
Abstract
Human T cell lymphotropic virus type 1 (HTLV-1) infection in Spain is rare and mainly affects immigrants from endemic regions and native Spaniards with a prior history of sexual intercourse with persons from endemic countries. Herein, we report the main clinical and virological features of cases reported in Spain. All individuals with HTLV-1 infection recorded at the national registry since 1989 were examined. Phylogenetic analysis was performed based on the long terminal repeat (LTR) region. A total of 229 HTLV-1 cases had been reported up to December 2012. The mean age was 41 years old and 61% were female. Their country of origin was Latin America in 59%, Africa in 15%, and Spain in 20%. Transmission had occurred following sexual contact in 41%, parenteral exposure in 12%, and vertically in 9%. HTLV-1-associated myelopathy/tropical spastic paraparesis (HAM/TSP) was diagnosed in 27 cases and adult T cell leukemia/lymphoma (ATLL) in 17 subjects. HTLV-1 subtype could be obtained for 45 patients; all but one belonged to the Cosmopolitan subtype a. One Nigerian pregnant woman harbored HTLV-1 subtype b. Within the Cosmopolitan subtype a, two individuals (from Bolivia and Peru, respectively) belonged to the Japanese subgroup B, another two (from Senegal and Mauritania) to the North African subgroup D, and 39 to the Transcontinental subgroup A. Of note, one divergent HTLV-1 strain from an Ethiopian branched off from all five known Cosmopolitan subtype 1a subgroups. Divergent HTLV-1 strains have been introduced and currently circulate in Spain. The relatively large proportion of symptomatic cases (19%) suggests that HTLV-1 infection is underdiagnosed in Spain.
Introduction
H
HTLV-1 is not a ubiquitous virus, being distributed throughout the world with clusters of high endemicity in southern Japan, the Caribbean basin, Romania, some regions of South America and sub-Saharan Africa, and foci in the Middle East and Oceania. 4
The main routes of HTLV-1 transmission are from infected mothers to their newborns, especially through prolonged breast-feeding, by sexual intercourse, and following transfusion of blood products contaminated with infected lymphocytes as well as sharing used needles. HTLV-1 is known to be the etiologic agent for two well-defined illnesses, a malignant T CD4+ T cell lymphoproliferation with very poor prognosis, named adult T cell leukemia/lymphoma (ATLL), and a chronic myelopathy named HTLV-1-associated myelopathy/tropical spastic paraparesis (HAM/TSP). 5 HTLV-1 infection is also associated with Strongyloides hyperinfection and disseminated disease. 6
Based on phylogenetic analyses of long terminal repeat (LTR) regions, HTLV-1 strains are classified into seven subtypes named a to g. Al least three of them (the Cosmopolitan, HTLV-1 subtype a; the Central African, HTLV-1 subtype b; and the Melanesian, HTLV-1 subtype c) have arisen from different interspecies transmission episodes from simian T cell leukemia virus type 1 (STLV-1)-infected monkeys to humans, followed by variable periods of evolution in the human host. 7 Subtype 1a, or Cosmopolitan, is distributed worldwide, 8 whereas the rest of HTLV-1 variants are restricted to specific regions. Subtypes 1 b, d, e, and g have been isolated in different regions of Central Africa. HTLV-1 subtype 1c is particularly highly divergent, and is called the Melanesian strain, as it has been isolated from natives from Papua New Guinea and Australia. The most widespread and characterized HTLV-1 subtype is the Cosmopolitan, which is further divided into five subgroups: Transcontinental (A), Japanese (B), West African (C), North African (D), and Black Peruvian (E). 9 –11
In European Western countries, HTLV-1 infection is rare and is mainly found in immigrants from endemic areas. 12 Spain is not an exception and the seroprevalence of HTLV-1 has been very low in different surveillance studies. 13,14 Moreover, all HTLV-1 strains reported to date in Spain belonged to the Cosmopolitan subtype a. 15,16 However, recent estimates have pointed out that the number of immigrants legally registered as living in Spain has increased more than 6-fold over the past 10 years. Many of the foreigners come from regions where HTLV-1 is endemic, such as some countries in Latin America and sub-Saharan Africa. The large diversity of HTLV-1 subtypes in Africa might contribute to expanding the molecular divergence of circulating HTLV-1 strains in Spain.
