
Abstract
The goals of this study conducted in Gabon were to determine the prevalence rate of HIV-1 group O (HIV-1/O) infections and to characterize the genetic diversity of HIV-1/O strains as well as implications on antiretroviral (ARV) drug resistance. During 2010–2011, 1,176 samples from HIV-positive subjects were tested at the CIRMF (Centre International de Recherches Médicales de Franceville) retrovirology laboratory using an in-house serotyping assay. Plasma HIV-1/O RNA viral loads (VL) were determined using the Abbott RealTime HIV-1 assay. After full genome sequencing, drug resistance patterns were analyzed using two different algorithms (Agence Nationale de Recherches sur le SIDA et les hépatites virales and Stanford). Overall, four subjects (0.34%) were diagnosed as HIV-1/O infected. One subject, untreated by ARVs, died 2 months after HIV-1/O diagnosis. One was lost to follow-up. Two additional patients, treated with nonnucleoside reverse transcriptase inhibitor (NNRTI)-based regimens, showed CD4 counts <200/mm3 and VL results of 101,000 and 10,050 cp/ml. After full-length genome sequencing of these two strains, we found a wide range of natural polymorphism in the protease (≥15 substitutions) and gp41 (N42D mutation) genes, as well as in the gag and gag-pol cleavage sites. No resistance mutation was detected in the integrase gene. These two strains harbored the Y181C mutation making them resistant to NNRTIs. M41L, M184V, and T215Y mutations were also found for one strain, making it resistant to all NRTIs by the Stanford algorithm. Even if HIV-1/O infection is low in Gabon, an accurate diagnosis and a reliable virological follow-up are required in Central Africa to optimize ARV treatments of HIV-1/O-infected patients.
Introduction
D
By contrast, little is known about HIV-1/O infections in neighboring countries such as Gabon. In a previous work published in 1997 by Peeters et al., two cases of HIV-1/O infections were diagnosed among 213 tested Gabonese HIV-positive sera, yielding a prevalence rate of 0.9%. 3 To date, the natural history of HIV-1/O infections as well as the intragroup genetic diversity of HIV-1/O strains circulating in Gabon are poorly documented. As recommended by the World Health Organization (WHO) in resource-limited countries, the scaling-up of first-line antiretroviral (ARV) regimens uses systematically nonnucleoside reverse transcriptase inhibitors (NNRTIs). The efficiency of this Public Health approach was recently described in Gabon. 4 Unfortunately, this strategy is not fully satisfactory in West-Central African countries since most of HIV-1/O isolates are naturally resistant to NNRTIs due to the presence of the Y181C mutation. 5,6
The main goals of the present study conducted in Gabon were to determine the prevalence rate of HIV-1/O infections in this country by using an in-house serotyping assay and to characterize the genetic diversity of HIV-1/O strains and implications on ARV drug resistance.
Materials and Methods
Study patients
This study was conducted between January 2010 and December 2011 at the retrovirology laboratory of the Centre International de Recherches Médicales de Franceville (CIRMF, Gabon). Whole blood specimens were collected in EDTA tubes from three Gabonese HIV care centers providing ART and located in Franceville (FCV) (a town of ∼75,000 inhabitants in the Haut-Ogooué province), Koulamoutou (KMO) (a town of ∼15,000 inhabitants in the Ogooué-Lolo province), and Libreville (LBV) (the capital city of Gabon in the Estuaire province). The study was approved by the ethical biomedical research committee of Franceville (No. 023/2010/MESRS/CERB). 4
Serotyping and molecular HIV-1/O assays
For HIV-1/O diagnosis, we implemented a variant serological strategy by using an in-house serotyping env gp120 V3 loop region immunoassay as described elsewhere. 7 For this purpose, five V3 peptide antigens were used for specific identification of HIV-1 groups M, N, O, and P, and HIV-2 infections. Plasma HIV-1/O RNA levels were determined using the Abbott RealTime HIV-1 assay (Abbott, Des Plaines, IL) according to the manufacturer's instructions.
