
Abstract
Oral preexposure prophylaxis (PrEP) was the first biomedical intervention to demonstrate efficacy in preventing HIV infection among men who have sex with men (MSM). Healthcare providers' attitudes toward PrEP will be critical in translating this finding into effective public health rollout programs. In a convenience sample of 186 healthcare providers in Peru, we assessed knowledge, barriers, and attitudes to prescribe and monitor HIV PrEP for high-risk MSM and transgender women, the populations with the highest HIV incidence in this setting. A total of 57.5% reported awareness of PrEP, and awareness was independently associated with caring for more than 50 MSM (OR: 3.67, p<0.002). Lack of local guidelines, concern about increased high-risk behavior, antiretroviral drug resistance, and limited availability of antiretrovirals for HIV-infected individuals were the most common barriers to prescribing PrEP. Of all physicians 44.6% indicated that they would be likely to prescribe oral PrEP now; likelihood to prescribe was higher if PrEP were supported by local guidelines (70.3%, p<0.001), if more trials supported its effectiveness (68.5%, p<0.001), and if intermittent use were shown to be effective (62.2%, p=0.019). Physicians were more likely to prescribe PrEP now if they care for more than 50 MSM (OR: 6.62, p=0.010). Infectious disease specialists were less likely to prescribe PrEP (OR: 0.10, p=0.003) than nonspecialists. Successful large-scale implementation of PrEP in Peru will require focused educational campaigns to increase awareness and address concerns among healthcare providers.
Introduction
HIV-1
In late 2010, the landmark proof-of-concept iPrEx trial was the first biomedical intervention shown to be efficacious in preventing HIV infection among MSM and TGW. The study demonstrated 44% efficacy in preventing HIV infection using daily oral co-formulated emtricitabine/tenofovir disoproxyl fumarate (FTC/TDF) as preexposure prophylaxis (PrEP). 9 Self-reported compliance was high (≥89% at week 4), but plasma drug concentration collected in a subset of participants suggested that actual adherence was probably lower. Adherence was low in some sites outside the United States (U.S.), raising many questions about applicability to diverse populations, the critical importance of adherence counseling and monitoring, optimal dosing intervals, and method of delivery. 10 Whereas different studies among MSM and TGW are either planned or in progress to assess these questions, 11 –16 other studies are trying to translate positive PrEP findings into programmatic priorities to address the need to identify and implement innovative evidence-based HIV prevention strategies. 17 –26
In addition to advocacy from populations at risk and governmental support of public health rollout programs, two critical aspects of a successful prevention program include a high-risk population willing to use such a method and providers willing to prescribe and monitor it. Given the magnitude of the HIV epidemic in Peru, MSM and TGW would benefit from access to PrEP. Although awareness of PrEP has been low among MSM and TGW, there is general enthusiasm about and interest in this HIV prevention method both in Peru and in other settings. 27 –30 Healthcare providers who are knowledgeable about PrEP and are comfortable prescribing it are also going to be a critical component of a successful PrEP implementation program since they would serve as a source of information for individuals at risk, provide counseling and testing, and be ready to ensure monitoring of potential side effects. 31
Literature about provider attitudes toward PrEP and willingness to prescribe PrEP is limited and pertains primarily to U.S.-based physicians. Recent data demonstrated that the majority of Massachusetts providers would be willing to prescribe PrEP if further studies show high efficacy and no evidence of risk compensation, drug toxicity, or development of antiretroviral resistance among users. 32 However, not much is known as to whether similar attitudes are prevalent among providers in developing settings, including Peru; reports are limited to qualitative studies with only a small number of providers. 33 In Peru, co-formulated FTC/TDF (marketed as Truvada) is not yet available for treatment of HIV, and its use for prevention is still far off. This presents a window of opportunity to examine provider attitudes and address potential barriers to prescribing Truvada for PrEP in anticipation of its availability and subsequent approval.
A one-time survey was administered to assess healthcare providers' attitudes toward oral PrEP for MSM and TGW at highest risk of HIV acquisition. In addition, we aimed to describe the concerns and barriers that would prevent healthcare practitioners from discussing or prescribing PrEP to these high-risk populations.
