
Abstract
Although 2-long terminal repeat (2-LTR) circles are only a fraction of the total viral DNA in infected cells, sequence analysis of 2-LTR circles reveals critical information regarding viral DNA synthesis and the nature of actively replicating virus. It was observed that a large proportion of the 2-LTR circular molecules in the peripheral blood mononuclear cell (PBMC) DNA of infected individuals are mutated at the circle junction. The integrase inhibitor raltegravir (RAL) blocks the strand transfer step of the integration of HIV-1; as a consequence of abortive integration a significant increase of episomal 2-LTR circles is observed. Moreover, it was demonstrated that in patients treated with highly active retroviral therapy (HAART) changes in 2-LTR concentration did not affect junction sequences and flanking regions of 2-LTR. Here we evaluated whether RAL therapy could have a differential impact on the 2-LTR circle junctional sequences in patients with different virological profiles at the time of starting RAL therapy. Sequence analysis indicates that RAL acts differently in the two populations.
T
Although 2-LTR circles are only a fraction of the total viral DNA in the infected cells, sequence analysis of 2-LTR circles reveals enormous critical information regarding viral DNA synthesis and crucial processes mediated by reverse transcription (RT). Interestingly, Sharkey et al. 6 recently demonstrated that analysis of envelope sequences from 2-LTR circles provides information about the nature of actively replicating virus and suggests the use of episomal HIV-1 as an additional or alternative approach to characterize virus that is maintained during highly active antiretroviral therapy (HAART). Previous analysis of 2-LTR junction sequences demonstrated that a large proportion of the 2-LTR circular molecules in the peripheral blood mononuclear cell (PBMC) DNA of infected individuals is mutated at the circle junction 7 –9 ; moreover, Zhu and colleagues demonstrated that in HAART-treated patients changes in 2-LTR concentration did not affect junction sequences and flanking regions of 2-LTR. 10
To date, little is known about 2-LTR junctional sequences in patients with or without detectable plasma viremia starting a new RAL-containing regimen. To this aim, 21 HIV-1-positive patients from an ongoing multicenter observational study on the use of new antiretroviral inhibitors were enrolled (Table 1). At the time they received their first RAL treatment 13 patients had HIV-1 RNA plasma levels >50 copies/ml (group D=detectable) while eight patients had HIV-1 RNA<50 copies/ml for at least 6 months (group U=undetectable). Their median age was 42 and 49 years and the median interval from HIV-1 diagnosis was 8 and 11 years for groups D and U, respectively. The median CD4 T cell count was 299 cells/mm3 for group D and 390 cells/mm3 for group U individuals (p=0.515). Most of the patients were white. All the patients had a long history of HAART therapy (median 10.5 and 7.0 years in groups D and U, respectively) and at study entry all patients were receiving a nucleoside reverse transcriptase inhibitor (NRTI) backbone, overall zidovudine–lamivudine (ZDV–3TC, n=9) or tenofovir–emtracitabine (TDF–FTC, n=4) or didanosine–lamivudine (ddI–3TC, n=4), in association with a protease inhibitor (PI) or nonnucleoside reverse transcriptase inhibitor (NNRTI). All the patients changed their previous drug regimen in the new RAL-based therapy (Table 1), optimized on the basis of the patients' drug resistance or intolerance. No differences between groups were observed regarding age, sex, ethnic origins, and CD4 levels. After 1 month of RAL-based treatment all patients had undetectable plasma viremia, and CD4 cells increased in both group D and group U patients.
Values are expressed as median and range or percentage.
HAART, highly active antiretroviral therapy; NRTI, nucleoside reverse transcriptase inhibitor; NNRTI, nonnucleoside reverse transcriptase inhibitor; PI, protease inhibitor; FI, fusion inhibitor; RAL, raltegravir.
At baseline, 2-LTR circles were amplified with primer pair 9600/515, obtaining a fragment of 220 bp encompassing the 2-LTR junction as described. 8 Negative samples were further processed in a nested reaction carried out using 5 μl of a 45 cycle direct polymerase chain reaction (PCR) and the inner primers 477/516 as previously described, 8 or amplified using the primer pair HIV-F/HIV-R1 spanning the junction. 11 PCR products were size selected, gel purified, and cloned into the pCR2.1 vector using the TA cloning kit (Invitrogen). Inserts were sequenced with T7AS primer using an ABI/Prism-377 DNA sequencer (PerkinElmer) and aligned using the AlignX program of the Vector NTI Advance suite from Invitrogen.
2-LTR junctions were detected and sequenced in 20 out of the 21 patients included in the study (95%); at day 15 and at day 30 after starting RAL therapy 2-LTR circles were detected and sequenced in 90% and 86% of the patients, respectively. Curiously, the only individual with undetectable 2-LTR circles both at baseline and after RAL treatment had a plasma viral RNA level at baseline >13,000 copies/ml. This might be explained by sequence variations at the LTR junction sequence preventing 2-LTR circle amplification.