Herein, we summarize the main characteristics of all HTLV-1 cases recorded at the Spanish HTLV-1 national register over the past 25 years, discussing with particular attention the molecular diversity of HTLV-1 subtypes.
Materials and Methods
The Spanish HTLV-1 national register is a publicly funded database that collects information from all individuals diagnosed with HTLV-1 infection in Spain since 1989. A centralized repository of stored clinical samples, plasma and/or peripheral blood mononuclear cells, functions in parallel and was used for the current study. This study was approved by the hospital ethics committee.
All individuals positive for HTLV-1 registered were first screened using a commercial enzyme immunoassay (EIA), which incorporates antigens of HTLV-1 and HTLV-2 (Murex HTLV I+II; Abbott, Madrid, Spain) and further confirmed by Western blot (Bioblot HTLV, MP Biomedicals). Interpretation was made following the HTLV European Research Network criteria. 17 Demographic and clinical data were collected for all patients in an electronic database.
HTLV-1 subtype analysis was performed on LTR sequences by nested polymerase chain reaction (PCR) testing proviral DNA extracted from peripheral blood mononuclear cells (PBMCs). 18 Primers LTRI01 (e): TGACAATGACCATGAGCCCCAA and LTRI02 (i): CGCGGAATAGGGCTAGCGCT served as outer primers; and LTRI03 (e): GGCTTAGAGCCTCCCAGTGA and LTRI04 (i): GCCTAGGGAATAAAGGGGCG were used as inner primers. Reaction conditions were as follows: denaturation 94°C, 2 min, followed by 35 cycles (94°C, 1 min; 55°C,1 min 15 s; 72°C, 1 min 30 s), ending with 10 min at 72°C. All amplification products were electrophoresed on 1% agarose gel stained with ethidium bromide, and visualized with ultraviolet light. The LTR amplification products were purified using the QIAquick Gel Extraction kit (Qiagen QIAamp DNA miniKit, Qiagen, Hilden, Germany) and sequenced on an automated 3100 genetic analyzer (Applied Biosystems, Inc., Foster City, CA).
Sequences obtained were evaluated using phylogenetic methods. The LTR sequences (partial 538 bp) and selected references strains (including isolates from different ethnic groups and different geographic regions) were downloaded from the GenBank/EMBL database, aligned with Clustal X 19 and Dambe, 20 and manually edited using the GeneDoc program. 21 Phylogenetic trees were generated using the neighbor-joining (NJ) and maximum-likelihood (ML) methods of PAUP*, version 4.0b10. 22 The Tamura–Nei evolutionary model (which takes into account different substitution rates for transversions and transitions, as well as intersite substitution rate heterogeneity, as modeled using a γ-distribution) was selected as the best model for analysis. The NJ tree was constructed with an optimized nucleotide substitution rate matrix and a γ-shape parameter, using empirical base frequencies. The reliability of the NJ tree was assessed by analyzing 1,000 bootstrap replicates. For ML trees, a heuristic search was performed with a subtree-pruning-regrafting branch swapping algorithm using the NJ tree as the starting material, including its optimized parameters. The likelihood ratio test (RT) method was used to calculate statistical support (expressed in p values) for the branches. Trees were drawn with TreeView, version 1.4. 23
Further HTLV-1 subtyping was additionally performed using other shorter sequences that could not be included in the final analysis. A genotyping tool available at
Results
Epidemiological and clinical features
A total of 229 cases of HTLV-1 infection had been recorded in Spain through December 2012. Table 1 summarizes the most relevant clinical and demographic features of these individuals. The mean age was 41 years old and 61% were female. A total of 46 individuals (20%) were native Spaniards, with the rest immigrants from Latin America (59%) and Africa (15%). The majority of the native Spaniards had a past history of traveling to or reported sexual contacts with persons from endemic areas. The main route of transmission was sexual (41%), vertical (9%), needle exchange among intravenous drug users, or following transplantation or transfusions. However, the route was unknown for a substantial number of patients. Overall, clinical manifestations typically linked to HTLV-1 infection were recorded in 19% of cases. There were 27 patients with HAM/TSP and 17 with ATLL. Twelve of the ATLL patients have already died. Another three patients developed strongyloidasis.