Materials and Methods
Participants and procedures
From March 2012 through July 2012, a convenience sample of 186 providers was recruited in Lima, Peru from a variety of sources: attendees of a national conference on HIV (69.9% of responders); healthcare institutions and organizations (30.1%), including IMPACTA and VIA LIBRE (HIV research non-governmental organizations—NGOs), EPICENTRO (a community-based organization for MSM), hospitals of the Ministry of Health and social security system, and urban sexually transmitted infection (STI) healthcare centers. Responders included healthcare providers and professionals with diverse experience working with individuals at risk for or living with HIV. A self-administered 40-question paper-based survey and an informed consent form (in Spanish) were distributed.
Eligibility criteria included age ≥18 years and working in a healthcare setting with patients with or at risk for HIV in Lima, Peru. Overall, approximately 700 surveys were distributed and 186 were completed for a response rate of 27%. No financial compensation was given for completing the survey.
The survey collected data on demographic characteristics (age, gender, occupation, level of training), type of practice, and number of MSM and HIV-positive patients cared for, as well as experience in prescribing antiretroviral treatment (ART), conducting HIV and STI testing, ART adherence counseling, and/or risk-reduction counseling as a part of their current job.
To assess awareness of oral PrEP, participants were asked: “Have you heard of PREEXPOSURE PROPHYLAXIS, which is the use of oral antiretrovirals taken BEFORE a high-risk exposure for the prevention of HIV acquisition?” In addition, physicians were asked whether they have ever prescribed PrEP to prevent HIV acquisition in MSM or TGW.
To evaluate potential barriers to prescribing PrEP, physicians were asked to rate on a scale from 0 (of little concern) to 10 (of extreme concern) how concerned they were about 10 issues such as access to medication, need for daily dosing, drug resistance, and risk behavior. Median score and interquartile range (IQR) were calculated for each barrier and then ranked.
Five questions were asked about the likelihood to prescribe PrEP now and under certain hypothetical situations: if the Ministry of Health of Peru approved guidelines for its use, if Truvada (FTC/TDF) or TDF alone had an indication for HIV prevention, if results of more clinical studies demonstrated efficacy for HIV prevention, and if it were shown that intermittent dosing before and after a high-risk sexual exposure is effective for the prevention of HIV. Likelihood to prescribe oral PrEP was assessed on a Likert scale from 0 (extremely unlikely) to 10 (extremely likely). Responses were dichotomized for analysis so that a response of 8 or higher was considered “likely to prescribe” and a response below 8 was considered “not likely to prescribe.” This cutoff was employed as it was used in similar studies on PrEP attitudes 34 and was considered a conservative estimate of a physician's likelihood to prescribe PrEP.
All participants provided written informed consent before participation. The study protocol and informed consent form were approved by both the Asociación Civil Impacta Salud y Educación and Columbia University Medical Center Institutional Review Boards in compliance with all applicable Peru and U.S. federal regulations governing the protection of human participants.
Statistical analysis
Responses were entered into an electronic database. Mann–Whitney U test and Chi-square or Fisher's exact tests were used to assess associations between variables. In the analysis evaluating factors associated with barriers to and likelihood of prescribing PrEP, only responses from physicians were used. To determine independent factors associated with provider awareness of or likelihood to prescribe PrEP in different scenarios, multivariable logistic regression analyses were conducted using backward stepwise elimination with the Wald test, including in the preliminary models only those variables that were significant at the p<0.20 level in the univariate analysis as well as responses on each of the potential barriers to prescribing PrEP. Multivariable analyses yielded odds ratio (OR) and 95% confidence intervals (CI). Friedman's test was used to determine if there were differences among various concerns rated by physicians. McNemar's test was used to assess differences between the likelihood of prescribing PrEP now versus prescribing PrEP under different hypothetical scenarios. All the above analyses were conducted using Statistical Package for the Social Sciences version 19.0 (SPSS Inc., Chicago, IL). All tests were two-sided and statistical significant associations were defined as p<0.05.
Results
The majority of participants were younger than 40 years old (51.1%), female (63.4%), mixed race (mestizo) (90.9%), and cared for fewer than 50 MSM (56.5%) and 50 HIV-positive (59.1%) patients (Table 1). Public hospitals were the most common place of practice (37.1%), followed by urban STI healthcare centers (17.7%) and NGOs (16.7%). Physicians constituted the greatest number of responders (40.3%), followed by nurses, midwives, and psychologists/counselors. Among physicians, slightly less than one-third were specialists in infectious diseases (ID), while the majority (68.0%) were general practitioners, internal medicine physicians, or physicians of another specialty. Those physicians who had at least 50 HIV patients in their practice were mostly ID specialists (69.6%).
