
Abstract
We evaluated the association of the number of late antiretroviral therapy (ART) refills with patient outcomes in a large public-sector human immunodeficiency virus treatment program in Lusaka, Zambia. Using pharmacy data routinely collected during 2004–2010, we calculated the number of late refills during the initial year of ART. We used multivariable Cox proportional hazard regression to examine the association between the number of late refills and death or program failure (i.e., death, loss to follow-up, or program withdrawal) >12 months after ART initiation, with and without stratification by the medication possession ratio (MPR) during the initial year of ART. Of 53,015 adults who received ART for ≥12 months (median follow-up duration, 86.1 months; interquartile range, 53.2–128.2 months), 26,847 (50.6%) had 0 late refills, 16,762 (31.6%) had 1, 6,505 (12.3%) had 2, and 2,901 (5.5%) had ≥3. Kaplan–Meier analysis revealed that ≥3 late refills was associated with a greater mortality risk than 1 and 2 late refills (p<0.001, by the log-rank test). The mortality risk was greater for patients with 2 late refills [adjusted hazard ratio (HR), 1.17; 95% confidence interval (CI), 0.99–1.38] or ≥3 late refills (adjusted HR, 1.51; 95% CI, 1.23–1.87), compared with that for patients with 0–1 late refills. Program failure was associated with ≥2 late refills. An MPR of <80% was associated with similar increases in mortality risk across late-refill strata. Monitoring late refills during the initial period of ART may help resource- and time-constrained clinics identify patients at risk for program failure.
Adherence is essential to the success of antiretroviral therapy (ART) for human immunodeficiency virus (HIV) infection, and poor adherence to ART promotes drug resistance, regimen failure, and ultimately death. 1 –4 ART adherence can be measured in various ways, from self-report to sophisticated monitoring of drug levels in samples of blood, body fluids, and hair. 3,5,6 Because of resource and time constraints, most ART programs in resource-limited settings rely on self-reported adherence, 3 but this metric can be inaccurate because of recall or social-desirability bias. Alternative adherence metrics that are suitable for resource-limited settings are needed.
Pharmacy adherence measures (PAMs) can objectively estimate treatment adherence, owing to their reliance on routinely collected pharmacy data, and are predictive of ART outcomes. 7 –9 The medication possession ratio (MPR) is one PAM that has become an accepted alternative to self-report. 10 The MPR measures the cumulative time that a patient has possession of antiretroviral drugs over a given interval and has been found to predict virologic suppression, mortality, and program failure among HIV-infected adults receiving antiretroviral therapy (ART) in public health clinics in Zambia. 8,11 However, the MPR can be tedious to calculate during patient visits, particularly those involving busy, overburdened facilities, and this undermines its usefulness as an adherence-monitoring tool.
In this study, we investigated a more practical PAM, the number of late ART refills during the first 12 months of treatment, as a predictor of patient outcomes. Late ART refills may be a feasible alternative to self-report that ART programs in resource-limited settings could use in routine adherence monitoring. To date, this adherence metric has not been rigorously evaluated in field settings.
We analyzed programmatic data from all adults (age, >15 years) who initiated ART across 18 public-sector sites in Lusaka, Zambia, during 2004–2010. Details of the ART program have been described in detail elsewhere. 11,12 In brief, the Zambian Ministry of Health has provided HIV care and ART free of charge since April 2004. During 2004, patients were eligible for ART if they had a CD4+ T cell count of <200 cells/mm3 or World Health Organization (WHO) stage 3 or 4 disease. From 2005 to 2010, eligibility for patients with WHO stage 3 disease also required a CD4+ T cell count of ≤350 cells/mm3. Follow-up clinical visits and pharmacy refills occur at 2 weeks, 6 weeks, and 12 weeks after ART initiation and then every 4–12 weeks for pharmacy refills, based on facility-level factors and presumed adherence levels, and every 12–24 weeks for clinical visits, based on clinical status. CD4+ T cell count is measured every 6 months, and HIV load is measured only when treatment failure is suspected.
We measured the number of late refills, defined as any ART dispensation that occurred ≥7 days after the scheduled refill date, 13 during the first 12 months of ART. Our primary outcomes were all-cause death and program failure, a composite outcome composed of death, treatment cessation, and loss to follow-up. Deaths were ascertained through family or clinic staff report, and patients who were >60 days late for a scheduled appointment on the date of administrative censoring were considered lost to follow-up. 14 Patients who interrupted treatment for >60 days but then subsequently returned to care were kept in the analysis. Because adherence patterns primarily affect long-term outcomes, we excluded patients who received ART for <12 months from the analysis.
