
Abstract
Physical disability is a major priority in aging, affecting morbidity, mortality, and quality of life. Despite the large number of adults aging with HIV, our understanding of the physiologic and clinical risk factors for disability is limited. Our goal is to determine whether the Veterans Aging Cohort Study (VACS) Index, based on routine clinical blood tests, could serve as a point of care screening tool to identify HIV-infected adults at high risk for physical disability. HIV-infected adults enrolled in the VACS participated in a cross-sectional exercise study with established measures of strength and endurance. The VACS Index was calculated using recent clinical laboratory values and age; a higher score reflects greater mortality risk. Statistical analyses included correlation and linear regression models adjusted for muscle mass. Fifty-five HIV-infected adults, predominantly African-American men, were included with age mean±SD of 52±7 years. Median (IQR) CD4 cell count was 356 cells/mm3 (212–527). The VACS Index was inversely correlated with quadriceps strength (r=−0.45, p<0.01), grip strength (r=−0.28, p=0.04), and 6-min walk distance (r=−0.27, p=0.05). A 20-point increase in VACS Index score was associated with a 10% lower leg strength (p<0.01), which remained significant after adjustment for muscle cross-sectional area (p=0.02). The VACS Index explained 31% of the variance in specific leg strength. In this group of middle-aged adults with well-controlled HIV infection the VACS Index was significantly associated with upper and lower extremity strength. The VACS Index may be valuable for identification of patients at high risk for disability due to muscle weakness.
Introduction
P
Our work in the Veterans Aging Cohort Study (VACS) shows that approximately half of HIV-infected adults report limitations with vigorous activities, 4 which agrees with other survey results. 5 Among patients with chronic lung disease, HIV-infected adults are more likely to report physical limitations compared to adults without HIV. 6 These findings are consistent with research using objective measure of functional performance or exercise capacity. In a VACS substudy including performance of the 6-min walk (6-MW), a standard measure of ambulatory function and endurance, 7 respiratory symptoms correlated with a shorter 6-MW distance in HIV-infected adults, but not HIV-uninfected adults. 8 Treadmill testing in studies of HIV-infected adults shows a significant deficit in endurance that is related to anemia, 9 hypertension, 10 and the use of thymidine analogue nucleoside reverse transcriptase inhibitors (NRTIs). 11
In contrast to endurance, deficits in strength among HIV-infected adults in the cART era are not as definitive. Grip strength in HIV-infected women is significantly lower compared with demographically similar uninfected women, but only among those with low CD4 cell count or a history of AIDS. 12 The difference, only 2–4 kg, was attenuated when adjusted for body mass index (BMI). Among older (50+ years) adults in South Africa, grip strength of HIV-infected individuals was on average 4.7 kg lower compared to uninfected individuals. 13 However, results were not adjusted for BMI, which was significantly lower in the HIV group. It is not surprising that strength is strongly affected by muscle mass in HIV-infected adults due to the propensity for wasting of lean tissue, 14 which remains an issue and independently predicts mortality. 15 In patients with AIDS wasting syndrome, lower extremity strength strongly correlates with muscle mass and quality of life. 16 More recently Yaresheski and colleagues reported that muscle mass is significantly lower in middle-aged HIV-infected men compared with uninfected men. 17 This deficit did not change over the 5-year follow-up, raising the question of whether HIV-infected adults have increased risk of aging-related loss of skeletal muscle (i.e., sarcopenia). The relationships of muscle loss with weakness, and clinical risk factors, besides AIDS-related conditions, 18 remain to be defined.
It is likely that physical disability in older HIV-infected adults is associated with burden of disease and overall risk of mortality. The Veterans Aging Cohort Study Index (VACS Index) was developed in HIV-infected adults to identify individuals at high risk for morbidity and mortality using readily available clinical laboratory data. The VACS Index predicts all-cause mortality across large cohorts of HIV-infected adults, 19 –21 in addition to medical intensive care hospitalizations 22 and bone fracture. 23 In adults without HIV a well-studied geriatric metric, the frailty phenotype, predicts mortality, hospitalizations, 24 bone fracture, and disability, 25 but requires measurement of grip strength and gait speed. Markers of chronic inflammation are independently associated with both the VACS Index 26 and the frailty phenotype. 27
Our goal is to determine whether the VACS Index could serve as a point of care screening tool to identify HIV-infected adults at high risk for physical disability. Our first step, and the aim of the current study, is to determine the association of the VACS Index with exercise capacity. We included gold standard measures of endurance (treadmill testing) and strength (isometric KinCom testing) to conduct a cross-sectional study as a test of concept. We also compared the association of the VACS Index to functional performance measures of endurance, the 6-MW test, and of strength, the grip test, to assist in future longitudinal research to determine VACS Index cut-off values that predict disability.