HTLV-1, human T cell lymphotropic virus type 1; ATLL, adult T cell leukemia/lymphoma; HAM/TSP, HTLV-1-associated myelopathy/tropical spastic paraparesis.
Figure 1 depicts the incidence of HTLV-1 cases communicated by calendar, recording separately cases with either HAM/TSP or ATLL. The significant increase noticed during the past 5 years might reflect both the wide implementation of HTLV-1 screening in blood banks as well as the large immigration flow from endemic countries.
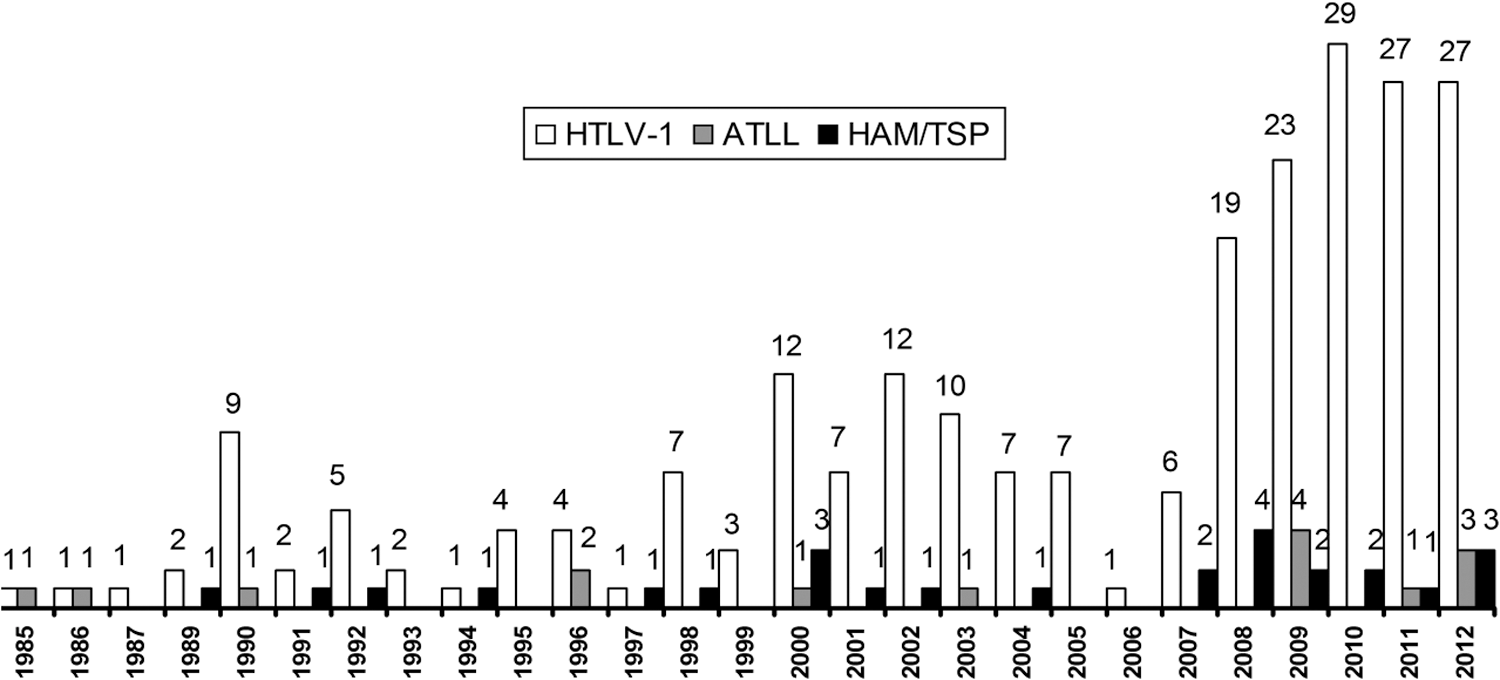
Yearly incidence of human T cell lymphotropic virus type 1 (HTLV-1) diagnosis in Spain (total and symptomatic cases).
