
Abstract
A prospective molecular epidemiology study of HIV-1 infection was conducted in newly diagnosed and antiretroviral-naive patients in Northern Greece between 2009 and 2010 using a predefined enrolling strategy. Phylogenetic trees of the pol sequences obtained in this study with reference sequences indicated that subtypes B and A1 were the most common subtypes present and accounted for 44.9% and 42.9%, respectively, followed by subtype C (3.1%), CRF02_AG (4.1%), CRF04_cpx (2.0%), and subtypes CRF01_01, F1, and G (1.0%). A high rate of clustered transmission of subtype A1-resistant strains to reverse transcriptase (RT) inhibitors was observed among men having sex with men. Indeed, 15 out of 17 study subjects (88.2%) infected with transmitted drug resistance (TDR) strains were implicated in transmission clusters, 10 of whom (66.7%) were men who have sex with men (MSM), and were also infected with subsubtype A1 strains. The main cluster within subtype A1 (I) included eight men reporting having sex with men from Thessaloniki infected with dual-class RT-resistant strains carrying both T215C and Y181C mutations.
T
In this study, we analyzed pol sequences of HIV-1 isolates from a prospective molecular epidemiology study, in which we recruited individuals newly diagnosed with HIV-1 infection from 2009 to 2010 in Northern Greece in an effort to characterize the epidemiological and genetic diversity of HIV-1 infection in the region, to determine the prevalence of transmitted drug resistance (TDR), and to gain further insight in the potential risk factors of TDR in relation to the reported risk behavior. The predefined enrollment strategy was for the most part based on the European prospective program (SPREAD) guidelines. Adult, newly diagnosed HIV-1-infected study subjects who had never been exposed to antiretroviral drugs were prospectively recruited. The blood sample was obtained within 3 months of HIV-1 seropositive diagnosis and isolated plasma was used for genotypic resistance analysis. Epidemiological, demographic, and clinical data were collected from each study subject using a standardized questionnaire.
The study subjects were consenting newly diagnosed HIV-1-seropositive patients attending the Division of Infectious Diseases of the AHEPA University Hospital in Thessaloniki, Greece between 2009 and 2010 (Table 1). A table summarizing the detailed analyses of the characteristics of the study subjects is presented in a concurrent study utilizing the same study cohort. 4 The study was approved by the Bioethics Committee of the Medical School of the Aristotle University of Thessaloniki. The HIV-1 serostatus of each subject was previously established by commercial enzyme-linked immunoassay and confirmed by Western blotting and blood was drawn within 3 months of HIV-1 diagnosis. An informed consent form was signed by each subject, a questionnaire was filled in with an interviewer, and blood samples were taken by qualified personnel. All samples and questionnaires were coded with a laboratory identifier number so as to ensure patient anonymity. Ninety-eight individuals were included in this study, representing 63.7% of antiretroviral-naive newly diagnosed HIV-1-seropositive patients registered at the database of the AIDS National Reference Laboratory of Northern Greece for the period 2009–2010.
Indicates the laboratory code for each study subject.
F, female; M, male.
Indicates the date of the sample collection.
Indicates the duration from the first known positive HIV antibody test.
Country of birth of the study subjects.
Information provided by the study subjects.
MSM, men who have sex with men; HSX, heterosexual contact; IDU, intravenous drug user, N/A, not available; ASM, asymptomatic; VZV, varicella zoster virus; HSV, herpes simplex virus; HCV, hepatitis C virus.