Full-length HIV-1/O genomes
For full-length amplification of HIV-1/O strains, proviral HIV-1 DNA as well as circular HIV-1 DNA were extracted from whole blood using the Qiagen DNA extraction blood kit (Qiagen, Courtaboeuf, France). Based on full-length HIV-1/O sequences available in the Los Alamos HIV database (
All PCR amplifications were performed using the Long Expand PCR kit (Roche Applied Science, Indianapolis, IN) according to the manufacturer's instructions. Each amplification reaction included a manual hot-start followed by 35 to 40 cycles. Annealing temperatures were set according to the primer melting temperatures. Extension times varied depending on the size of the expected fragment and were typically set at 1 min/kb. PCR products were purified on 1% agarose gel with a QBIOgene GENECLEAN Turbo kit (MP Biochemicals). Direct sequencing of both strands using the Big Dye terminator technology [ABI PRISM Big Dye Terminator Cycle Sequencing Ready Reaction kit with AmpliTaq FS DNA polymerase (PE Biosystems, Warrington, England)] was performed on an ABI 3130xl Genetic Analyser. Sequences were then assembled using the software package Lasergene (DNASTAR, Inc., MAD). Overlapping sequence fragments were assembled using DNAstar package (Lasergene).
Newly derived HIV-1 group O Gag, Pol, and Env amino acid and nucleic acid sequences were aligned with 21 available and independent full length HIV-1/O sequences from the GenBank by using MEGA4 with minor manual adjustments if necessary. 8 Appropriate models of evolution were selected for each data set using Topali v2.5 software and maximum likelihood phylogenies were reconstructed using PhyML. 9,10 To define newly derived HIV-1/O clades, we used the classification proposed by Yamaguchi et al. 11
ARV resistance genotypic patterns
ARV drug resistance mutations were identified and interpreted using the ANRS algorithm (version 21, October 2011) (
Results
Prevalence rate of HIV-1/O infection
A total of 1,176 specimens were serotyped (FCV, n=544; LBV, n=457; and KMO, n=175). Four subjects (one from FCV and three from LBV) infected with an HIV-1/O strain were identified, yielding an overall prevalence of HIV-1/O infections in Gabonese HIV-1-infected subjects of 0.34% (95% confidence interval, 0.11–0.82). Among these four specimens, optical densities (ODs) found for the O peptide oscillated between 0.386 and 1.505 whereas ODs were strictly negative (<0.1) for the HIV-1 M, N, and P as well as HIV-2 peptides. No dual O+M specimen was observed. A vast majority (1,118/1,176; 95.1%) of patients were infected with HIV-1 strains belonging to group M whereas 51 (4.3%) subjects showed negative or indeterminate results. HIV-2 infection was found for three (0.26%) individuals, including two with a dual HIV-1/HIV-2 reactivity. No case of HIV-1 group N or P infection was found.
Epidemiological, clinical, and immunovirological characteristics of subjects infected with HIV-1/O strains
The main features of the four HIV-1/O-infected patients are presented in Table 1. Three were men. All subjects were aged >40 years. Two individuals were born at Oyem, a city located in North Gabon. At the time of HIV-1/O diagnosis, three patients progressed to CDC stage C. One subject (LBV#1744) who was untreated with ARVs died 2 months later (in March 2010). One individual (LBV#6947) was lost to follow-up from February 2011. Two patients, FCV#1190 and LBV#6352, treated with NNRTI-based regimens, were still alive by the end of 2011. At baseline, their CD4 counts were low. After 31 (for patient FCV#1190) and 19 (for patient LBV#6352) months of ART, their CD4 counts remained low or even decreased, and their HIV-1 RNA viral load (VL) results were 101,000 and 10,050 cp/ml, respectively.
HIV-1/O diagnosis by serotyping (see Materials and Methods section).
At the time of HIV-1/O diagnosis.
Two months after HIV-1/O diagnosis.
ART, antiretroviral treatment; VL, viral load; F, female; M, male; ND, not done; NA, not available; AZT, zidovudine; 3TC, lamivudine; EFV, efavirenz; d4T, stavudine.
