
Abstract
Physiological effects of aging make the older population more susceptible to adverse drug events and drug–drug interactions. We evaluated the impact of aging and gender on the pharmacokinetics (PK) of atazanavir/ritonavir (ATV/r) 300/100 mg once daily (qd) in 22 well-suppressed HIV-infected patients. This was a 24-h intensive PK study. Subjects were HIV-1-infected adults aged ≥18 years with HIV RNA <50 copies/ml and treated with ATV/r 300/100 mg once daily plus two nucleoside reverse transcriptase inhibitors (NRTIs) for at least 2 weeks. Atazanavir and ritonavir plasma concentrations were measured by validated high-performance liquid chromatography (HPLC). Plasma PK parameters were calculated using noncompartmental methods. Since 50% of the patients were older than 42 years, age 42 was selected as the cut-off point for the older (>42 years) group. Gender, weight, duration of ATV/r therapy, and proportion treated with tenofovir disoproxil fumarate (TDF)-containing regimens did not differ between both groups. Patients from the aging group had a reduced creatinine clearance (91 versus 76 ml/min). The older group had a higher atazanavir exposure with median AUC0–24 71.2 vs. 53.1 mg·h/liter, C max 8.5 vs. 5.5 mg/liter, and C trough 1.17 vs. 0.78 mg/liter, and slower apparent clearance (3.5 vs. 4.8 liter/h). Ten patients (91%) from the older group and 36% from the younger group had ATV C trough levels higher than the proposed upper limit for toxicity of 0.85 mg/liter. Females had a lower body weight (BW) (46 versus 63 kg) than the males, but atazanavir concentrations in females were greater. However, in multivariate analysis, older age was the only significant predictor for higher atazanavir concentrations. Parameter estimate for age and atazanavir AUC after adjusting for gender and BW was 2.17 (95% CI 1.01–3.33). That is, for every year increase in age, AUC increases by approximately 2 mg·h/liter. Age seems to be an important factor influencing atazanavir pharmacokinetics. Patients from the aging group appeared to have higher atazanavir exposure compared to the younger group. Further PK explorations of ATV in the extremely aged population are warranted.
Introduction
C
In resource-limited settings (RLS), boosted protease inhibitors (PIs) are commonly prescribed as part of antiretroviral therapy (ART) after first line treatment failure. Boosted lopinavir and ritonavir is the most widely used in RLS; however, it is well-known that it results in lipid abnormalities, potentially leading to the development of cardiovascular disease. Atazanavir (ATV) has shown to be lipid friendly, has potency in suppressing HIV viruses, and can be used as a once daily regimen 3 ; its use in RLS is on the rise due in part to lopinavir-related dyslipidemia. Because the aging HIV population is increasing, few PIs have been studied in the elderly. 3 –5 The Bristol-Myers Squibb Company (BMS) product information 3 and von Hentig et al. 5 reported that age does not influence atazanavir concentrations. However, both studies were conducted in a white population.
We have previously shown that boosted atazanavir (atazanavir/ritonavir) at a standard dose recommended for white populations leads to higher plasma ATV concentrations in Thais. 6 Based on the results from this study, it was shown that age significantly affects the pharmacokinetic (PK) parameters of ATV. The older patients had a higher area under the curve (AUC0–24), maximum concentration (C max), and trough concentration (C trough). The older Asian population might be more vulnerable to high drug exposure and long-term toxicity. Here, we report the impact of age on boosted atazanavir/ritonavir 300/100 mg once daily in a Thai HIV-infected population. Although this original study was not primarily designed to evaluate the PK of atazanavir in aging HIV-infected patients, because of this surprising new discovery, we decided to reanalyze the data to assess the effects of aging on atazanavir/ritonavir PK, which may have significant implications for treating older HIV-infected patients in this region.
Materials and Methods
This was a 24-h intensive PK study of which the main study design and results have already been published. 6 In brief, subjects were HIV-1-infected adults ≥18 years of age with HIV RNA <50 copies/ml and were treated with atazanavir/ritonavir 300/100 mg once daily plus two nucleoside reverse transcriptase inhibitors (NRTIs) for at least 2 weeks.