All blood samples were processed for population-based nucleotide sequencing of plasma HIV-1 RNA encoding regions of reverse transcriptase (RT) and protease (PR) genes at the National AIDS Reference Laboratory of Northern Greece of the Aristotle University of Thessaloniki by using commercially available kits. 5 The phylogenetic analyses were performed at the Laboratory of Biotechnology and Molecular Virology of the University of Cyprus according to previously published methodologies. 6,7 The GenBank accession numbers for the reference sequences used in the phylogenetic analyses of the pol regions are A1-DQ676872, A1-AB253429, A1-AF004885, A1-AB253421; A2-AF286238, A2-AF286237; B-K03455, B-AY331295, B-AY173951, B-AY423387; C-U52953, C-U46016, C-AY772699, C-AF067155; D-AY253311, D-U88824, D-K03454; F1-AF077336, F1-AF075703, F1-AF005494, F1-AJ249238; F2-AJ249236, F2-AJ249237, F2-AY371158, F2-AF377956; G-AF061641, G-AF084936, G-U88826, G-AY612637; H-AF190128, H-AF005496, H-AF190127; J-AF082395, J-AF082394, J-EF614151; K-AJ249235, K-AJ249239; 01AE-U54771, 01AE-AB220944; 02AG-L39106, 02AG-AY271690; 03AB-AF414006, 03AB-AF193276; 04cpx-AF119820, 04cpx-AF049337, 04cpx-AF119819. Transmitted drug resistance mutations (TDRM) were defined according to the mutation list published for surveillance of transmitted drug resistance as recommended by the World Health Organization. 8 Potential drug resistance transmission clusters were define as sequences sharing a most recent common ancestor with >85% bootstrap support and a mean genetic distance of <0.015 nucleotide substitutions per site. 9
The study group consisted of 98 HIV-1 newly diagnosed individuals. Eighty-one subjects were Greek citizens living permanently in Northern Greece at the time of the study, although a number of them reported traveling or living abroad in the past, whereas 13 subjects were born in Albania (two subjects), Cameroon, Romania, Nigeria (two subjects), South Africa, Ukraine, Russia (four subjects), and Georgia. Eighty-eight study subjects (89.8%) were male and 10 (10.2%) were female with a median age of 34 years (IQR, 27–41). The most common reported risk factor of HIV-1 transmission was homosexual contact (74.5%), followed by heterosexual contact (15.3%), intravenous drug usage (5.1%), and of unknown reason (5.1%). Investigation for other sexually transmitted diseases showed that seven of the patients were found to be positive for syphilis and one for HCV. Most of the patients were diagnosed during stage A of their infection according to CDC guidelines and at the time of diagnosis the median CD4 count and the plasma virus load were 468.5 cells/μl (IQR, 307–679.5) and 4.6 log copies/ml (IQR, 4.15–5.31), respectively. Analyses of the HIV-1 pol sequences indicated that subtypes B and A1 were the most common subtypes present and accounted for 44.9% and 42.9%, respectively, followed by subtype C (3.1%), CRF02_AG (4.1%), CRF04_cpx (2.0%), and subtypes CRF01_01, F1, and G (1.0%). The GenBank accession numbers obtained in this study for HIV-1 pol sequences are KF671758-KF671855 for protease sequences and KF671856-KF671953 for reverse transcriptase sequences.
A summary of the characteristics of patients with transmitted drug resistance mutations is shown in Table 2. The overall prevalence of transmitted drug resistance mutations (TDRM) to current HIV-1 antiretroviral drugs in the studied patients was 17.4%, of whom 29.4% were infected with viruses carrying a single TDRM. Dual-class and multiclass-resistant mutations were observed in 64.7% and 5.9% of the patients, respectively. The prevalence of nucleoside reverse-transcriptase inhibitor (NRTI) resistance was 12.24% (12 of 98 patients), the prevalence of nonnucleoside reverse transcriptase inhibitor (NNRTI) resistance was 17.35% (17 of 98 patients), and the prevalence of protease inhibitor (PI) was 1.02% (1 of 98 patients). NRTI TDRM were found in 11 patients infected with HIV-1 subtype A1 (T215C, nine patients; T215S, two patients) and in one patient with subtype C (D67N). The highest prevalent mutation was the revertant mutations at position 215 (C/S, 91.7%) followed by D67N (8.3%). NNRTI TDRM were found in all 14 patients infected with HIV-1 subtype A1 (Y181C, nine patients; K103N, five patients), two patients with subtype C subtype (Y181I), and one patient with B subtype (G190A). PI TDRM was found in a single patient (GR087) infected with subtype A1 (N88S).
Indicates the laboratory code for each study subject.
F, female; M, male.
Indicates the duration from the first known positive HIV antibody test.
Country of birth of the study subjects. N/A, not available.
Defined according to the published list of mutations for surveillance to transmitted drug resistance as recommended by the World Health Organization. 8
MSM, men who have sex with men; HSX, heterosexual contact; IDU, intravenous drug user, N/A, not available; NRTI, nucleoside reverse transcriptase inhibitor; NNRTI, nonnucleoside reverse transcriptase inhibitor; PI, protease inhibitor.