We stratified data by the number of late refills (0–1, 2, or ≥3) and compared baseline characteristics, including age, sex, body mass index (BMI; calculated as the weight in kilograms divided by the height in meters squared), CD4+ T cell count, WHO disease stage, presence of tuberculosis, and ART regimen, using analysis of variance and χ2 analysis, as appropriate. We categorized continuous variables according to previously reported cutoffs. 11,12 We used multivariable logistic regression to identify the predictors of having ≥3 late refills and Kaplan–Meier analysis to describe the probability of death after month 12 of treatment. Multivariable Cox proportional hazard models were used to examine the association between the number of late refills and the primary outcomes. Cox models were for adjusted for age, sex, BMI, CD4+ T cell count, WHO disease stage, and ART regimen based on a priori decision or after identification of an association with the outcome at a p value of <0.05 during bivariable analyses. The proportional hazards assumption was assessed in both the unadjusted and adjusted models using the Grambsch and Therneau test. 15
To investigate the possible interaction between the number of late refills and the interval without ART, we stratified the population according to MPR over the first 12 months as part of a secondary analysis. The MPR was calculated by dividing the number of days of ART possession (based on pharmacy data) by 365 and multiplying the quotient by 100. MPRs were categorized as optimal (≥95%), suboptimal (80–94%), and poor (<80%) on the basis of previously established thresholds. 8,11 We investigated the risk of the primary outcomes, using Cox proportional hazard models as described above.
We used SAS, version 9.1 (SAS Institute, Cary, NC), for statistical analysis. A p value of <0.05 was considered indicative of a statistically significant difference. The ethics boards at the University of Zambia (Lusaka) and the University of North Carolina at Chapel Hill approved the use of programmatic data for this study.
Between 1 April 2004 and 1 February 2010, 72,492 HIV-infected adults initiated ART within Lusaka public-sector clinics. Of these, 19,477 (26.9%) were excluded from analysis because they had not been followed for at least 12 months, owing to death [6,235 patients (8.6%)], loss to follow-up [9,937 (13.7%)], or program withdrawal [3,305 (4.6%)]. Our analysis cohort thus consisted of the remaining 53,015 patients. Compared with patients who were excluded, patients included in analysis were more likely to be female (63% vs. 57%), had a higher BMI (20.1 vs. 19.0), were more likely to have WHO stage 1 or 2 disease (39% vs. 31%), had a higher CD4+ T cell count at baseline (144 vs. 123 cells/mm3), and were more likely to report having an adherence supporter (87% vs. 73%; p<0.001 for all comparisons).
In the analysis cohort, the median duration of follow-up was 86.1 months (interquartile range, 53.2–128.2 months). A total of 26,847 patients (50.6%) had 0 late refills, 16,762 (31.6%) had 1, 6,505 (12.3%) had 2, and 2,901 (5.5%) had ≥3 (maximum of 8). Across the late-refill categories, data on age, sex, BMI, baseline WHO disease stage, presence of tuberculosis, and ART regimens reached statistical significance, but were not judged to be clinically different (Supplementary Table S1; Supplementary Data are available online at
In Kaplan–Meier analyses, patients with ≥3 late refills had a higher mortality risk than patients with 2, 1, or 0 late refills (p<0.001, by the log-rank test; Fig. 1). The mortality risk appeared to decrease as the number of late refills decreased. In multivariable Cox models, patients with 2 late refills [adjusted hazard ratio (HR), 1.17; 95% CI, 0.99–1.38] or ≥3 late refills (adjusted HR, 1.51; 95% CI, 1.23–1.87) had an increased hazard of mortality, compared with patients with 0–1 late refill. Having ≥2 late refills was also associated with an increased hazard of program failure [adjusted HR, 1.46 (95% CI, 1.39–1.54) for 2 late refills and 1.51 (95% CI, 1.23–1.87) for ≥3 late refills].
