
Abstract
In Hong Kong, the CCR5 antagonist has recently been introduced into salvage therapy for multiclass drug-resistant HIV-1-infected patients. Coreceptor usage must be determined prior to the usage of the CCR5 antagonist, which does not inhibit X4-tropic viruses. This study aimed to determine the tropism prevalence for HIV-1 subtypes B and CRF01_AE in Hong Kong. In addition, a modified promoter-PCR phenotypic assay was used to validate the genotypic tropism prediction on CRF01_AE. One hundred and five subtype B and 98 CRF01_AE antiretroviral-naive patients were recruited for this study. The viral env V3 region isolated from the patients was sequenced and analyzed by Geno2pheno (FPR=5.75% or 10%, Clonal or Clinical), position-specific scoring matrix (WebPSSM, x4r5 subtype B matrix), and the combination of 11/25 and net charge rules. Fifteen concordant and 22 discordant tropism genotyped CRF01_AE samples were further phenotyped by either enhanced sensitivity Trofile assay or an optimized promoter-PCR phenotypic assay. The prevalence of Dual/Mixed- or X4-tropic virus in antiretroviral-naive subtype CRF01_AE was 39.1%, which was significantly higher than subtype B (p<0.05), regardless of the choices of genotypic algorithms. Our phenotypic data proposed that a better genotypic tropism prediction for HIV-1 CRF01_AE would be using both Geno2pheno (FPR=10%, Clonal) and WebPSSM (x4r5 subtype B matrix) algorithms in combination. The sensitivity and specificity for this combination were 88.9% and 89.3%, respectively. The comparatively high prevalence of Dual/Mixed- or X4-tropic virus in CRF01_AE demonstrated the need for special attention to future treatment strategies.
Introduction
HIV-1
The Enhanced Sensitivity Trofile Assay (ESTA) (Monogram Biosciences, USA) is believed to be the “gold standard” for HIV tropism phenotypic determination and is available only in the United States. 4 –6 Due to its limited accessibility, other in-house phenotyping assays or genotyping assays have been developed for coreceptor prediction. 7 –10 Although the phenotyping assays provide better sensitivity and specificity, they are time consuming to process and require intensive laboratory set-up, which is definitely not suitable for clinical diagnosis. Hence the use of genotyping methods becomes the global trend for tropism prediction. Different genotypic algorithms are designed on the basis of the variable loop 3 (V3) in the HIV-1 env region, which is believed to interact with coreceptor when binding. 11 –13 The simplest prediction rule relies on the basic amino acids present at positions 11 and/or 25 of the V3 loop and the net charge of the sequences. 14 A modified prediction rule considering both 11/25 and net charge rules was proposed since it had a better prediction result for non-B subtypes. 15 In addition, Geno2Pheno [coreceptor] (G2P) and position-specific scoring matrix (WebPSSM) are two more advanced interpretation algorithms and achieved high concordance with phenotyping data in several clinical studies with HIV-1 subtype B and C isolates. These algorithms were reported to be around 80–90% specific and 50–60% sensitive for subtype B viruses and a minority of non-B subtypes. 9,12,16 –18 On the other hand, less concordance was observed in other circulating recombinant forms (CRFs) such as CRF02_AG. 19
Several genotypic studies focused on non-B subtypes suggested that subtype CRF01_AE, the major circulating strains among Southeast Asian countries, 20 had a higher proportion of X4-tropic (X4) or Dual/Mixed-tropic (D/M) than other subtypes. 21 –24 However, the small sample size and unknown treatment background led to many uncertainties in these studies. In addition, no phenotypic data on CRF01_AE tropism were available to validate any of the above-mentioned genotypic algorithms. Hence it is critical to investigate and evaluate the prevalence of X4 or D/M in antiretroviral-naive patients infected with subtype CRF01_AE.
In this study, we optimized a recently published promoter-PCR (pPCR) phenotypic assay for CRF01_AE strains and validated it with the ESTA method. 8 The phenotypic tropism assay was used to compare the genotypic predictions by three commonly used algorithms. Through the use of the genotypic tropism results, we tried to study the prevalence of tropism among subtypes B and CRF01_AE viruses circulating in Hong Kong.