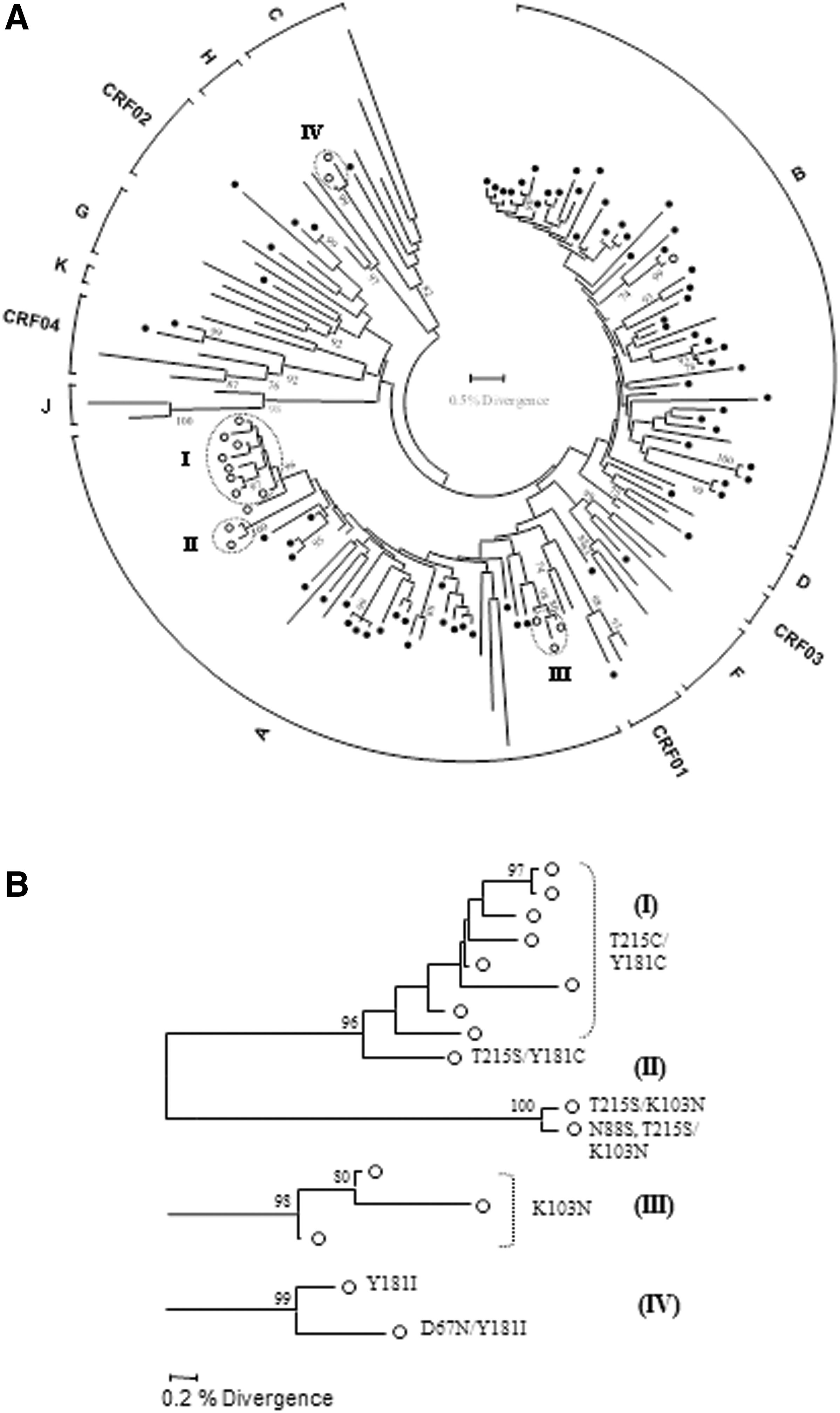
Phylogenetic analyses, presented in Fig. 1, revealed four transmission clusters highly supported by bootstrapping (>85%) and a mean genetic distance of <0.015 nucleotide substitutions per site. Three of the clusters included individuals infected with subtype A1 strains and one cluster with subtype C. The main cluster within subtype A1 (I) included eight men reporting having sex with men infected with dual-class RT-resistant strains carrying both T215C and Y181C mutations. The second subtype A1 cluster (II) involved two men who have sex with men (MSM) individuals, one with a dual-class RT-resistant strain carrying T215S and K103N and one with a triple-class-resistant strain carrying T215S, K103N, and N88S mutations. The third subtype A1 cluster (III) involved three individuals including a woman from Russia and two men from Greece, one of whom is MSM. The only subtype C cluster (IV) involved one heterosexual couple, a woman from South Africa and a man from Greece. Overall, 15 out of 17 study subjects (88.2%) infected with TDR strains were implicated in transmission clusters, 10 of whom (66.7%) were MSM and were also infected with subsubtype A1 strains.
