at a higher level than in patients who do not delay cART initiation despite the normalization of circulating CD4 T cell numbers.
Lange et al. 29 reported that delaying the initiation of cART results in impaired functional immune restoration despite normalization of CD4 T cell count. It could be hypothesized that a functionally nonrecovered immune system can cause a higher risk of non-AIDS events in those patients who delay cART initiation. An alternative explanation is that although the CD4 T cell count immediately before cART initiation and the last determination of CD4 T cell count were not statistically different between those patients who have or did not have non-AIDS events, the quantitative and not only the qualitative immune recovery in patients who delay medication would be worse than in those patients who start cART with a higher CD4 T cell count. In fact, in our cohort, patients with a nadir CD4 T cell count below 350 cells/mm3 had a CD4 T cell count immediately before cART initiation and a last determination of CD4 significantly lower than patients with a nadir CD4 T cell count above 350 cells/mm3. These data suggest that the nadir CD4 T cell count is a good marker both of immunosuppression and of immune recovery after cART initiation.
All these data suggest that cART should start early, but it is not known how early it should be started. Clinical data supporting therapy for nonprogressors and elite controllers are lacking 25 and data on cohorts could help to answer this question. The increase in the rate of non-AIDS events in HIV-infected patients has been explained by the premature aging that appears to be due to constant and sustained immune activation. 30 It has been found that controllers also have abnormally high T cell activation levels, which may contribute to progressive CD4 T cell count loss even without measurable viremia 31,32 and may account for early atherosclerosis in these patients. 33 These findings could also explain why the risk of non-AIDS events in elite and viremic controller patients of our cohort was similar to that in noncontrollers. In addition, similar to noncontrollers, cART did not prevent the appearance of new non-AIDS events in controllers with a low nadir CD4 T cell count, suggesting that cART should also be initiated early in these patients. However, these data have to be taken with caution since the low number of events in these patients precludes a conclusion and further studies should confirm our data.
Our study has a number of drawbacks. First, the number of included patients and events are quite small, although we think that the study benefits from a long median follow-up. Second, one of the main limitations of our study was how the collection of non-AIDS events was chosen. The criteria selected those patients who were admitted to a hospital ward (not only emergency room) due to five prespecified non-AIDS events. Those patients under follow-up who developed an event without hospital admission or who were treated in the outpatient clinic were not included as events. We prefer to select these criteria to be certain that the event was severe enough to need a hospital admission. Therefore, it is possible that there could be a bias in our data and that the real number of events could be higher than those we collected. In any case, the CIR we observed was similar to that previously reported by other groups. 2,3,21,26 Third, cART initiation criteria could change according to guidelines or to physician and/or patient election and this could influence the results. Fourth, a number of factors possibly related to the occurrence of non-AIDS-related events and deaths are missing (i.e., comorbid factors such as smoking, hypertension, creatinine, and lipid levels) and have not been taken into account in the analysis. Finally, these results should be taken with caution since cohort studies have many limitations when trying to address whether earlier therapy is better and a randomized clinical trial is the only nonbiased way to assess it. The ongoing START clinical trial has been designed to respond to this question.
In summary, the analysis of a cohort of antiretroviral-naive HIV-infected patients with a baseline CD4 T cell count showed that age, a nadir CD4 below 350 cells/mm3, and a detectable viral load at last determination were factors independently associated with non-AIDS events. After cART initiation the CIR of non-AIDS events was 4-fold higher in those patients who had a nadir CD4 T cell count below 350 cells/mm3 as compared with patients with a nadir above 350 cells/mm3 suggesting that reduction of CIR of non-AIDS events after cART initiation depends on nadir CD4 T cell count. Finally, the CIR of non-AIDS events was similar in elite controllers, viremic controllers, and noncontrollers. Only those patients who retained a spontaneous control of viral replication during the entire follow-up period had a lower risk of non-AIDS events. These data suggest that early initiation of cART could also prevent the appearance of new non-AIDS events in controllers, although larger studies need to be performed to confirm our data.
Footnotes
Acknowledgments
This study was supported in part by the following grants: RIS: Red Temática Cooperativa de Grupos de Investigación en Sida del Fondo de Investigación Sanitaria (FIS): EC10-153, PI10/02984, TRA-094, FIS PS09/01297, and FIS 07/0291. Montserrat Plana is a researcher from the Institut d'Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS) and is supported by the ISCIII (Instituto de Salud Carlos III) and the Health Department of the Catalan Government (Generalitat de Catalunya).
Author Disclosure Statement
No competing financial interests exist.