Informed consent was obtained from each patient before entering the study. The trial was approved by the Institutional Review Board of the Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand.
Pharmacokinetic assessment
After at least 2 weeks on an atazanavir/ritonavir-based regimen, patients underwent a standardized PK assessment under steady-state conditions at predosing, 1, 2, 3, 4, 6, 8, 10, 12, and 24 h after drug intake. All meals and snacks on the pharmacokinetic study days were standardized. The plasma concentrations of atazanavir and ritonavir were measured by a validated high-performance liquid chromatography (HPLC) method. The atazanavir and ritonavir calibration curves were linear over a range of 0.045 to 30.0 mg/liter. The lower limit of quantification (LLOQ) was 0.045 mg/liter for both atazanavir and ritonavir.
Determination of pharmacokinetic parameters was based on individual plasma concentration data versus time by noncompartmental analysis. Pharmacokinetic parameters were calculated by noncompartmental methods using the WinNonlin software package (version 5.0.1; Pharsight Corporation, Mountain View, CA) with the log/linear trapezoidal rule.
On the basis of the individual plasma concentration–time data, the following pharmacokinetic parameters were determined: the area under the plasma concentration–time curve (AUC) from time zero to 24 h (AUC0–24; in milligrams·hour per liter), the maximum concentration of drug in plasma (C max; in milligrams per liter), the time to reach C max (T max; in hours), the trough concentration drug in plasma (C trough; in milligrams per liter; defined as the 24 h concentration after the observed dose), the apparent elimination half-life (t 1/2; in hours), and the apparent oral clearance (CL/F; in liters per hour).
The median and interquartile range (IQR; 25–75%) and geometric mean ratio (GMR) for AUC0–24, C max, and C trough were calculated. A multivariate linear regression model was used to assess the effect of age after adjusting for other covariates.
Results
Demographic data of the study population are shown in Table 1.
Statistical analysis was expressed in median and interquartile range (IQR).
eGFR, estimated glomerular filtration rate by modification of Diet in Renal Disease (MDRD); BMI, body mass index; TDF, tenofovir disoproxil fumarate.