Materials and Methods
Participants
Between 2004 and 2007, 58 HIV-infected patients participated in a cross-sectional study of exercise capacity at the Baltimore VA Medical Center. Study exclusion criteria included history of an AIDS-defining illness (ADI) in the prior 6 months and conditions that increase the risk of exercise treadmill testing per the American College of Sports Medicine, such as very poorly controlled hypertension. 28 Complete laboratory data required for calculation of the VACS Index were not available for three participants; the remaining 55 participants represent the analytical set of the current study. All research was approved by the University of Maryland, Baltimore Institutional Review Board and the Baltimore VA Medical Center Research and Development Committee, and included written informed consent.
VACS Index
The VACS Index is a weighted scale that includes additional points for increased age and abnormal laboratory values on eight routine clinical tests: CD4 count, HIV-1 RNA, hemoglobin, platelets, aspartate transaminase (AST), alanine transaminase (ALT), creatinine, and hepatitis C infection. 19 Definitions, cut-off values, and scoring are provided in Table 1. The VACS Index was calculated for each subject using the most recent clinical laboratory values within a year of exercise testing. An index restricted to CD4 count, HIV-1 RNA, and age (restricted index) also was calculated.
FIB, fibrosis index; ALT, alanine transaminase; AST, aspartate transaminase; FIB 4: (years of age×AST)/(platelets in 109/L×square root of ALT); eGFR, estimated glomerular filtration rate: 186.3×(serum creatinine−1.154)×(age−0.203)×(0.742 for women)×(1.21 if black).
Hepatitis C: diagnosis, positive antibody test or detectable virus.
Exercise capacity
Endurance was quantified as total exercise time and maximum metabolic equivalents (METS) during a modified Bruce treadmill protocol. 28 METS were based on measured oxygen consumption (VO2peak) rather than formula estimates. Subjects walked on a motorized treadmill starting at a speed of 1.7 mph and 0% incline with workload increased every 3 min, by incline only at first, then by both incline and speed. Exercise time was measured from the beginning of the protocol until voluntary exhaustion or safety criteria for termination were reached. 28 Breath-by-breath oxygen utilization, carbon dioxide production, and minute ventilation values were averaged at rolling 10-s intervals using a SensorMedics V max 29C series metabolic cart. Peak oxygen utilization (VO2peak) was recorded as the average of the last two VO2 values during exercise, and then was translated into METS. The 6-MW test was conducted according to the guidelines of the American Thoracic Society. 29 Subjects were instructed to walk at their fastest comfortable pace on an even surface between two cones for 6 min. The total distance covered was measured.
Muscle strength was measured as the average force generated by the knee extensors (quadriceps) during three trials of maximum voluntary isometric contraction (MVC) with the subject sitting and the knee in 90° of flexion (KinCom dynamometer, Chattanooga, TN), as previously described. 18 Hand grip strength was measured using a dynamometer and the average of three trials of the dominant hand (Lafayette hand dynamometer).
Body composition
Results from dual-energy X-ray absorptiometry (DXA) (Model GE iDXA Scan) included total body and lower extremities lean tissue mass and total percent body fat. Quadriceps cross-sectional area (CSA) was determined from a single mid-thigh image by computed tomography (CT; Siemens Somatom Sensation 16) using Medical Imaging Process Analysis and Visualization software (MIPAV, version 2.7.47). BMI was calculated as weight/(height) 2 based on measurements from the same scale.
Statistics
Data distribution was tested by the Shapiro–Wilk test for normality. Pearson correlation (Spearman if distribution was not normal) was used to test associations between the VACS Index or the restricted index with exercise capacity and body composition. Linear regression analyses were used to determine the relationship of exercise capacity with the VACS Index. Regression models of strength were adjusted for muscle mass. Analyses were performed using STATA software (v10.0, Stata Corp, College Station, TX). All analyses were two-tailed.