Materials and Methods
Clinical samples
In 2010 and 2011, there were a total of 827 new HIV-1 infections recorded in Hong Kong. 25 About 60% of the patients sought medical consultation at the Integrated Treatment Centre (Department of Health, Hong Kong) and 203 antiretroviral-naive patients were available for this study. Baseline peripheral blood was collected from all patients during their clinic visit at the Centre after consent. An in-house genotyping assay was used to sequence the HIV-1 pol gene, which was then analyzed by the REGA Genotyping Tool version 2.0 for subtype identification. 26,27 The tropism of all samples was first estimated by genotypic tropism prediction. Based on genotyping, 15 concordant and 22 discordant CRF01_AE samples were further phenotyped by the ESTA method and/or the pPCR phenotypic assay.
Genotypic coreceptor prediction
Five hundred microliters of plasma was centrifuged at 20,000×g, 4°C for 90 min, followed by viral RNA extraction using the QIAamp Viral RNA Mini Kit according to the manufacturer's instructions (Qiagen, Hilden, Germany). The viral V3 env region was then reverse transcribed and amplified by the SuperScript III One-Step RT-PCR system with Platinum Taq High Fidelity enzyme (Invitrogen, USA) in triplicate. 3,28 The 35 amino acid V3 region was nested polymerase chain reaction (PCR) by the Expand High Fidelity PCR system (Roche Diagnostics, Germany) and cycle sequenced by BigDye Terminator v1.1 (Life Technologies, USA). The amplification and sequencing reaction conditions were described elsewhere. 29 All sequences were generated by ABI PRISM 3130xl Genetic Analyzer (Life Technologies, USA) and manually edited by Staden Package version 2.0. 30
The HIV-1 tropism was predicted by three sets of algorithms: (1) Geno2Pheno [coreceptor] 1.2 (
Phenotypic coreceptor prediction by ESTA (Monogram Biosciences)
Plasma samples of 12 HIV-1 CRF01_AE-infected patients with viral load above 2,000 copies/ml were randomly selected and sent to Monogram Biosciences in California for ESTA.
Phenotypic coreceptor prediction by a pPCR phenotypic assay
A recently published phenotypic assay was adopted in this study with slight modifications of PCR cycling conditions. 8 Briefly, the extracted RNA was reverse transcribed and amplified in triplicate reactions. An overlapping PCR technique was employed to add the CMV promoter/enhancer to the PCR products without cloning. After cotransfecting pPCR products and pNL4-3.Luc.R-E-, pseudoviruses produced were used to infect two U87 indicator cell lines expressing either the CCR5 or CXCR4 coreceptor. The luciferase activities were measured to determine coreceptor usage. Reference viruses, plasmids, and cell lines, including MJ4, LAIBRU, 89.6, pYU2, pNL4-3, pNL4-3.Luc.R-E-, U87.CD4.CCR5, and U87.CD4.CXCR4, were obtained from the AIDS Research and Reference Reagent Program (NIH, USA). MJ4 and LAIBRU viruses were used as positive controls in each batch of amplification and luciferase measurement for R5 and X4 prediction, respectively.
Statistical analyses
The viral loads and CD4 cell counts of subtype B and CRF01_AE were statically analyzed by two-tailed t-tests using GraphPad Prism (version 4.0, GraphPad software, CA). Chi-square tests were used to calculate the tropism genotypic distributions between subtype B and CRF01_AE. The sensitivity and specificity of each genotypic algorithm were calculated by converting X4 predictions to positive values and R5 predictions to negative values of the assay.
Results
Characteristics of the patients
After analyzing the pol sequence by REGA, 105 samples were confirmed to be HIV-1 subtype B while the remaining 98 samples were HIV-1 subtype CRF01_AE. The mean viral load and CD4 counts for subtype B treatment-naive patients were 4.77 log10 copies/ml (95% confidence interval: 4.66 to 4.88 log10 copies/ml) and 310 cells/μl (IQR: 163 to 446 cells/μl), respectively. For subtype CRF01_AE treatment-naive patients, their mean viral load and CD4 counts were 4.82 log10 copies/ml (95% confidence interval: 4.66 to 4.98 log10 copies/ml) and 289 cells/μl (IQR: 125–392 cells/μl). Using the t-test, both subtypes had no significant differences between their viral load (p=0.5907) and CD4 counts (p=0.2298).