In this study, the molecular epidemiology of HIV-1 infection and TDR in newly diagnosed patients in Northern Greece is presented. Ninety-eight newly diagnosed untreated patients, representing 63.7% of the antiretroviral-naive newly diagnosed HIV-1-seropositive patients at the database of the AIDS National Reference Laboratory of Northern Greece for the period 2009 to 2010, took part in this work, providing demographic and epidemiological characteristics as well as information on risk groups and drug use behavior. The subjects were predominantly young Greek men. The nationalities of the subjects who were not Greek demonstrate the influx of young people from Eastern Europe to the region and possibly its association with neighboring countries in the Balkans. 10
From retrospective studies carried out in Northern Greece, the main subtypes found were subtype B and subtypes A. 5,11 –13 Phylogenetic subtyping of these sequences obtained in the pol region of the HIV-1 genome confirmed the frequent presence of subtype B and A strains in this population, but subtypes C, CRF02_AG, CRF04_cpx, CRF01_01, F1, and G were also found in significantly decreased frequencies. Interestingly, 41.1% of MSM were infected with subtype A1 strains, showing that this subtype has a significant prevalence in MSM in Northern Greece, and possibly illustrating spill-over among similar risk groups in the geographic region and neighboring countries. 3,10 This would have to be confirmed by phylogenetic analysis with HIV-1 sequences from comparable risk groups from these countries and other regions in Greece. 10,14,15
The results of the study showed that within the group tested, the prevalence of TDR to current HIV-1 antiretroviral drugs was 16.32%, which is significantly higher than known prevalence rates of TDR in newly diagnosed patients in other European countries, 16 but is comparable to previously published prevalence rates of TDR in Northern Greece. 13 The phylogenetic analysis of the sequences resulted in four clusters within TDR samples, with small genetic distances (<0.015) and high bootstrap values. Two of the four clusters included MSM infected with subtype A1 TDR strains. The main cluster included eight MSM individuals, seven Greeks and one immigrant from Albania, infected with dual-class RT-resistant strains, whereas the second subtype A1 cluster included two MSM individuals, one with a dual-class RT-resistant strain and one with a triple-class-resistant strain. Interestingly, 88.2% of the patients infected with TDR strains were implicated in transmission clusters, of whom 66.7% were MSM and were also infected with subsubtype A1 strains. Although further investigation would be necessary with a more extended sampling group to obtain a more complete picture of the molecular epidemiology of HIV-1 among MSM in Northern Greece, the results obtained in this prospective study could have an impact on the development of prevention strategies for TDR for the local setting.
Footnotes
Acknowledgments
Preliminary parts of this work were presented at the 10th European Meeting on HIV and Hepatitis, Barcelona, Spain, 2012 (P_20) and the 11th European Meeting on HIV and Hepatitis, Rome, Italy, 2013 (P_16). We thank all participating subjects from the National AIDS Reference Laboratory of Northern Greece and the Division of Infectious Diseases Division of AHEPA University Hospital of Thessaloniki, the Bioethics Committee of the Medical School of the Aristotle University of Thessaloniki for valuable assistance, M. Frangiscou for preliminary statistical analysis, and A. Andoniadis for helpful discussions.
This work was supported by financial support from the University of Cyprus and University of Thessaloniki and the Birch Biomedical Research LLC, USA (3416-25017) awarded to L.G. Kostrikis and by the Hellenic Center for Disease Control and Prevention (grant 81227).
Author Disclosure Statement
No competing financial interests exist.