Full-length genomes of HIV-1/O strains
On the four patients infected with HIV-1/O strains, two (FCV#1190 and LBV#6352) had sufficient material available for HIV-1/O full-length genome sequencing. GenBank accession numbers for sequences deposited in EMBL and analyzed in this study are 10Gab1190: JX245014, and 11Gab6352: JX245015. As depicted in Fig. 1, the 10Gab1190 strain clustered with high bootstrap values with HIV-1/O Ia clade (MABB197, CMA105, and Ant70 HIV-O as reference strains) on the three genes analyzed (gag, pol, and env). The amino acids Gag, Pol, and Env sequence analyses presented identical tree topologies although bootstrap values were nonsignificant (data not shown). The 11Gab6352 strain was at the root of the HIV-1/O Ib clade (with MABB1441 and US2478B as reference strains) in gag and pol nucleic sequences and with the HIV-1/O 1a clade in the env nucleic sequence. By using Gag, Pol, and Env amino acids sequences, the tree topologies were different (data not shown). In both nucleic and amino acids analyses, bootstrap values were nonsignificant, making the classification of this strain quite difficult.
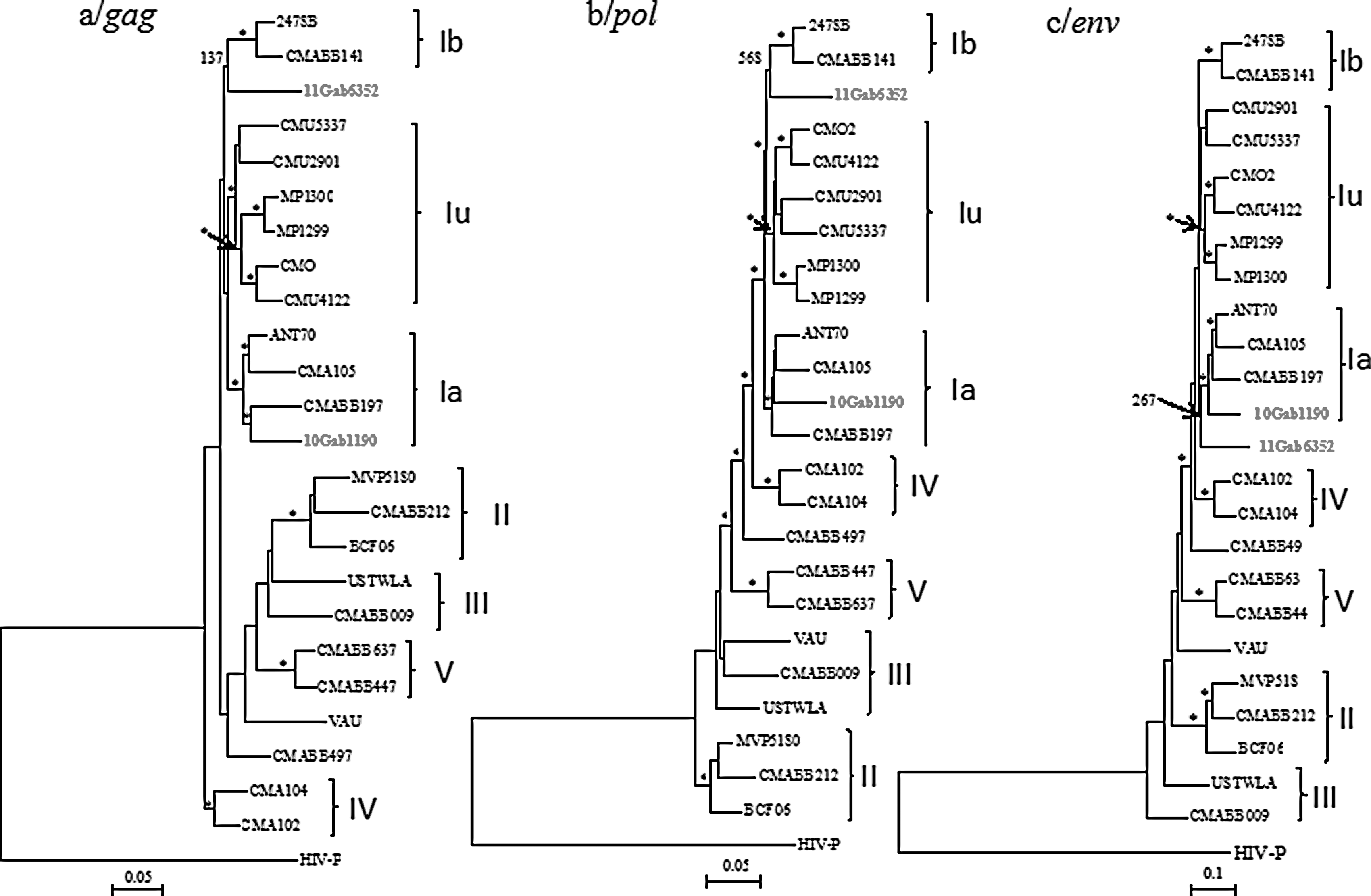
Phylogenetic relationships of two newly derived viruses (10Gab1190 and 11Gab6352) to the previously described strains in gag, pol, and env genes, as inferred by the maximum likelihood method from nucleotide sequence alignments (see Materials and Methods for further details). The classification used was proposed by Yamaguchi et al.8 Bootstrap values≥80% are indicated by an asterisk.
Antiretroviral drug resistance results