V3 sequence amplification
Through triplicate PCR amplification reactions, 104 (99.0%) subtype B and 87 (88.8%) CRF01_AE were successfully sequenced and analyzed by Geno2pheno, WebPSSM, and the CR algorithms. Within the 35 amino acid V3 loop, 11 subtype B (10.5%) and 11 CRF01_AE (12.6%) samples had variable lengths of V3 loop. Most of the deletions occurred at position 24, and at other positions such as 6, 18–22, 25, and 27. Insertions were less common and could be found only at positions 15–16 and 19. The length of the V3 loop was proposed to be related to tropism. For instance, deletion of residues 9 to 12 affects tropism and the extracellular loops of the CXCR4 coreceptor interact more easily with the longer V3 loop. 34,35 Yet none of these effects was observed or had an association with the discordant genotypic coreceptor predictions as suggested. 36
Tropism genotyping by G2P, WebPSSM, and CN Rules
Either the clonal or clinical model and different FPR cut-offs were selected before inputting V3 sequences into the G2P algorithm. Of the clonal model 5.75% FPR was first selected as this is the only validated FPR with clinical studies. 31,32 “Recommendations from the European Consensus Group on the clinical management of HIV-1 tropism testing (10% FPR)” 3 was selected for the second batch of analysis. The third set of analysis used the clinical model of G2P (FPR=10%) 10,33 with the input of patient clinical parameters including viral load and CD4 and CD8 cell counts. However, the WebPSSM algorithm uses V3 amino acid sequences for prediction. All possible amino acid sequences were generated whenever a heterogeneous viral population was presented. This implied that more than one prediction would be produced with a single sequence. D/M was assigned if both CCR5 and CXCR4 coreceptor usage was predicted. The CN rules used the following criteria for X4 predictions: (1) R/K at amino acid position 11 and/or 25 in the V3 loop, (2) a net charge over+6, and (3) a net charge over+5 with R present at amino acid position 25. Table 1 summarizes all analyzed results in subtypes B and CRF01_AE as detected by G2P, PSSM, and the CN rules.
Chi-square test.
X4 includes all D/M and X4 predictions; FPR, false-positive rate.
CRF01_AE tropism phenotyping by ESTA and the pPCR assay
Twelve antiretroviral-naive CRF01_AE samples were randomly selected and sent to Monogram for phenotyping. This included seven R5 and five D/M viruses that were used to validate our modified version of the pPCR phenotypic assay. Our assay managed to reproducibly distinguish between R5 (MJ4, pYU2), X4 (LAIBRU, pNL4-3), and D/M (89.6) reference strains. More importantly, the assay results completely agreed with the coreceptor predictions by ESTA. Hence, the pPCR assay was employed to validate the genotypic tropism tests for CRF01_AE hereafter.
Based on the CRF01_AE tropism genotypic results, 15 concordant and 22 discordant predictions between each algorithm were selected arbitrarily for evaluation by the pPCR assay. The sequence alignment of these 37 samples and their coreceptor predictions by the pPCR assay, G2P, WebPSSM, and CR are shown in Fig. 1. Individual sensitivities and specificities of each genotypic algorithm against the ESTA or pPCR assay were calculated and are presented in Table 2a and 2b, respectively.