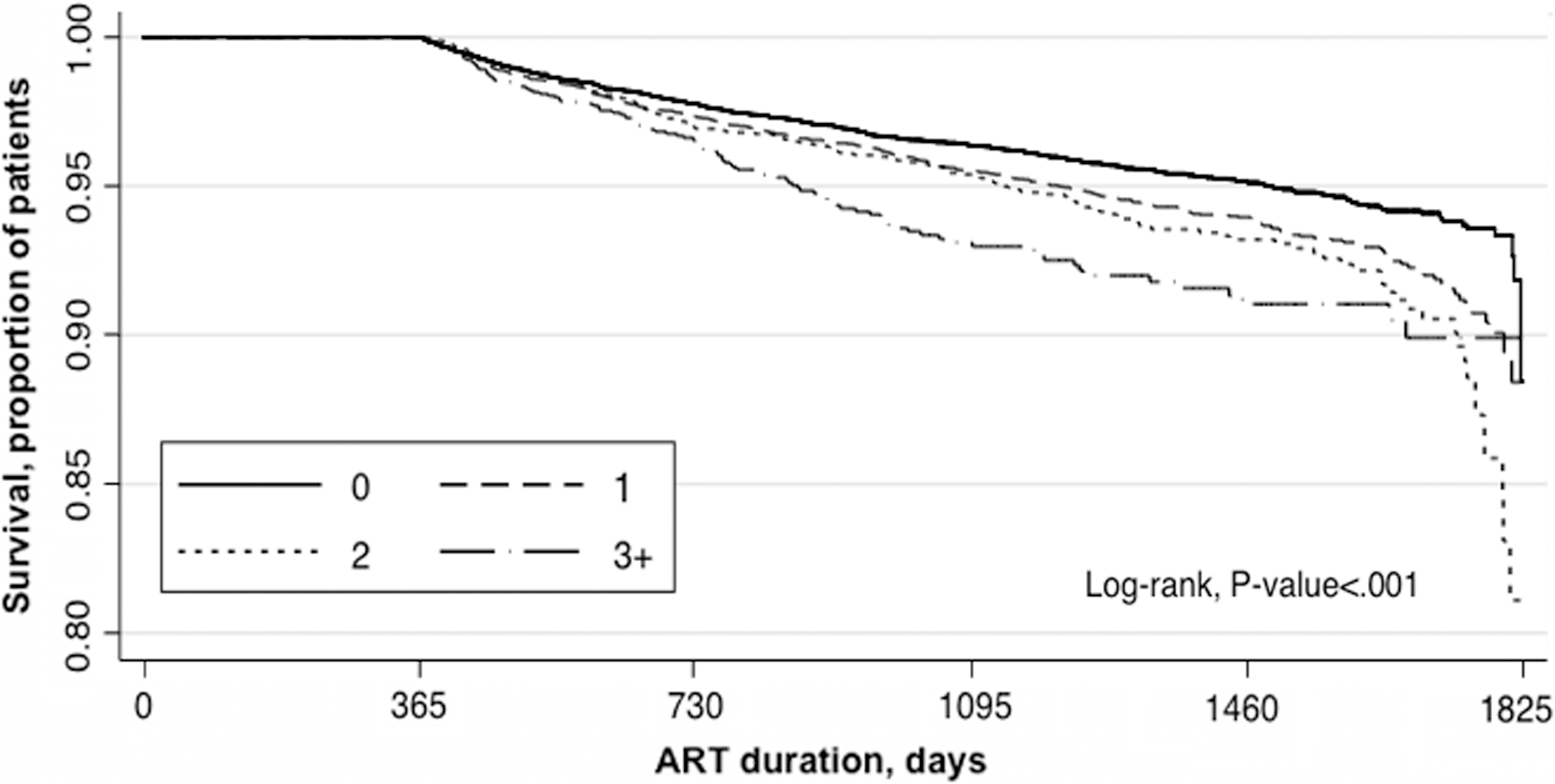
Association between the number of late refills during the first 12 months of antiretroviral therapy (ART) and subsequent mortality among 53,015 HIV-infected Zambian adults.
We further stratified this analysis by MPR during the first year of ART, with patients with 0–1 late refills and an optimal MPR constituting the reference group. Among patients with ≥1 late refill, the associated hazard of death and of program failure (Table 1) increased when the MPR was poor. Compared with the reference group, patients with 2 late refills and a poor MPR had an adjusted hazard of death of 1.81 (95% CI, 1.41–2.31) and an adjusted hazard of program failure of 2.21 (95% CI, 2.04–2.39). When MPR was suboptimal, having 2 late refills conferred a smaller but significantly increased hazard of program failure (adjusted HR, 1.41; 95% CI, 1.32–1.50) but was not associated with an increased hazard of death (adjusted HR, 1.09; 95% CI, 0.88–1.35). Similar trends in the adjusted hazard of program failure were seen among patients with ≥3 late refills.