Includes generalists, residents in training, and specialists.
Includes biologists, pharmacists, dentists, medical students, technicians, and other clinic research staff.
Among all physicians.
Question had more than one option.
Data are no. (%) of subjects with characteristic. Total denominators varied slightly because of missing data.
Awareness of PrEP among all healthcare providers
A substantial proportion (57.5%) of healthcare providers had heard of oral PrEP (Table 2). Providers whose principal role was to prescribe ART, compared to others, were more likely to be aware of oral PrEP (81.3% vs. 53.7%, p=0.005). Providers caring for at least 50 MSM were more likely to be aware of PrEP than providers with fewer MSM in their practice (80.4% vs. 49.0%, p<0.001); similarly, providers caring for at least 50 HIV-positive patients were more likely to be aware of oral PrEP than their counterparts caring for fewer HIV infected patients (77.1% vs. 50.9%, p=0.003). Furthermore, ID physicians were more likely to have heard of oral PrEP than others physicians (83.3% vs. 54.9%, p=0.021).
p-value calculated by comparing those practicing in public hospitals to those practicing in other institutions.
p-values are calculated for the difference between levels of each variable: e.g., between female and male providers.
PrEP, preexposure prophylaxis; MSM, men who have sex with men; ID, infectious disease.
In multivariable analysis, only caring for more than 50 MSM patients remained independently associated with awareness of oral PrEP (OR: 3.67, 95% CI: 1.63–8.27, p<0.002).
Barriers to prescribing PrEP among physicians
There were statistically significant differences in how physicians ranked their concerns about PrEP (p<0.001). The most common concerns about prescribing PrEP included the lack of formal Peru Ministry of Health guidelines regarding its use (median=9.0, IQR: 7.0–10.0), concern about increased high-risk behavior (median=8.0, IQR: 6.0–10.0), limited availability of antiretrovirals for people infected with HIV (median=8.0, IQR: 6.0–10.0), and risk of inducing antiretroviral drug resistance (median=8.0, IQR: 5.0–9.0) (Fig. 1). ID and non-ID physicians expressed similar concerns regarding prescribing PrEP, with the exception of the concern about inexperience managing antiretrovirals, which was higher among non-ID physicians (median=7.0, IQR: 5.5–9.0) than ID physicians (median=5.0, IQR: .75–8.0; p=0.017).