Results
The VACS Index, exercise, and body composition data had a normal distribution with the exception of time on treadmill. The mean±SD VACS Index was 33.6±16.7 with median (range) score of 31 (0–75). The mean±SD restricted index (based on CD4, viral load, age) was 27.8±17.2 with a median (range) score of 33 (0–88). The mean±SD age was 52.3±7.4 years in the 53 male and two female participants, of whom 91% were of African-American race. Participant characteristics based on the VACS Index scoring categories are summarized in Table 1. Median (IQR) CD4 cell count was 356 cells/mm3 (212–527). All participants were receiving combination antiretroviral therapy including NRTIs; additional medications included protease inhibitors (78%), nonnucleoside reverse inhibitors (10%), or both (6%). However, 39% (N=21) had a prior history of an AIDS-defining illness. Current cigarette smoking was reported by 66%. History of heroin or cocaine use was reported by 82% of the participants, with active use in the prior year in 10 subjects. The most common non-HIV conditions were hypertension (42%), dyslipidemia (31%), diabetes (13%), and chronic obstructive pulmonary disease (9%).
The mean (±SD) BMI was 24.7 (±4.5) kg/m2. DXA and thigh CT scans were added to the study after it began and were performed in 91% (N=50) and 87% (N=48) of participants, respectively. Results are summarized in Table 2. Quadriceps strength had a stronger correlation with quadriceps cross-sectional area (r=0.51, p<0.001) than with leg lean mass (r=0.26, p=0.07), and the former was used in the adjusted model of quadriceps strength. Grip strength correlated with total lean mass (r=0.39, p<001). Total percent body fat was not associated with skeletal muscle mass or area (all p>0.2). The VACS Index correlated with skeletal muscle mass and area, but not percent body fat (Table 2).
Pearson.
Spearman.
By DXA (n=50) and CT (n=48).
Exercise capacity results are summarized in Table 2. A higher VACS Index score was consistently associated with worse exercise capacity but was statistically significant only for strength measures. The association was strongest for quadriceps strength (r=−0.45, p<0.01), followed by hand grip strength (r=−0.28, p=0.04) and 6-min walk distance (r=−0.27, p=0.05), and was weakest for METS (r=−0.21, p=0.1) and time on treadmill (rho=−0.20, p=0.2) (Table 2). The restricted index did not significantly correlate with any of the exercise measures. Results of bivariate linear regression models were consistent with correlation testing. A 20 point increase in the VACS Index score (β=−84; 95% CI: −132, −36; p<0.01) was associated with a 10% lower leg strength, which remained significant after adjustment for muscle cross-sectional area (p=0.02) (Fig. 1). The VACS Index explained 31% of the variance in specific leg strength. Grip strength was on average 2.6 kg lower per 20-point higher VACS Index score (β=−2.6 ; 95% CI: −5.1, −0.1; p=0.04), which was attenuated after adjustment for total lean mass [β=−1.42 kg; 95% CI (−4.3, 1.5); p=0.3].
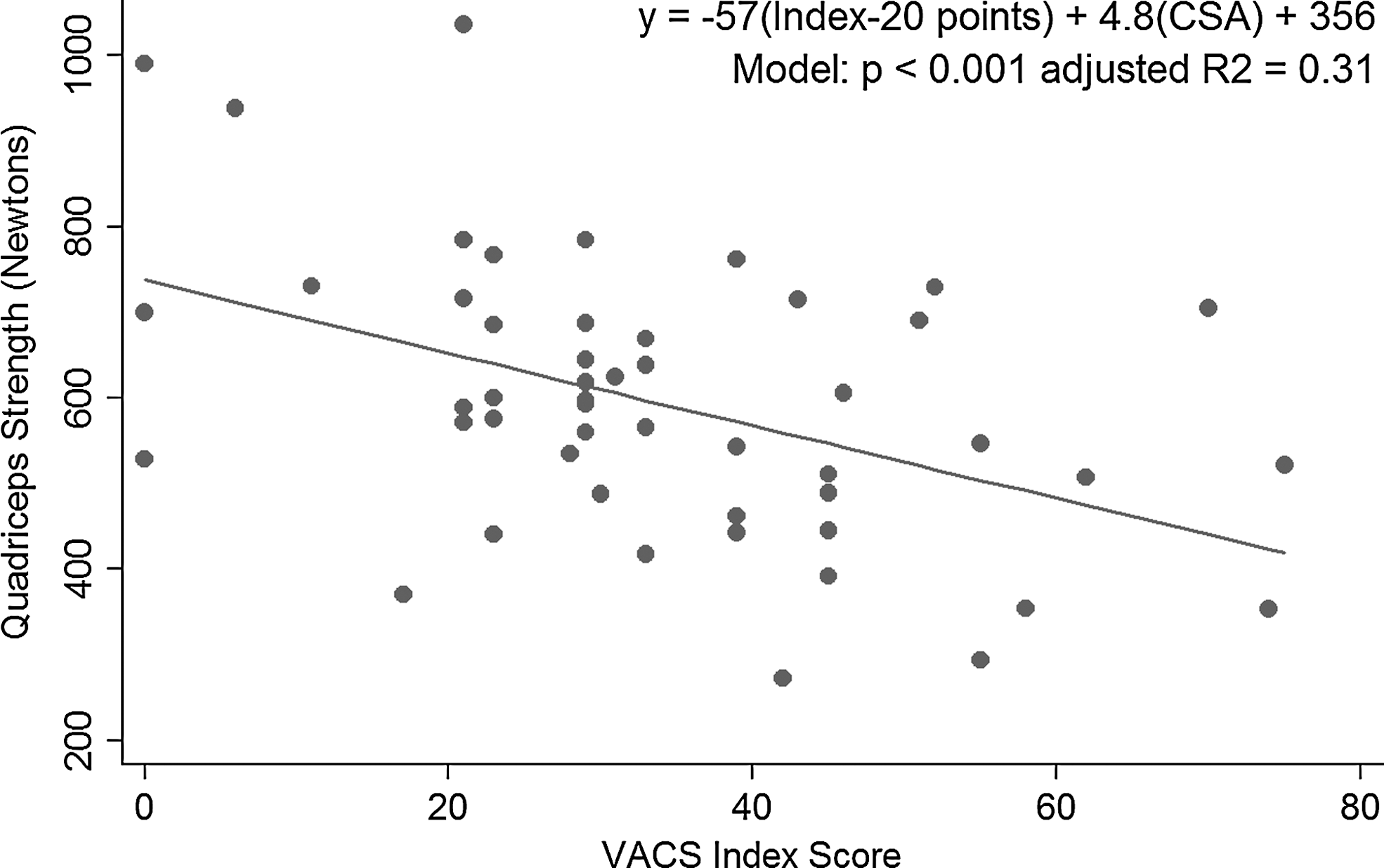
VACS index predicts quadriceps strength adjusted for muscle cross-sectional area (CSA).
Discussion
This study presents novel results on the relationship of the VACS Index to exercise capacity in older adults with stable chronic HIV infection on antiretroviral therapy. In these patients, we found a moderate correlation between the VACS Index and strength that was statistically significant and clinically relevant. Our findings support further investigation of the VACS Index as a screening tool to identify patients at high risk for disability.