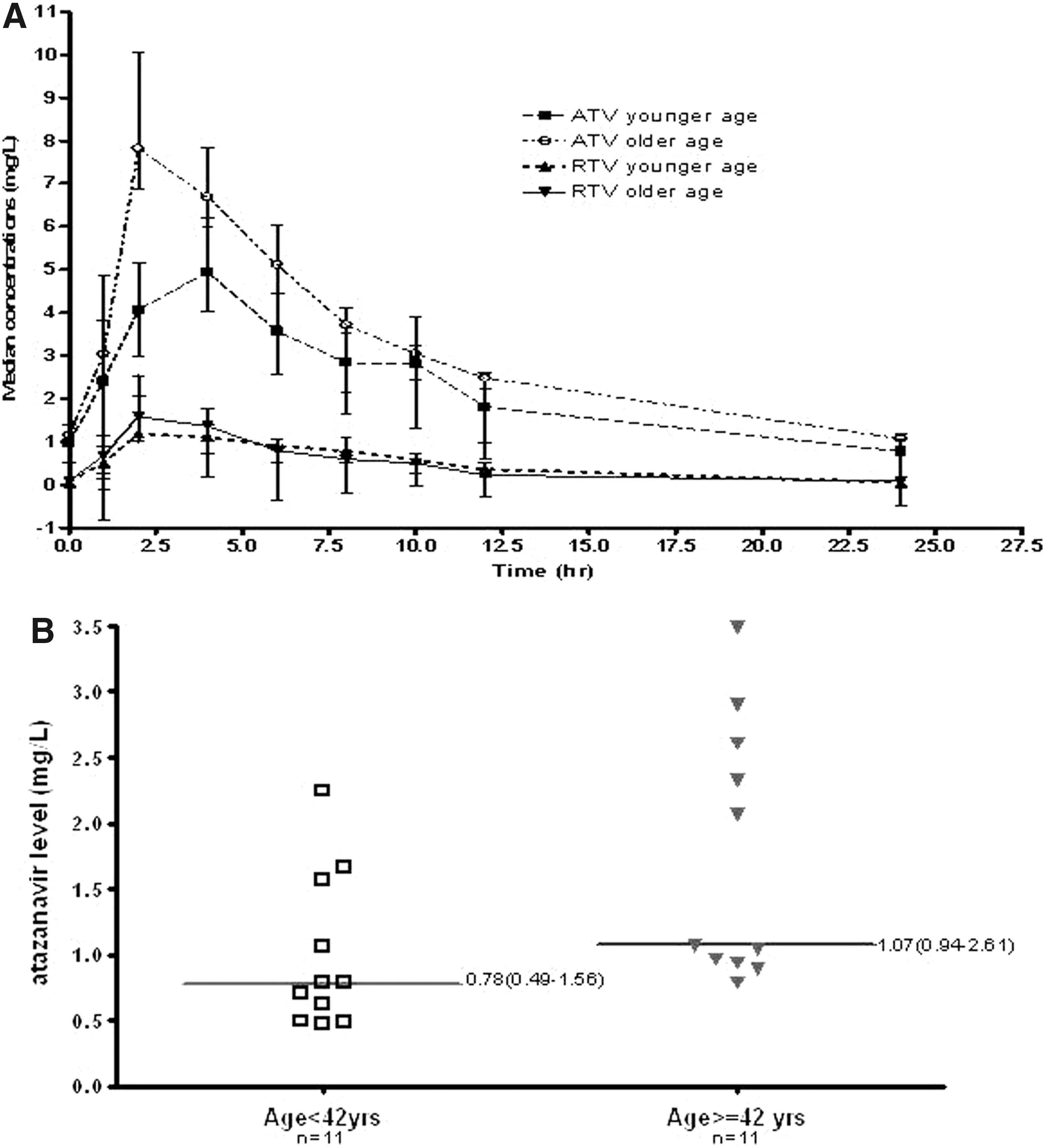
A total of 22 subjects, 11 males and 11 females, were enrolled with a median age of 41.9 years (range 28.6–57.1). Eleven (50%) patients were older than 42 years and therefore age 42 years was selected as the cut-off point for the older (≥42 years) versus the younger (<42 years) group. There were six females and five males in the younger group and five females and six males in the older (≥42 years) group. The baseline characteristics, except creatinine clearance, were similar between the older (≥42 years) and the younger (<42 years) groups. Pharmacokinetic profiles of atazanavir/ritonavir 300/100 mg are presented in Table 2 and Fig. 1.
IQR, interquartile range (25–75%); AUC0–24, area under the plasma concentration–time curve (AUC) from time zero to 24 h; C max, the maximum concentration of drug in plasma; C trough, 24 h concentration after the observed dose; T-half, the apparent elimination half-life; CL/F, the apparent oral clearance.
The older (≥42 years) group had higher atazanavir exposure with a median atazanavir AUC0–24 of 71.23 versus 53.1 mg·h/liter, C max of 8.45 versus 5.48 mg/liter, and C trough of 1.07 versus 0.78 mg/liter, and a slower apparent oral clearance compared to the younger group (5.65 versus 4.21 liter/h). The GMRs of AUC0–24, C max, and C trough between the older and younger groups were 1.51, 1.46, and 1.76, respectively. Additionally, ritonavir exposure was also higher in the older group. The AUC0–24, C max, and C trough of ritonavir between the older and younger group were 13.09 versus 11.54 mg·h/liter, 2.18 versus 1.49 mg/liter, and 0.09 versus 0.05 mg/liter, respectively. The apparent oral clearance of ritonavir was shown to be slower in the elderly group (2.29 versus 2.59 liter/h).
Ten patients (91%) from the older group and four patients (36 %) from the younger group had atazanavir C trough levels higher than the proposed upper limit for toxicity of 0.85 mg/liter. Four patients who were >50 years old had a much higher median (IQR) AUC0–24 of 88.26 (68.6–135.48) mg·h/liter, C max of 8.50 (7.13–10.8) mg/liter, and C trough of 1.84 (0.97–3.27) mg/liter. The oral clearance of patients >50 years old was much slower compared to the younger subjects [median clearance 3.53 (IQR 2.26–4.38) versus 4.77(IQR 4.02–5.78) liter/h].