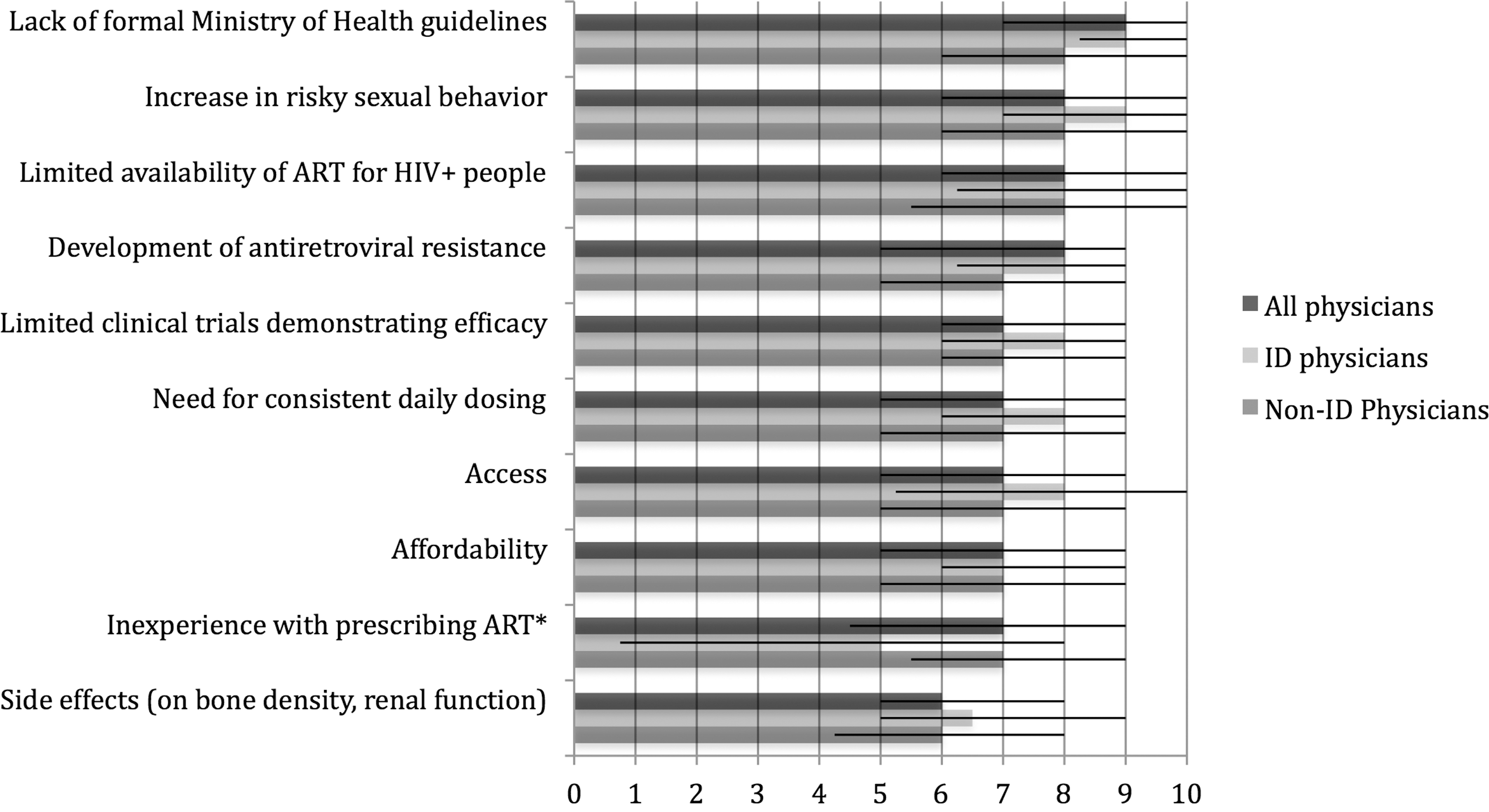
Concerns about prescribing oral preexposure prophylaxis (PrEP) by physicians in Lima, Peru. Seventy-five physicians were asked to rate on a scale (from 0 to 10) how concerned they were about the following potential barriers when considering prescribing PrEP. A median score was calculated for each category of concern. Shown are the median score (with IQR) for all physicians and infectious disease (ID) and non-ID physicians. *ID and non-ID physicians expressed similar concerns regarding prescribing PrEP, with the exception that ID physicians were less concerned about inexperience with prescribing antiretrovirals (ART) (p=0.017).
Likelihood of prescribing PrEP among physicians
Among the physicians who completed the survey, likelihood to prescribe oral PrEP at the time this survey was conducted was 44.6%. There was no difference in the likelihood to prescribe PrEP now than if Truvada (FTC/TDF) or TDF alone had an indication for the prevention of HIV acquisition (47.3%, p=0.832); however, likelihood to prescribe increased if PrEP for HIV prevention were supported by Peru Ministry of Health guidelines (70.3%, p<0.001), if more clinical trials supported its effectiveness (68.5%, p<0.001), and if intermittent use were shown to be effective (62.2%, p=0.019).
Likelihood to prescribe oral PrEP either now or under hypothetical scenarios differed with physician specialty and patient population. For example, likelihood to prescribe it now was lower among ID compared to non-ID specialists (29.2% vs. 52.0%, p=0.083). If Truvada (FTC/TDF) or TDF alone had an indication for HIV prevention and if more clinical trials supported its effectiveness, physicians caring for more than 50 HIV-positive patients would be more likely to prescribe PrEP compared to providers with fewer patients (69.6% vs. 37.0%, p=0.020 and 86.4% vs. 60.9%, p=0.049, respectively).
In multivariable analysis, ID compared to non-ID specialists were less likely to prescribe PrEP now (OR: 0.098, 95% CI: 0.02–0.45, p=0.003), while physicians with at least 50 MSM patients under their care had a higher likelihood of prescribing PrEP (OR: 6.62, 95% CI: 1.58–27.80, p=0.010). These differences disappeared under hypothetical situations that demonstrated support for the efficacy of PrEP or if external sources (such as the Ministry of Health) provided support for its use.