As shown in Table 2, at positions associated with resistance to NRTIs, the two strains HIV-1/O 10Gab#1190 and 11Gab #6352 harbored the uncommon mutations V118C and L210Y. The T69N mutation was observed for strain HIV-1/O 10Gab#1190 only. The M41L, M184V, and T215Y DRMs were found in the 11Gab#6352, making this strain resistant (intermediate or high-level) to all NRTIs according to the Stanford algorithm. According to the ANRS algorithm, this strain was resistant (intermediate or high-level) to zidovudine (AZT), stavudine (d4T), lamivudine (3TC), emtricitabine (FTC), and abacavir (ABC) but remained susceptible to didanosine (ddI) and tenofovir (TDF). When considering positions associated with resistance to NNRTIs (Table 2), the two HIV-1/O samples harbored the Y181C mutation making them resistant to first-generation NNRTIs. For etravirine, they were susceptible according to the ANRS algorithm but intermediate using the Stanford interpretation. For rilpivirine, they were intermediate with both algorithms. In the protease gene, multiple minor resistance mutations were found for both strains (Table 3). They remained susceptible to atazanavir, darunavir, fosamprenavir, indinavir, and lopinavir, whatever the algorithm used. They showed discrepancies between the two algorithms for nelfinavir, saquinavir, and tipranavir. A high natural polymorphism in the gag gene cleavage sites was obtained for both strains, mostly in the p1/p6, TFP/p6 pol , and p6 pol sites (Fig. 2). For the two strains, no major resistance mutation (such as E157Q) was detected in the integrase gene, indicating a conserved susceptibility to integrase inhibitors [(INI) such as elvitegravir (EVG), raltegravir (RAL), and dolutegravir (DTG)] with both ANRS and Stanford algorithms. The two samples carried the N42D mutation within the HR1 domain of gp41, conferring a resistance to enfuvirtide (ENF) according to the ANRS algorithm.