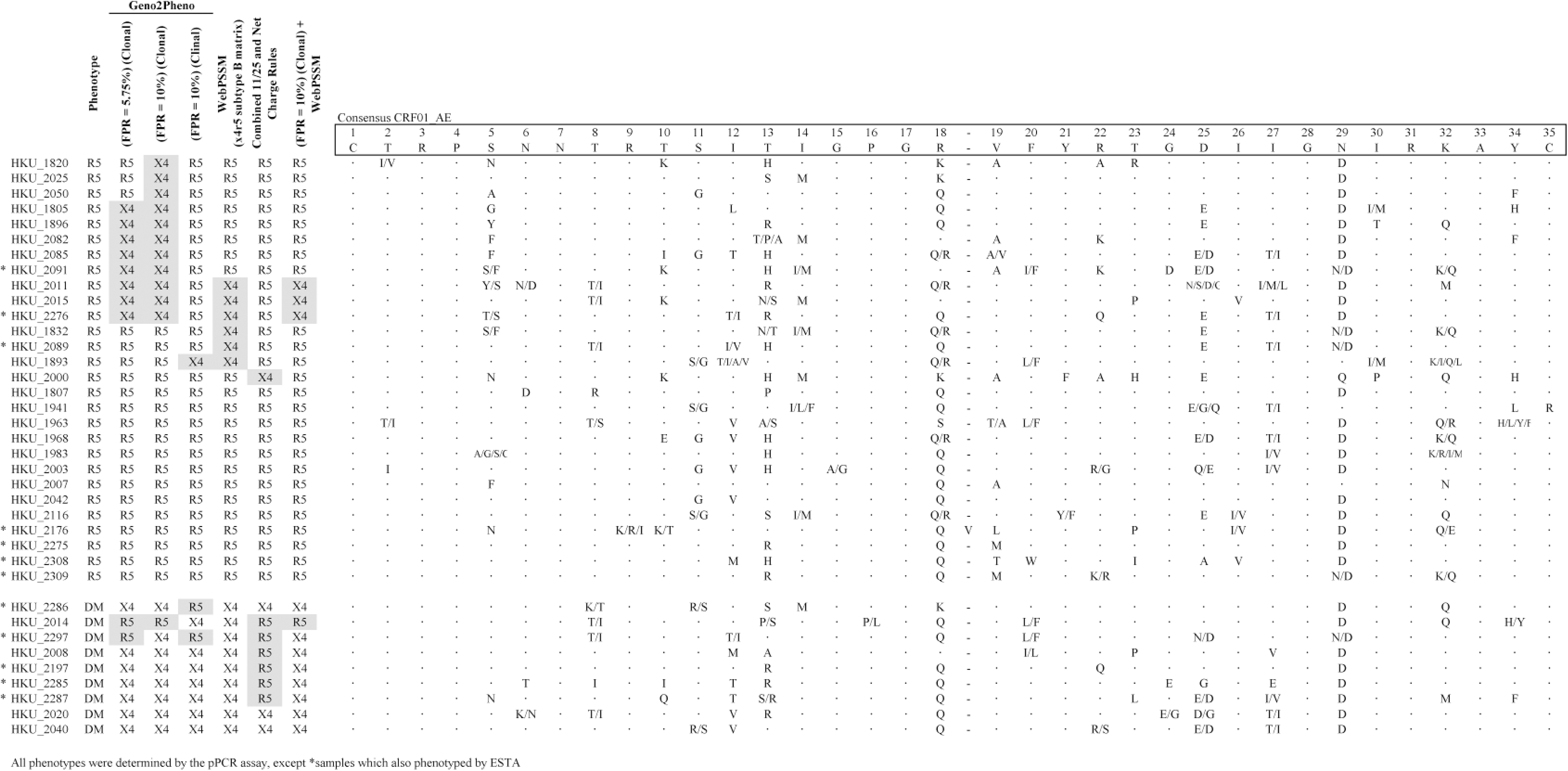
Thirty-seven antiretroviral-naive patients infected by HIV-1 CRF01_AE were phenotyped by the optimized pPCR assay. Samples marked with an asterisk (*) were also phenotyped by ESTA for validation. Their genotypic coreceptor predictions by different algorithms were compared. Discordant predictions by genotyping were shadowed. There were no distinct polymorphisms associated with the discordant data, as seen in the sequence alignment.
Proposed genotypic analysis guideline for CRF01_AE
As shown in Fig. 1, there were frequent discordant data observed between G2P and WebPSSM. Our data showed that using G2P or WebPSSM alone had overidentified X4 in some patients. This will eliminate the potential CCR5 antagonist prescription for those patients. After assessing and outweighing the sensitivities and specificities of each algorithm, we propose merging the predictions from G2P (FPR=10%, Clonal) and WebPSSM. Samples were cidentified as X4 or D/M only when both algorithms agreed with each other. The combined predictions were 88.9% sensitive and 89.3% specific. The prevalence of X4 or D/M in antiretroviral-naive CRF01_AE-infected patients was estimated to be 39.1% under these circumstances.