The sequence data derived from both populations displayed sequence heterogeneity across the circle junction, as already observed. 7,8 In particular, we classified these junctions as follows: (1) Consensus junction: when the complete sequence from the ends of the linear viral DNA is present with unprocessed 2-LTR termini, probably due to an ineffective IN; (2) Deletions: removal of at least three nucleotides at either or both LTR ends, due to the 3′ processing activity of a partially effective IN, which removes the terminal GT dinucleotides without completing the integration reaction and theoretically increasing accessibility of viral LTR ends to cellular nuclease 2 ; (3) Insertions: one or more additional nucleotides inserted between LTRs termini, due to erroneous or incomplete cleavage by RNase H during reverse transcription with retention of viral sequences (PPT adjacent to the 3′ LTR and/or PBS regions adjacent to the 5′ LTR) 7,9 ; (4) Partially Processed junctions: sequences partially processed for integration with removal of one or both the terminal GT; and (5) Mixed junctions: containing both deletions and insertion. None of the cloned circle junctions found possessed two correctly processed ends predicted for integration. Nucleotide sequences derived from patient samples at any time point are reported in Fig. 1.
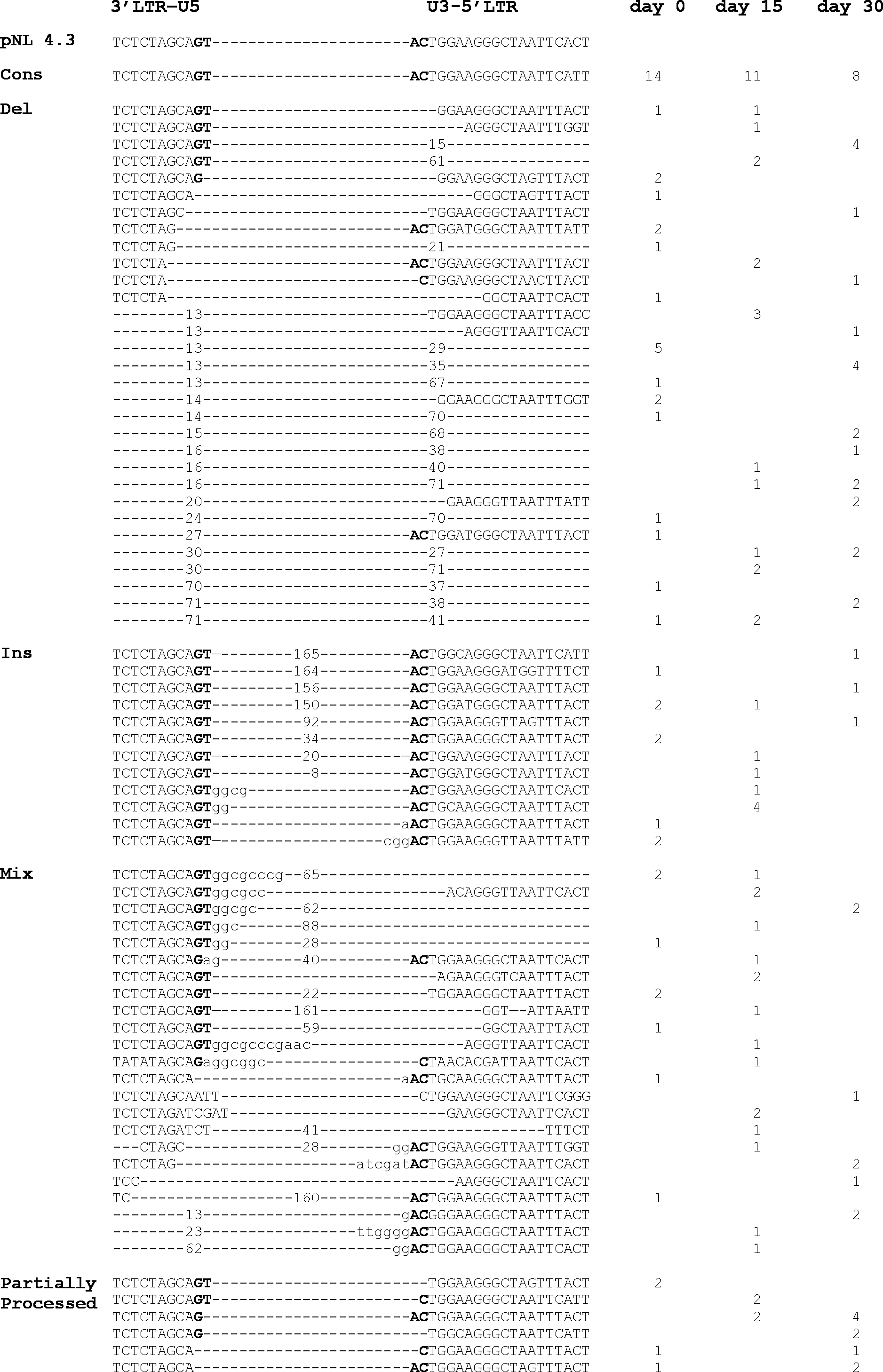
Sequence analysis of 2-long terminal repeat (2-LTR) circle junctions in HIV-1-infected patients before and after raltegravir (RAL) treatment. Sequences were aligned with the pNL4.3 molecular clone consensus 2-LTR junctional sequence (top) using the AlignX program of the Vector NTI Advance suite from Invitrogen (Carlsbad, CA). Dashes indicate gaps introduced for alignment; large deletions or insertions are indicated by+or – followed by the number of nucleotides deleted or inserted. The total number of each detected sequence is shown for each time point. The invariant GT and AC nucleotides are shown in bold. Nucleotides in lower case letters are those derived from the tRNA primer binding site or from the PPT next to the U3. Sequences evaluated and included in the analysis were only those that differed from each other, when derived from the same polymerase chain reaction (PCR), or were identical, when obtained from different PCR amplification.