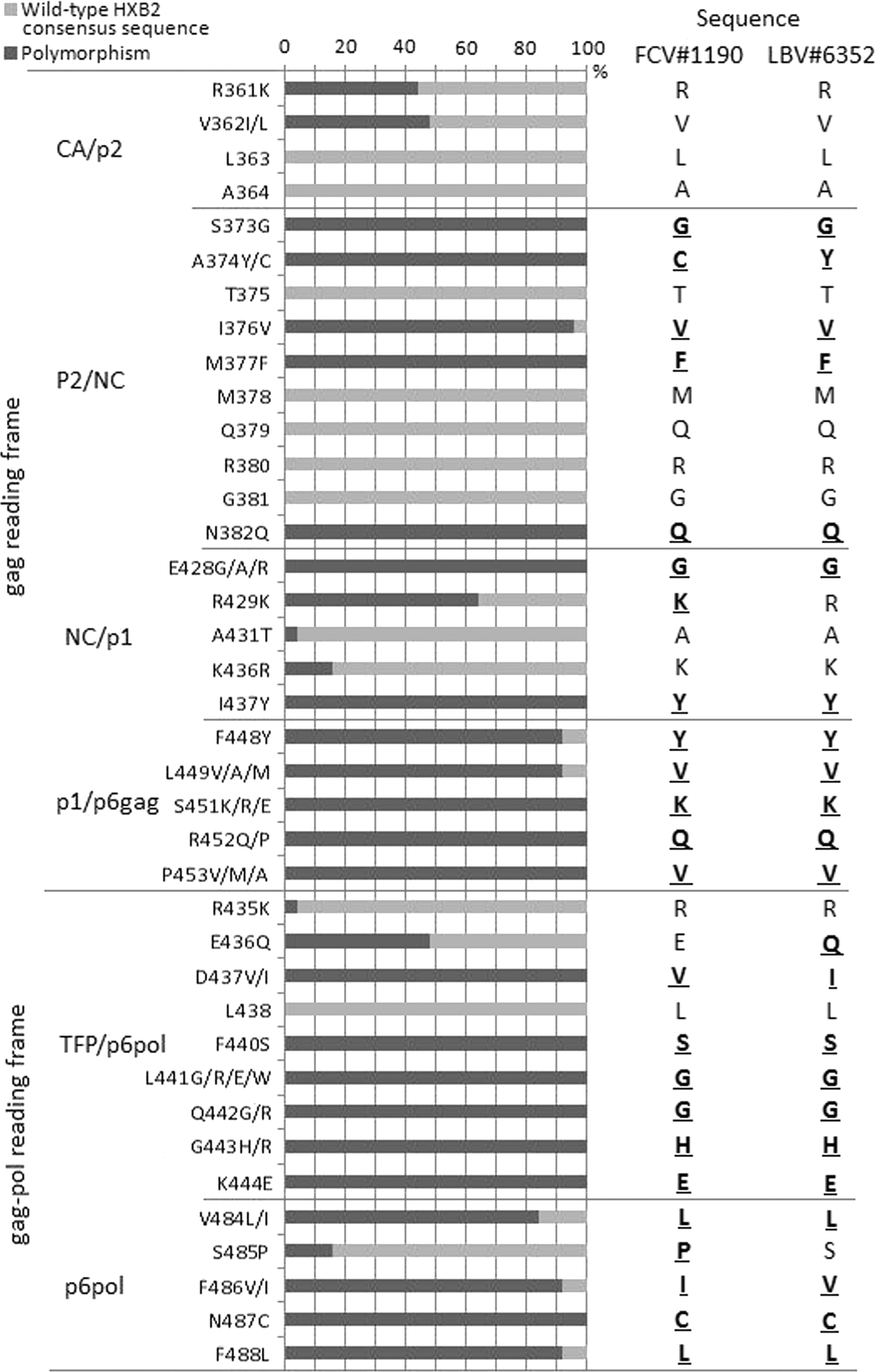
Gag and gag-pol cleavage site substitutions in two protease inhibitor-naive subjects infected with HIV-1/O strains in Gabon. Frequencies (horizontal bars) of each substitution were obtained from 21 independent HIV-1/O sequences (see Materials and Methods).
NRTI resistance mutations; **NNRTI resistance mutations.
Genotypic resistance interpretations are reported as follows: S, susceptible; I, intermediate level of resistance; R, resistance. For each drug, results are given as a fraction consisting of a numerator (ANRS interpretation) and a denominator (Stanford interpretation). For this purpose, the ANRS (version 21) and Standford (HIVdb, January 2012) algorithms were used.
3TC, lamivudine; ABC, abacavir; AZT, zidovudine; d4T, stavudine; ddI, didanosine; FTC, emtricitabine; TDF, tenofovir; NVP, nevirapine; EFV, efavirenz; ETR, etravirine; RPV, rilpivirine.