Discussion
To our knowledge, this is the first study focusing on the CRF01_AE tropism and the prevalence of coreceptor usage among antiretroviral-naive patients with current genotypic and phenotypic assays. The prevalence of X4 or D/M in subtype B samples is around 10–20% in many validated global studies. 14,16,37 Depending on the genotypic algorithms, a similar prevalence at 13.5–25% was observed in our locality. However, the prevalence of X4 or D/M in CRF01_AE is about 39.1% in Hong Kong, which is slightly lower than other studies at around 50%. 21,23,24 Indeed, the prevalence of X4 or D/M in CRF01_AE viruses is nearly 2-fold higher than subtype B.
In our study, over 50% of CRF01_AE samples with D/M reported by ESTA had discordant genotypic predictions by G2P and WebPSSM. Genotypic predictions were based on population sequencing and considered all possible heterogeneous viral populations, yet not all of them were really present and able to infect and replicate. More importantly, the env variable loops 1 and 2 were proposed to affect HIV-1 tropism. 38 Our pPCR assay results showed that using G2P or WebPSSM alone had a high rate of false X4 or D/M predictions for CRF01_AE samples. This implied that the prevalence of X4 or D/M among CRF01_AE viruses was not as high as reported. 21,22,24,39 The false-positive prediction would be a concern in the future for patients who have fewer salvage therapeutic options.
The patients recruited for this study were all antiretroviral-naive and had baseline samples collected at the earliest time point. A recent study showed that X4 was present in transmission clusters regardless of subtypes and routes of infection. 22 Therefore the evidence of having a high ratio of X4 transmission in CRF01_AE was promising. Some R5-tropic CRF01_AE isolates in other studies were shown to have a lower baseline susceptibility than subtype B viruses toward CCR5 antagonists. 40 Thus, an investigation of CRF01_AE viral pathogenesis will be necessary in the future due to the high prevalence of X4 observed.
In conclusion, the prevalence of X4 in CRF01_AE antiretroviral-naive patients is significantly higher than that in subtype B patients in Hong Kong. In addition, an optimized pPCR phenotypic assay, validated with the commercial ESTA method, was used to evaluate the specificities and sensitivities of common genotypic coreceptor prediction algorithms on CRF01_AE variants. Our study proposed a better coreceptor prediction for CRF01_AE strains by combining G2P (FPR=10%, Clonal) and WebPSSM (x4r5 subtype B matrix). An independent study with clinical and virological outcome data will be required to validate the proposed algorithm before implementation. The high prevalence of CXCR4 HIV-1 variants among antiretroviral-naive CRF01_AE patients suggests the need to evaluate their disease progression and pathogenesis in future studies.
Footnotes
Acknowledgments
The study was supported by the AIDS Trust Fund of Hong Kong Special Administrative Region Government (grant MSS-180R). The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
We would like to thank the Nursing Team of the Integrated Treatment Centre for their patient care and sample collection. The opinions and assertions contained herein are private views of the authors and do not necessarily reflect those of the Centre for Health Protection, Hong Kong Department of Health.
The following reagents were obtained through the AIDS Research and Reference Reagent Program, Division of AIDS, NIAID, NIH: 89.6 from Dr. Ronald Collman, LAI-1BRU from Drs. Jean-Marie Bechet and Luc Montagnier, MJ4 from Drs. Thumbi Ndung'u, Boris Renjifo, and Max Essex, pYU2 from Drs. Beatrice Hahn and George M. Shaw, pNL4-3.Luc.R-E- from Dr. Nathaniel Landau, pNL4-3 from Dr. Malcolm Martin, U87.CD4.CCR5 and U87.CD4.CXCR4 from Drs. Hong Kui Deng and Dan Littman, and AMD3100 and TAK-779 from the Division of AIDS, NIAID.
Presented in part at the 10th European Meeting on HIV and Hepatitis, Treatment Strategies and Antiviral Drug Resistance, Barcelona, March 2012.
Author Disclosure Statement
No competing financial interests exist.