Phylogenetic analysis
HTLV-1 subtype could be obtained from 45 individuals recorded at the national registry. Lack of PBMCs or insufficient levels of proviral HTLV-1 DNA precluded obtaining results in the remaining subjects.
Large enough LTR sequences could be obtained from 38 individuals. As shown in Fig. 2, phylogenetic analysis demonstrated that one patient belonged to HTLV-1 subtype b (patient no. 42). It corresponded to a 28-year-old pregnant woman from Nigeria who probably acquired the infection vertically; it was recommended that she bottle-feed her child. She had been living in Spain for a decade. She denied transfusions or any other significant risk behavior in the past. Fortunately, HTLV-1 proviral DNA from her infant was negative at months 3, 6, and 12 after birth.
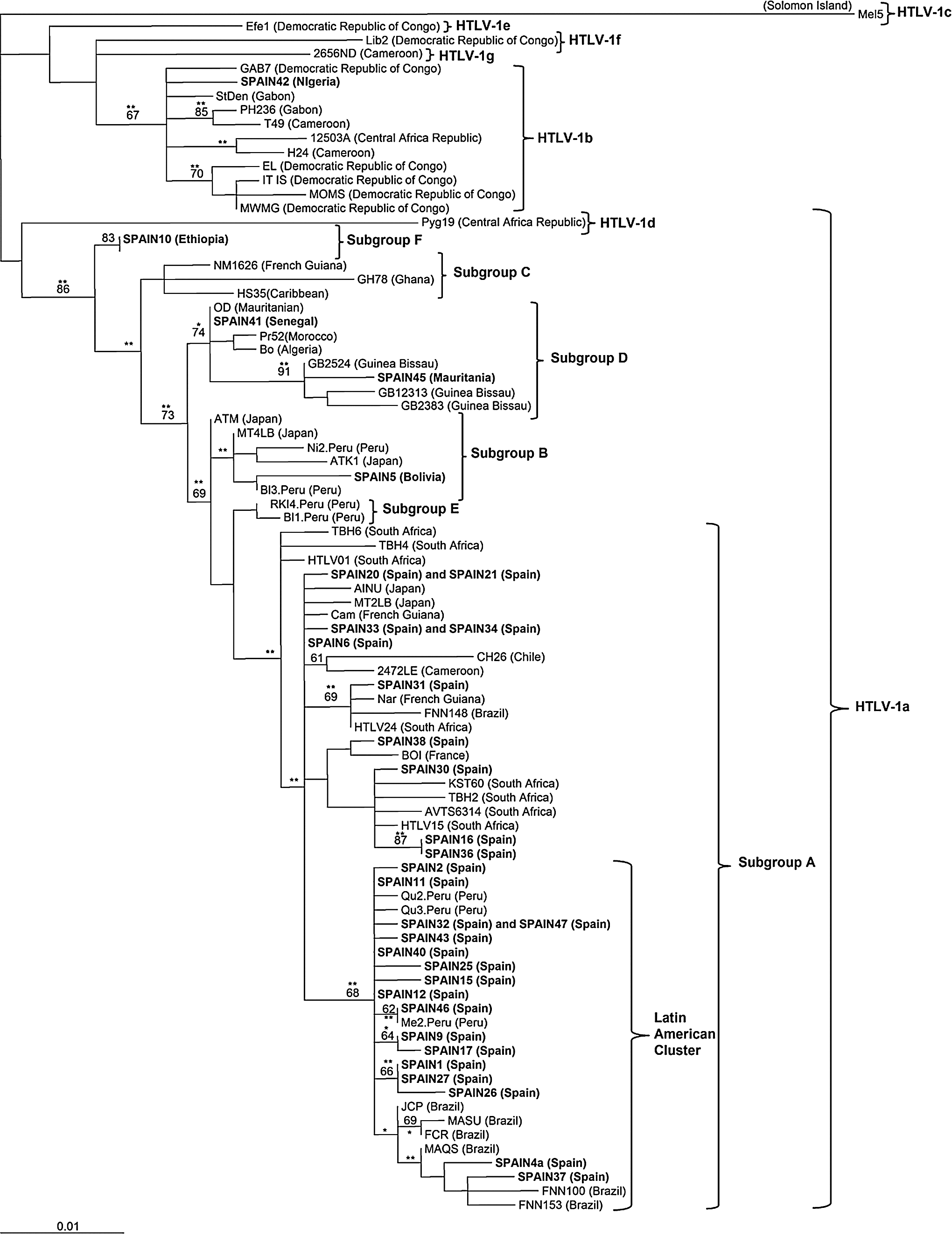
Rooted maximum-likelihood (ML) tree of HTLV-1 strains based upon a 538 bp of the long terminal repeat (LTR) region. The bootstrap values (above 60% and using 1,000 bootstrap) on the branches represent the percentage of trees for which the sequences at the right end of the branch form a monophyletic group. Mel5 was used as the outgroup. The geographic origin is given in parentheses. Newly sequenced LTRs included in this analysis are in bold. **The ML method was highly significant with a p value<0.001 or significant with a p value<0.005.