Interestingly, prescribers who indicated a high level of concern about the need for daily dosing were more likely to prescribe PrEP now (OR: 1.31, 95% CI: 1.02–1.67, p=0.036) if Truvada (FTC/TDF) or TDF alone had an indication for HIV prevention (OR: 1.38, 95% CI: 1.01–1.89, p=0.045), and if it were supported by guidelines from the Ministry of Health (OR: 1.31, 95% CI: 1.01–1.70, p=0.041). In multivariable analysis, increasing concerns for other barriers were also associated with the likelihood of prescribing PrEP under certain hypothetical scenarios (Table 3).
Expressed concerns for prescribing PrEP measured by asking physicians to rate on a scale from 0 to 10.
Men who have sex with men.
Antiretroviral treatment.
Peru Ministry of Health.
All variables remaining in the final multivariate regression models are reported. No adjustment was conducted to build these models.
Of note, only three physicians stated that they had previously prescribed PrEP to MSM or TGW, but no information on the antiretroviral PrEP regimen was obtained.
Discussion
To our knowledge, this is the first study to provide quantitative data about providers' awareness, attitudes, and experience regarding oral PrEP in a developing country. Among 186 Peruvian healthcare professionals, close to half of whom were physicians, awareness of oral PrEP was high at over 50%, but only a minority of physicians indicated a willingness to prescribe it at the time the survey was administered.
Awareness of PrEP was nearly 4-fold higher among healthcare providers with a larger MSM practice. This is not surprising, considering that MSM in Peru are a high-risk population for HIV infection, and healthcare providers caring for them are more likely to be aware of new HIV prevention methods that are targeted for this community. In particular, they may be more familiar with the iPrEx study and its scientific community education efforts conducted in the city (36% of the entire sample size of the iPrEx study was enrolled in Lima 9 ).
Interestingly, although awareness of PrEP was higher among ID compared to non-ID specialists, likelihood to prescribe at the time the study was conducted was lower among specialists. This may be because ID physicians, who often see sicker HIV-positive patients and have more experience prescribing ART, are more concerned about adherence and long-term side effects of PrEP. These issues may make them less willing to use antiretrovirals freely in HIV-negative patients, compared to generalists who may desire to take advantage of this additional opportunity to prevent HIV infection in their patients. Moreover, those who cared for a significant number of MSM patients were almost 7-fold more likely to prescribe PrEP, and potentially saw it as an important new tool to prevent the spread of HIV in this heavily affected community.
For those who were likely to prescribe PrEP now or under hypothetical scenarios (if there were an indication for Truvada as PrEP, or if there were formal guidelines from the Ministry of Health), there was high concern about the need for daily use. Although mathematical modeling suggests that it may be sufficient to take oral PrEP two or three times a week with the same efficacy, 35 evidence from clinical studies to date suggests that oral PrEP will work only with daily adherence. Physicians who are willing to prescribe PrEP understand the importance of daily dosing, which will be critical to emphasize when counseling patients about adherence to this intervention.
Previous qualitative studies conducted among a small number of providers in Peru reported that the most important and commonly mentioned barriers were access to PrEP among high-risk groups, cost-effectiveness, adherence, and side effects. 33 Our data, in contrast, demonstrate that the greatest concerns to prescribing oral PrEP were lack of formal guidelines from the Peruvian Ministry of Health, limited availability of antiretrovirals for those already infected with HIV, increase in risky sexual behavior, and development of drug resistance. Potential side effects were of least concern to our responders. Surveys conducted among U.S. and Canadian providers reported a similar level of concern about the development of ART resistance, but much less concern about risk compensation than noted in our study. 32,36,37 In fact, one survey among New York City providers showed that risk compensation and limited availability of antiretrovirals for HIV-positive patients were of least concern among a list of 11 potential barriers to prescribing PrEP. 37
As a developing country with an increasing prevalence of HIV, Peru has only a limited amount of antiretrovirals for HIV-positive individuals, let alone HIV-negative individuals; thus, Peruvian providers may be less likely to prescribe relatively scarce drugs to at-risk patients. However, certain hypothetical scenarios, such as the introduction of normative guidelines or more data supporting the efficacy of PrEP, appeared to increase the likelihood of prescribing oral PrEP among all physicians. For example, if the Ministry of Health provided guidelines for use of PrEP, 70.3% of physicians would be likely to prescribe it. Support from the Ministry of Health could help alleviate concerns about the lack of availability of antiretrovirals for HIV-infected patients since physicians may feel they are getting approval from the government that PrEP is a cost-effective use of limited resources. In addition, formal guidelines about regular HIV testing, risk reduction counseling, and monitoring around PrEP could help address ways to reduce the development of drug resistance and minimize risk compensation, as has been done in the U.S. 38 Differences between ID and non-ID specialists' willingness to prescribe PrEP disappeared under our hypothetical scenarios, suggesting that ID specialists may be waiting for more guidelines and clinical data about optimal dosing around high-risk exposure before prescribing it.