Studying muscle strength is challenging due to the complex relationship between muscle size, quality (intramuscular adiposity), and muscle fiber types, which vary between individuals and over time. 30 Therefore universal cut-off strength values for large muscle groups that predict disability are not well established. However, longitudinal research in elderly adults without HIV (age ≥70 years) demonstrates that baseline quadriceps strength predicts mortality, independent of muscle cross-sectional area and comorbidity. 31 In HIV-infected adults, change in muscle strength with aging is unknown. The Study of Fat Redistribution and Metabolic Change in HIV Infection (FRAM) performed whole-body 1 H-magnetic resonance imaging in HIV-infected adults and healthy controls at baseline and after 5 years. 17 Compared with the healthy men, age-matched HIV-infected men without a history of opportunistic infection had significantly less muscle mass. The muscle mass decline observed over 5 years was similar between the men, who were a median age of 41 years. The implications for disability are limited by the absence of strength or physical function data and lack of older participants. A recent cross-sectional study of ambulatory function in HIV-infected adults (median age 48 years, 80% men) further suggests that impaired strength in older HIV-infected men translates to physical limitations. 32 Richert and colleagues 32 found that 53% of the participants had poor performance in the chair-rise test, which was the most common mobility limitation. Although leg muscle strength was not directly measured, chair-rise performance in elderly adults is dependent on quadriceps strength and independently predicts disability 33 and mortality. 34
Hand grip strength predicts mortality across a wide age span, 35 but does not always predict progressive disability. 36 In elderly adults (age ≥70 years) enrolled in the Health, Aging, and Body Composition Study, a 10-kg lower grip strength at baseline was associated with a 45% increased risk of death over 5 years. 31 We are only beginning to characterize grip strength in HIV-infected adults, and results in older individuals and mortality risk are scarce. In middle-aged HIV-infected men on cART we have shown that grip strength is only 10% lower than expected (41 kg). 9 Similarly, the Women's Interagency HIV Study (WIHS) found that the average grip strength (30 kg) was the same for HIV-infected women (mean age 41 years) with a high CD4 cell count (≥350 cells/mm) compared with uninfected women. 12 It should be noted that grip strength in these two HIV studies was significantly higher compared with BMI-based threshold values used in the frailty phenotype for uninfected elderly men (29–32 kg) and women (17–21 kg). 24 The significant correlation between grip strength and VACS Index, while modest in magnitude, was noteworthy given the relatively intact strength. Interestingly, when grip strength is included with measures of weight loss and walking speed as part of the frailty phenotype, younger HIV-infected adults are 2-fold more likely to be considered frail than age-matched uninfected adults. 37 Therefore, while our conclusions are limited to cross-sectional relationships, these findings suggest that the VACS Index may be sensitive to preclinical loss of strength. Future research in a larger and more diverse HIV-infected patient population is needed to establish a threshold value of the VACS Index across BMI categories which is associated with weakness and predicts disability.