The other 37 samples examined belonged to the Cosmopolitan subtype a. Overall, 33 strains clustered within the Transcontinental subgroup A. One specimen from a carrier from Bolivia belonged to the Japanese subgroup B (patient no. 5) and the other two belonged to the North African subgroup D (patient nos. 41 and 45). These individuals had been born in Senegal and Mauritania, respectively. Another sequences (patient no. 10) branched off from all five known Cosmopolitan subgroups in a well-supported clade, and accordingly we propose a new HTLV-1a subgroup for this sample. Following the current nomenclature, it should be named subgroup F. It belonged to a 4-year-old boy from Ethiopia who had been adopted by a Spanish family. Six sequences within the Cosmopolitan subtype clustered in pairs (Fig. 2), suggesting they had a common ancestor. Two (patients nos. 33 and 34) were recipients of solid organ transplants from the same donor. 15 There was also a couple (patients nos. 20 and 21), suggesting that one infected the other through sexual intercourse. Finally, another two sequences belonged to sisters (patient nos. 32 and 47) most likely infected following vertical transmission from their mother.
Seven shorter sequences were removed from the phylogenetic analysis but were subsequently analyzed using the Bio Africa genotyping tool. Six of them were classified as subgroup A and another (patient no. 3) was ascribed to subgroup B. It belonged to a 35-year-old Peruvian male who developed ATLL. He reported that his mother had died as result of a T cell lymphoma.
It is noteworthy that the two individuals infected with an HTLV-1 Cosmopolitan subtype belonging to subgroup B (patient nos. 3 and 5) both developed ATLL (Table 2). In contrast, the subject infected with HTLV-1 subtype b (patient no. 42), the two individuals harboring subgroup D (patient nos. 41 and 45), and the subject with the new subgroup (patient no. 10) remain asymptomatic so far.