Atazanavir exposure concentrations in females were greater than in males: median AUC of 70.54 versus 59.76 mg·h/liter, C trough of 1.56 versus 0.89 mg/liter, and slower clearance of 4.25 versus 5.02 liter/h. Although both age and gender seemed to be factors influencing atazanavir exposure, in a multivariate analysis, older age was the only significant predictor for higher atazanavir exposure (Fig. 2). The parameter estimate for age and atazanavir AUC after adjusting for gender and BW was 2.17 (95% CI 1.01–3.33). That is, for every year increase in age, the AUC increases by approximately 2 mg·h/liter.

Continuous scattergrams of individual age plotted against the various individual kinetic parameters of atazanavir.
Grade 3 or 4 hyperbilirubinemia (bilirubin >3.2 mg/dl) was the only short-term toxicity reported, occurring in 5/11 (45%) and 3/11 (27%) of older and younger patients, respectively (p=0.7). All patients, except one in the younger age group, had bilirubin concentrations >1 mg/dl. Unfortunately, EKGs were not performed at that time, therefore it was not able to assess prolonged QTC.
Discussion
Older individuals are more susceptible to adverse drug reactions than younger subjects such as lactic acidosis, 7 chemical hepatitis, hypertension, and hyperlipidemia. 8 In addition, higher rates of hospitalization due to adverse drug reactions in older individuals were reported. 9 Older adults may suffer from chronic disease for which multiple medications are usually prescribed. The comorbid medical conditions along with the effects of physiologic aging make the older population susceptible to adverse drug events and drug–drug interactions. Finally, aging is accompanied by marked changes in the physiology of many organs including hepatic and renal function, which, in turn, affect drug absorption, distribution, and elimination. 2 Understanding of their pharmacokinetic profiles is critical to minimize long-term toxicity, improve tolerability, and maintain long-term efficacy.
We found a positive correlation between age and pharmacokinetic profiles including AUC0–24, C max, and C trough. In our study, the cut-off was 42 years old, giving us an equal distribution of subjects (50%) between both groups. Although younger than 50 years old was used, we have demonstrated that aging, not gender, does significantly influence the PK of atazanavir/ritonavir 300/100 mg once daily. The PK profiles of atazanavir were significantly greater in patients over 42 years and even more so in those over 50 years of age, suggesting that the effect may be more pronounced in an elderly population.
Our study demonstrated that aging, not gender, significantly influenced the PK of atazanavir/ritonavir 300/100 mg once daily. The AUC0–24, C max, C trough, and half-life of both atazanavir and ritonavir were higher in patients aged over 42 years and even more in those over 50 years old, suggesting that the effect may be more pronounced in elderly patients. This could be due to the changes in the patients' body composition and CYP450 activity due to aging. 2 Atazanavir and ritonavir were primarily metabolized by an isoenzyme of hepatic cytochrome P450, CYP3A4/CYP3A5, which showed a decrease in activity with advancing age. 10 In older individuals, aging causes a 40% reduction of blood flow to the liver and a decreased liver mass, which, in turn, impact drug clearance. More importantly, it is possible that the higher exposure of ATV in older patients is a result of a higher concentration of ritonavir, which could lead to a greater inhibitory effect of ritonavir.
This information is important since it will affect HIV treatment and management among elderly HIV-infected patients. Interestingly, the influence of aging on atazanavir/ritonavir pharmacokinetics observed in our patients contrasts with a recent finding 5 that showed no clinical correlation between age and atazanavir concentrations in 26 white females [mean age 38.9 years, body weight (BW) 63.9 kg, and body mass index (BMI) 20.7 kg/m2] and 48 white males (mean age 43 years, BW 80.6 kg, and BMI 24.9 kg/m2). Additionally, a study by Dumond et al. 11 reported a decrease of atazanavir AUC0–24 and an increase of C max in six elderly subjects. However, these effects did not achieve statistical significance.