Sequences evaluated and included in the analysis were only those that were different from each other, when derived from the same PCR reaction, or were identical, when obtained from a different PCR amplification; this approach allowed comparisons of independent viral clones from the same individual. As shown in Fig. 2, RAL treatment caused variations among the different junctional classes in both populations but there is statistical significance only in group D (Fig. 2a). In particular, sequence analysis showed an evident decrease in the frequency of consensus junctions and insertions, while deletions increased over time, as already observed. 2,5 Junctional sequences with a mixed phenotype gave rise to a wave trend while partially processed junctions showed a statistically significant increase at day 30, switching from 9% at day 0 to 28% at day 30 (p=0.021). Conversely, in group U patients RAL therapy induces modest but not significant fluctuations among the different classes of junctions (Fig. 2b) producing a random pattern. Sequence analysis at baseline showed that group D individuals had 2-LTR junction sequences more homogeneously distributed among the different classes than group U individuals.

Frequencies evolution of 2-LTR junction sequences in group D
Different studies 12,13 reported that in some patients on HAART with viral load below 50 copies/ml, much of the residual viremia consists of one or two predominant plasma clones. Thus, the existence of these predominant clones could explain the nonhomogeneous distribution of the 2-LTR junction at baseline in group U individuals. Namely, the different distribution in the two groups could be related to the presence of the widest pool of replicating viruses in patients with detectable viremia with respect to patients with undetectable viremia. Although we did not associate the viremic status of our patients with the presence of predominant plasma clones or with their resistance profile, it is possible that the high rate of virus replication in these individuals would lead to a higher degree of virus diversity, favoring a wider distribution among junctional classes.
Interestingly, after RAL treatment, 2-LTR junction analysis showed a clear increase in deleted sequences and a statistically significant increase in partially processed sequences (p=0.021) only in group D patients. Previous in vitro and in vivo studies 1,2,5 reported a high prevalence of deleted junctions after IN inhibitors; however, in these studies deleted and partially processed junction sequences were combined in a single class. We differentiate between these two different classes as we hypothesize that the increase in partially processed junctions following RAL treatment might be ascribed to the mode of action of strand transfer IN inhibitors. 14 In this model, referred to as “interfacial inhibition,” the drug takes advantage of transient energetic or structural conditions created by the macromolecular complex, which allows drug binding. The binding site becomes completely available only after the removal of 3′-GT nucleotides on the catalytic strand. 14,15 Thus RAL stabilizes the macromolecular IN-viral DNA complex at the 3′-processing step of the reaction, inhibiting integration. When the IN inhibitor dissociates from the complex, cellular enzymes are thought to act either by repairing or “eating” single-stranded DNA breaks, leading in this case to a 2-LTR circle containing partially processed junctions.
Additional studies need to be done to better evaluate the correlations between plasma viral load, circle junction sequences, and quantification in the absence and presence of RAL. Moreover, it would be important to monitor 2-LTR dynamics and junctional sequences in these patients over time, with particular attention to the emergence of RAL-resistant viruses. In fact, in the case of limited functionality or therapeutic failure of this IN inhibitor in patients with detectable viral load, the proportion of partially processed junctions might return to pretreatment levels, confirming that RAL has become only partially effective.
Sequence Data
GenBank accession numbers for the sequences of this study are KF060956–KF061019.
Footnotes
Acknowledgments
We thank Mrs. Stefania Donnini for secretarial help and Dr. Marina Franco for editorial assistance. The following reagents were obtained through the AIDS Research and Reference Reagent Program, Division of AIDS, NIAID, NIH: HTLV-IIIB/H9 virus from Robert Gallo. This study was carried out with financial support from the Italian AIDS National Program (RF-ISS-2009-1300961 to A. Cara).
Author Disclosure Statement
No competing financial interests exist.