Discussion
Most HTLV-1 carriers are asymptomatic and live in highly endemic regions where rates of infection range from 3% to 6% in the Caribbean islands 25,26 to above 10% in some areas of south Japan. 27 Spain is a nonendemic region that has experienced a large immigration flow from Latin America during the past decade. As shown in the national Spanish register, the incidence of new HTLV-1 infections has increased during the past 5 years, with approximately 20 new cases reported annually. More interestingly, around 25% of cases present with typical associated diseases, namely HAM/TSP or ATLL. Thus, HTLV-1 infection should no longer be considered as an extraordinary condition in Spain, and health professionals should be prompted to consider it within the differential diagnosis of subacute neurological illnesses or acute T cell lymphoproliferative disorders. In this regard, the recent widespread policy in many autonomous communities of Spain of employing a universal HTLV-1 antibody screening test in transfusion centers must be viewed as appropriate. 28
Despite recent increases in new diagnosies, the overall prevalence of HTLV-1 infection in Spain remains low, with no evidence of rapid spreading within the general population. In recent surveys, rates of 0.01% were seen testing 20,518 pregnant women, 29 and of 0.06% testing individuals attended in hospitals for any reason. 30 However, when surveys were conducted testing immigrant populations, rates increased to 0.2% among foreign pregnant women living in Spain, coming mainly from Latin American and Africa. 29 Given the benefit of preventing vertical transmission, antenatal HTLV-1 screening is currently recommended in pregnant women from endemic regions. 31
The majority of HTLV-1 cases recorded in our national registry come from Latin America and Africa (74%), reflecting that the immigration wave from these endemic regions is the main source of HTLV-1 infection in Spain. However, up to 20% of cases were native Spaniards most of whom acquired HTLV-1 through sexual intercourse with persons from endemic areas. Thus, to some extent the virus is already circulating within the native Spanish population, suggesting that transmission and disease will not be completely halted by just checking immigrants from endemic regions. It is noteworthy that females predominated over males in our registry, most likely reflecting the more efficient sexual transmission of HTLV-1 from men to women than vice versa. 32
Typical HTLV-1-associated diseases, namely HAM/TSP and ATLL, were seen in a substantial proportion (19%) of HTLV-1 subjects recorded in the Spanish registry. Since clinical manifestations develop roughly in only 5% of HTLV-1 carriers, 33 our findings indirectly suggest that misdiagnosis is common and therefore active screening of higher risk populations is warranted.
To our knowledge we reported for the first time the presence of HTLV-1 subtype b in Spain. This variant has been reported to be endemic in Cameroon, the Central African Republic, and the Democratic Republic of Congo, being to date found exclusively in central Africa. 7,34 The individual we found to be infected with HTLV-1 subtype b came from Nigeria. We also found two individuals infected with HTLV-1 subgroup B and another two infected with subgroup D. Carriers of these variants within HTLV-1 subtype a were originally from Peru and Bolivia (subgroup B) and Mauritania and Senegal (subgroup D), respectively. Prior reports have highlighted the presence of subgroup b in Latin America, including cases from Brazil, Colombia, and Peru. 35 Likewise, subgroup D has previously been found in Africans, including subjects from Algeria and Guinea Bissau. 36 Finally, we identified a young boy from East Africa living in Spain infected with a new HTLV-1 subgroup within the Cosmopolitan subtype A, which we potentially nominated as subgroup F. To confirm this new subgroup it would be important to get more HTLV-1-infected samples from the Ethiopian population to investigate the molecular epidemiology of this virus in that region.
The fact that all uncommon HTLV-1 variants in Spain were found in subjects from Africa and Latin America suggests that the immigration flow from HTLV-1 endemic regions has created an opportunity for the virus to both spread and diversify. The introduction of new HTLV-1 variants in Spain, apart from its epidemiological interest, may have clinical consequences, as others have hypothesized that the risk of HAM/TSP might be HTLV-1 subgroup dependent. 37 This claim, however, remains controversial. Interestingly, the two individuals we found infected with subgroup B developed ATLL. Further studies examining larger HTLV-1 populations are warranted to determine the role of HTLV-1 diversity in disease development.
In summary, HTLV-1 infection should no longer be considered an exceptional infection in Spain. The large immigration flow in the past decade from highly endemic regions, mainly Latin America and Africa, accounts for the majority of cases diagnosed in recent years. Although the Transcontinental subgroup A within the Cosmopolitan subtype is the most prevalent circulating variant in persons infected with HTLV-1 living in Spain, new variants are circulating as well to a lesser extent. This is the case for HTLV-1 subtype b and for subgroups B, D, and F of HTLV-1 subtype a. To date, all these “minor” variants have been found in subjects originally from Africa and to a lesser extent from Latin America. However, with time, spreading to native Spaniards must be expected, mainly throughout sexual contact. Therefore, periodic surveillance studies, including molecular characterization of HTLV-1 strains, are warranted in Spain.
Footnotes
Acknowledgments
This work was supported by grants from Fundación Investigación y Educación en Sida (IES), RIS (Red de Investigación en SIDA, ISCIII-RETIC RD06/0006/0040 and RD/12/0017/0031), and the European NEAT project (LSHP-CT-2006-037570).
Author Disclosure Statement
No competing financial interests exist.