Genotypic resistance interpretations are reported as follows: S, susceptible; I, intermediate level of resistance; R, resistance. For each drug, results are given as a fraction consisting of a numerator (ANRS interpretation) and a denominator (Stanford interpretation). For this purpose, the ANRS (version 21) and Standford (HIVdb, January 2012) algorithms were used.
ATV, atazanavir; DRV, darunavir; FPV, fosamprenavir; IDV, indinavir; LPV, lopinavir; NFV, nelfinavir; SQV, saquinavir; TPV, tipranavir.
Discussion
It remains unknown why HIV-1/O variants constitute a low-level background in their contribution to the global HIV/AIDS pandemic, contrary to the dramatic increase of HIV-1M strains. In our study, we confirmed a low HIV-1 group O prevalence in Gabon, accounting for only 0.3% (95% CI, 0.1–0.8) of HIV-1 infections diagnosed in 2010–2011. It is lower than the 0.9% (95% CI 0.2–3.0) rate previously reported for this country in 1997. 3 Given that the p value between the two prevalence rates was not statistically significant (χ2 test, p=0.22), we were not able to draw solid conclusions about the trend (declining or stable or increasing) of HIV-1/O prevalence over time in Gabon. Even if two individuals were born in Oyem, a Gabonese city located in the Woleu-Ntem province, it was difficult to demonstrate higher prevalence rates of HIV-1/O infections in North Gabon compared to other Gabonese areas. North Gabon is just neighboring to Cameroon, which is known to be the epicenter of HIV-1/O infections. 11 –13
In our study, full-length genome analyses revealed that one strain (10Gab1190) clustered with the ANT70 archetype HIV-1/O strain along its whole genome. By contrast, the 11Gab6352 strain remained unclassifiable. Given that only 21 independent HIV-1/O full-length genomes are available in the HIV sequence database (
Little is known about the efficacy of antiretroviral drugs on HIV-1/O strains, with sometimes a poor agreement between the genotypic resistance testing results designed for HIV-1 group M and in vivo virological responses. 14,15 For the two HIV-1/O strains well-characterized in our study, and as previously described by other teams, we found a wide range of natural polymorphism in the protease, gp41, gag, and gag-pol regions such as (1) about 15 natural sequence polymorphisms in the protease (that may contribute to a more rapid virological failure to PIs), 16 (2) the signature N42D mutation in the gp41 (whose impact on ENF needs to be further assessed in vivo), 17 (3) and a high polymorphism in some gag and gag-pol cleavage sites (which may be associated with a higher risk of virological failure on PI-based monotherapy). 18 Conversely, no polymorphism was observed in the integrase gene, as reported by others. 19 For the reverse transcriptase gene, we were not able to determine if mutations were due to ARV pressure or were naturally present before ARV treatment. The presence of the Y181C mutation made the two strains resistant to first-generation NNRTIs, whereas a few minor mutations (A98G, V179E) led to possible resistance to newly developed NNRTIs such as etravirine and rilpivirine. In addition, the 11Gab#6352 strain harbored M184V and some TAM-1 mutations (M41L, T215Y) leading to resistance to all NRTIs using the Stanford algorithm. As a consequence, this viral strain was predicted to be resistant to all three drugs constituting the ARV regimen. Patient LBV#6352 was thus clearly infected with a multidrug-class-resistant HIV-1/O strain and is still waiting for a salvage ARV regimen such as TDF+IP/r (such as LPV/r)+INI (such as EVG or RAL) whose access is quite difficult in Gabon. The efficacy of an INI-based regimen has been recently reported for one patient in Cameroon. 20
In conclusion, individuals infected with HIV-1/O variants are rare in Gabon. However, they should be diagnosed earlier and accurately followed-up in order to switch without delay from inefficient NNRTI-based regimens to appropriate ARV regimens including PIs and/or INIs.
Footnotes
Acknowledgments
François Rouet is supported by the French Ministry of Foreign and European Affairs. We are indebted to all patients who participated in this study. This work is dedicated to Dr. Chantal Zamba who died in December 2012 in Libreville.
Author Disclosure Statement
No competing financial interests exist.