We were surprised to find a relatively weak correlation between the VACS Index and endurance. Our prior work with treadmill testing of older HIV-infected adults shows that time on treadmill and METS were significantly lower in those with hypertension and anemia. 9,10 Preliminary work with the 6-MW shows endurance is reduced in HIV-infected adults with pulmonary symptoms. 8 The 6-MW is a reliable measure of exercise capacity in patients with heart failure 38,39 and lung disease, 40,41 with performance of less than 350 m predictive of mortality. 7 A possible reason for our results is that the VACS Index, based on laboratory values, does not directly include measures of cardiovascular or pulmonary disease. This rationale is supported by preliminary results from Erlandson and colleagues who found a similar weak association between the VACS Index and endurance, measured by the long-distance corridor walk in 305 HIV-infected men 45–65 years of age. 42 However, since the VACS Index predicts cardiac-related mortality, 43 another possibility is that our study had an insufficient number of subjects with poor endurance. None of the subjects had a 6-MW distance <350 m (range 371–690) and only 25% of the subjects met Social Security Administration treadmill criteria for disability (5 METS). 44 Therefore, our findings may be affected by the relatively narrow spectrum of cardiopulmonary disease. Future research in HIV-infected adults with a wide range of cardiac and pulmonary function is needed to determine the utility of the VACS index to predict endurance. Investigation of the relationship of endurance to established risk factors for cardiopulmonary disease, such as smoking, will provide further understanding of mechanisms of physical disability and modifiable factors.
The primary limitation of the study is the limited diversity of the study population, who were predominantly African-American men receiving cART who were able to perform treadmill testing. Since our participants were relatively healthy, we would expect the results to be biased to the null. Therefore, generalization of findings to other patients groups should be done with caution. In addition, given the small sample size and select patients, we analyzed the VACS Index as a continuous measure, and did not attempt to define cut-off values of the VACS Index associated with exercise capacity.
In conclusion, these findings provide additional evidence that the VACS Index is a metric for loss of physiologic reserve that extends beyond traditional prognostic indicators used in HIV-infected adults. Numerous cross-sectional studies demonstrate that physical limitations are more prevalent in HIV-infected adults compared with uninfected adults based on endurance, 9,11 muscle mass, 17 functional performance, 32 self-reported frailty-related phenotype, 45 and frailty phenotype. 37 However, the relevance to mortality and disability is yet to be defined. These findings help advance our understanding of the risk factors for physical disability in adults aging with HIV.
Footnotes
Acknowledgments
Disclosure of Funding: National Institute on Aging (NIA) K23 AG024896 (Dr. Oursler), NIA University of Maryland Claude D. Pepper Older Americans Independence Center P60-AG12583 (Drs. Oursler and Sorkin), Baltimore VA Geriatric Research, Clinical and Education Center (Drs. Oursler and Sorkin), NIA K24AG021507 and P30AG021342 (Dr. Gill), NHLBI R01 HL090342 (Dr. Crothers), NINR K01 NR013437 and CTSA NCRR UL1 RR024139 (Dr. Womack), and NIAAA U10-AA13566 and U24-AA020794 and in kind by the U.S. Department of Veterans Affairs (Dr. Justice).
Author Disclosure Statement
No competing financial interests exist.