Of note, the product information for atazanavir 3 reported age as having no influence in the pharmacokinetics of the drug, but we would like to point out that single-dose unboosted atazanavir was used in healthy volunteers (18–40 years, n=29 vs. ≥65 years, n=30). It is difficult to account for this inconsistency, but it is possible that a small number of older patients included in each study, the difference of food habit, ethnicity, and pharmacogenomic factors may have played a part in the different results obtained. However, since this study was not primarily designed to evaluate PK in the elderly and based on its small sample size, it cannot be conclusively ascertained that aging has an effect on atazanavir/ritonavir concentrations.
In our study, 91% of patients from the older (≥42 years) group and 36% of the younger group had atazanavir C trough >0.85 mg/liter. Having a higher plasma concentration of atazanavir could be a potential risk for developing arrhythmia. Asymptomatic PR prolongation and atazanavir dose-dependent QT interval prolongation have been observed. 3 Ly and Ruiz. 12 reported a 59-year-old woman with congestive heart failure who developed torsades de pointes due to a prolonged QT interval from atazanavir 400 mg once daily. It could be possible that the patient's atazanavir concentration was higher due to her age, female sex, and/or drug–drug interactions. Older patients tend to have more comorbidities and therefore need to take multiple medications, which could interact with each other. This could lead to a prolonged QTc and fatal arrhythmia, especially when atazanavir exposure is high. 3 The atazanavir/ritonavir dose reduction to 200/100 mg once daily plus two NRTIs under the guidance of therapeutic drug monitoring in this special population may be an appropriate strategy. Unfortunately, we did not have EKG data to show whether our patients with high ATV concentrations are associated with prolong QTC. At this time, all patients have switched to lower dose ATV.
This study's limitation is its small sample size with inadequate numbers of persons who are truly old. HIV-infected persons who are 50 years of age and older are generally considered older adults in the literature. The study had only four persons who were 50 years old. The range of age is too small to draw a definite conclusion about the impact of aging. Nevertheless, our data have addressed an important issue of PK in aging that needs to be further explored in a much larger study of the extremely aged population.
Conclusions
Older patients appear to have a different PK profile for atazanavir in our population. The PK of atazanavir/ritonavir and other protease inhibitors in an extremely aged population should be further explored, given the potential impact on long-term efficacy and safety.
Footnotes
Acknowledgments
We are grateful to all participants and all staff of HIV-NAT, Thai Red Cross AIDS Research Centre. This study was funded by Social Security Office, Thailand Research Fund (TRF), grant number RSA 5380002, the National Research Councils of Thailand (NRCT), grant number 2553-112 and the Aligning Care and Prevention of HIV/AIDS with Government Decentralization to Achieve Coverage and Impact: ACHIEVED Project (The Global Fund Project, Thailand).
This study was partly presented as a poster (A953) at the 48th Annual ICAAC/IDSA 46th Annual meeting, October 25–28, 2008, Washington, D.C.
Author Disclosure Statement
J.A. has received educational grants, travel grants, and/or speakers' honoraria from Roche, Gilead, Abbott, and Tibotec. J.L. has received consultancy fees and honoraria from GlaxoSmithKline, Boehringer-Ingelheim, Bristol-Myers-Squibb, Hoffmann-LaRoche, Merck Sharp & Dohme, Schering-Plough, Bayer, Shire Pharmaceuticals, Agouron/Pfizer, and Virco/Tibotec. D.C. has received research grants/funding, honoraria, or lecture sponsorships from, or is a consultant or advisor to, Abbott, Boehringer-Ingelheim, Bristol-Myers-Squibb, Gilead, GlaxoSmithKline, Johnson & Johnson, Merck Sharpe & Dohme, and Pfizer. K.R. has served as a consultant for Merck and Tibotec. He has had paid speaking engagements with Bristol-Meyers Squibb, Merck, Roche, Jensen-Cilag, GlaxoSmithKline, and GPO. He has also received Senior Researcher Scholar, Thai Research Fund (TRF), the National Research University Project of CHE, and the Ratchadaphiseksomphot Endowment Fund (HR1161A).