Adjusted Hazard Ratio of Death and Program Failure During Follow-up Among 53,015 HIV-Infected Zambian Adults, by Number of Late Medication Refills and Medication Possession Ratio During the First 12 Months of Antiretroviral Therapy, 2004–2010
Defined as a pharmacy refill that took place ≥7 days after medication in the current dispensation was scheduled to run out.
Calculated by dividing the number of days of ART possession (based on pharmacy data) by 365 and multiplying the quotient by 100.
Not reported because there was only one patient in this category.
Defined as death, loss to follow-up, or program withdrawal.
HR, hazard ratio; MPR, medication possession ratio; CI, confidence interval.
Among HIV-infected Zambian adults receiving ART in a large public-sector cohort, the number of late refills during the first 12 months of therapy was associated with risks of mortality and program failure >12 months after ART initiation. Mortality and program failure risk doubled when MPR was poor, regardless of the number of late ART refills.
Monitoring late refills after ART initiation could be a widely implementable activity for measuring adherence in resource-limited settings. In a small HIV-infected cohort in Cameroon, late refills were better predictors of virologic failure than either CD4+ T cell count recovery or self-reported adherence. In addition, investigators noted that unlike other adherence measures, pharmacy data were complete in 95% of cases. 9 Whereas other PAMs have been challenging to implement in resource-limited settings because they can be tedious to measure (in the case of pill counts) and/or overly complex to calculate (in the case of the MPR), late refills could be easily tallied in a readily observable format on the medical chart summary page and/or on the patient's clinic identification card. Once a threshold of late refills is exceeded, the patient could be referred for intensive adherence interventions.
In our cohort, individuals with a poor MPR during the first year of ART had an increased risk of mortality and program failure independent of the number of late refills, compared with patients with an optimal MPR and 0–1 late refills. This suggests that although tallying the number of late refills may offer a simple adherence measure that predicts long-term outcomes, MPR might further enhance routine adherence monitoring if it could be calculated in real time. Use of electronic health records in resource-limited settings could facilitate calculation of the MPR by documenting the cumulative time that a patient does and does not possess ART.
Our finding that patients with higher CD4+ T cell counts have an increased odds of having ≥3 late refills during the first year of ART is concerning and requires further investigation. Similar findings were reported in Uganda, where researchers speculated that because relatively healthy, asymptomatic patients do not perceive that improvements in their health are due to ART, they may be less likely to overcome the structural, social, and economic barriers to adherence. 16 As a larger number of individuals with high CD4+ T cell counts receive ART under the World Health Organization's recently revised guidelines that include “test-and-treat” approaches to HIV care, 17 adherence and the consequences of poor adherence must be closely monitored.
Several key limitations to our analysis warrant discussion. Although PAMs are useful proxies of health behavior, they assume that possession of a medication is highly correlated with its ingestion. In this analysis of routine program data, we did not have access to virologic data and were therefore unable to validate late refills or MPR against viral load, which is a direct outcome of adherence. Instead we utilized a survival outcome. Some deaths may have resulted from non-AIDS events, but this should have had a nondifferential effect on our results. In addition, some deaths were likely misclassified as losses to follow-up, and for this reason we also considered program failure as an outcome. Finally, we considered only pharmacy refills during the first 12 months after ART initiation for methodological reasons, based on the assumption that early adherence behavior, an established predictor of long-term ART outcomes, 18 would mirror later adherence behavior. A systematic difference in adherence after the first 12 months of therapy among patients in certain late-refill strata could have implications for these findings.
In summary, among HIV-infected adults in Lusaka, Zambia, the number of late refills during the first 12 months of ART predicted the subsequent risk of death and program failure. In each late-refill stratum, the risks were consistently highest among patients who had a longer period without ART (i.e., a poor MPR), suggesting that tiered approaches that include PAMs might greatly enhance clinical monitoring. While PAMs hold great promise, continued research is needed to understand how best to incorporate them into routine clinical care in resource-limited settings.
Footnotes
Acknowledgments
Trainee and investigator support were provided by the National Institutes of Health through the Fogarty Global Health Fellowship (R25TW009340), the Fogarty International Clinical Research Scholars and Fellows Program (R24TW007988), and the Vanderbilt-CIDRZ AIDS International Training and Research Program (D43TW001035).
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.