A few other countries' governments have already provided interim guidelines for the use of oral PrEP. In mid-July 2012, the U.S. Food and Drug Administration (U.S. FDA) approved Truvada (FTC/TDF) for oral PrEP, 39 and the World Health Organization (WHO), 40 the U.S. Centers for Disease Control and Prevention (U.S. CDC), 38 the British Association for Sexual Health and HIV (BASHH), 41 as well as the South African HIV Clinicians Society (SA-HIV Society) 42 have all published interim guidelines recommending FTC/TDF-based PrEP as a useful strategy to enhance the effectiveness of a comprehensive HIV prevention strategy among populations at risk. Truvada is not yet available commercially in Peru, but will be available in early 2014. So far, the Peruvian government has not issued guidelines regarding the use of PrEP among high-risk populations, although limited data suggest that Peruvian national policymakers may support the introduction of PrEP among individuals at risk for HIV infection. 33 Furthermore, other data show that a strategic PrEP intervention that is rapidly scaled and targets groups at highest risk (MSM and TGW) could be a cost-effective intervention in Peru. 26 When Truvada becomes available, the Ministry of Health will likely recommend its use in treatment, but not prevention. However, our study suggests that official Peru Ministry of Health support of PrEP would lead to an increase in PrEP prescribing practices.
One important note is that the U.S. FDA approved Truvada toward the end of our study. Only six participants (including two physicians) took our survey shortly after the FDA's approval. However, the information about new guidelines and indications from the U.S. FDA are likely to take longer to reach providers in Peru and are thus less likely to affect their opinions right away. These respondents were more likely influenced by data from iPrEx, which recruited heavily from Peru and demonstrated that daily adherence of FTC/TDF was effective in MSM. Even so, our data suggest that FTC/TDF having an indication for HIV prevention would not increase the likelihood that physicians would prescribe PrEP.
One major limitation of our study is that we used a convenience sample, where most of those surveyed came to attend a national HIV conference and were more likely to be motivated to learn about new discoveries in the literature, and thus be better informed about HIV prevention methods. In addition, our response rate of 27% was low and included only 75 physicians. Those who were most interested in PrEP may have been more likely to respond, creating a selection bias. Furthermore, some healthcare providers in our study may have been involved in the iPrEx study since it heavily recruited from Lima. While we did not specifically ask respondents if they worked at an iPrEx site, only three physicians had stated that they had previously prescribed PrEP to MSM or TGW; thus, up to three physicians may have been directly involved in iPrEx. While this number is small (4.0% of all physicians surveyed), these factors together limit the generalizability of results to other healthcare professionals in Peru, and our sample may have overestimated the proportion of people who were aware of and prescribed PrEP. Another major limitation is that participants responded only to what they would likely do now and in certain hypothetical situations, not what they actually did. Answers to our survey questions may serve as only a weak proxy for what providers would do in real-life situations when faced with patients at high risk for HIV infection.
Our results highlight the importance of effective educational campaigns that will be needed to increase awareness and address concerns of PrEP among providers and healthcare professionals. Prior to a successful large-scale implementation of PrEP to prevent the transmission of HIV in Peru, healthcare providers must be knowledgeable about PrEP, be willing to counsel their at-risk patients about it, and prescribe and monitor its use over time. Our study suggests that more clinical trials and approval by the Peruvian government may increase physicians' willingness to prescribe PrEP. Only then will PrEP contribute to an effective comprehensive HIV preventive strategy that will be necessary to achieve incremental reductions in the incidence of HIV among high-risk MSM and TGW living in Peru.
Footnotes
Acknowledgments
The authors would like to acknowledge all of the participants as well as the Asociación Civil Impacta Salud y Educación (IMPACTA) staff without whom this study would not have been possible. This work was supported by a grant from the Doris Duke Charitable Foundation to Columbia University College of Physicians and Surgeons to fund International Clinical Research Fellow, Eric C. Tang and by unrestricted discretionary core funds from IMPACTA. The funding sources played no role in the study design, data collection, data analysis, data interpretation, writing of the manuscript, or the decision to submit the article for publication.
Author Disclosure Statement
No conflicts of interest are reported.