
Abstract
The prevalence of HIV drug resistance varies with geographic location, year, and treatment exposure. This study generated yearly estimates of nonnucleoside reverse transcriptase inhibitor (NNRTI) resistance in treatment-naive (TN) and treatment-experienced (TE) patients in the United States (US), Europe (EU), and Canada. Studies reporting NNRTI resistance identified in electronic databases and 11 conferences were analyzed in three groups: (1) TN patients in one of four geographic regions [US, Canada, EU countries with larger surveillance networks (“EU1”), and EU countries with fewer data (“EU2”)]; (2) TE patients from any region; and (3) TN patients failing NNRTI-based treatments in clinical trials. Analysis data included 158 unique studies from 22 countries representing 84 cohorts of TN patients, 21 cohorts of TE patients, and 8 trials reporting resistance at failure. From 1995 to 2000, resistance prevalence in TN patients increased in US and EU1 from 3.1% to 7.5% and 0.8% to 3.6%, respectively. Resistance in both regions stabilized in 2006 onward. Little resistance was identified in EU2 before 2000, and increased from 2006 (5.0%) to 2010 (13.7%). One TN Canadian study was identified and reported resistance of 8.1% in 2006. Half of TN clinical trial patients had resistance after treatment failure at weeks 48–144. Resistance in TE patients increased from 1998 (10.1%) to 2001 (44.0%), then decreased after 2004. Trends in NNRTI resistance among TN patients show an increased burden in the US and some EU countries compared to others. These findings signify a need for alternate first-line treatments in some regions.
Introduction
A
Many international guidelines recommend the first-generation NNRTI, efavirenz (EFV), as the preferred NNRTI-based treatment for first-line treatment. 2 –4 EFV was introduced in 1998 and is considered the gold standard for patients beginning therapy. Although the number of approved ARVs has increased in recent years, the number of available regimens to any given patient remains limited. This is due in part to cross-resistance, which can preclude use of treatments within the same class. Resistance can be transmitted or arise after virologic failure. For example, the two mutations most frequently selected by EFV, K103N and Y188L, also confer resistance to the other first-generation NNRTI, nevirapine (NVP), whereas second-generation NNRTIs available since 2008 may still remain active. 5 One concern is that transmitted NNRTI resistance observed among treatment-naive patients can be relatively persistent, with the potential to become endemic. 6
NNRTI resistance has been found to vary by geographic location, patient observation year, and exposure to treatment. 7,8 Given the importance of optimal selection of initial treatment regimens fully effective against patients' viral strains, understanding population-wide resistance prevalence can guide health policy makers by informing treatment recommendations and help clinicians prescribe treatments most likely to suppress viral replication. Therefore, the objective of this study was to understand the overall prevalence and recent trends of NNRTI resistance in European countries, the United States, and Canada.
Materials and Methods
Systematic search
A systematic literature review was conducted in EMBASE and PubMed to identify relevant citations containing estimates of the prevalence of NNRTI drug resistance. Database search terms included the following: [“HIV-1” (MeSH) OR “human immunodeficiency virus 1” (tiab)] AND [“reverse transcriptase inhibitor” (all fields) OR “reverse transcriptase inhibitors” (all fields)] AND [“nonnucleoside” (all fields) OR “nonnucleoside” (all fields) OR “NNRTI” (all fields)] AND [“resistance” (all fields) OR “resistant” (all fields)]. The search was restricted to studies with abstracts published between 2002 and July 2012 in English. Manual searching of references of systematic reviews and meta-analyses identified from the searches was also conducted to find additional relevant articles.
To identify more recent studies not yet published, we also searched abstracts presented at 11 research conferences (International HIV Drug Resistance Workshop, International HIV & Hepatitis Drug Resistance Workshop & Curative Strategies, Conference on Retroviruses and Opportunistic Infections, Annual Conference of the British HIV Association, IAS Conference on HIV Pathogenesis, Treatment and Prevention, International AIDS Conference, International Conference on Human Retroviruses: HTLV and Related Viruses, International Congress on Drug Therapy in HIV Infection, Infectious Disease Society of America, International Symposium on HIV & Emerging Infectious Diseases, and International Conference on Antimicrobial Agents and Infectious Diseases). Conference proceedings from 2009 to July 2012 were searched using text-based methods with the following search strings: “resistan,” “NNRTI,” “nonnucleoside,” “nonnucleoside,” “EFV,” “efavirenz.” These words were selected to correspond to the database search terms.
Study selection
Inclusion criteria consisted of clinical trials or observational cohort studies with explicit mention of patient type (treatment-naive, treatment-experienced, or treatment-failing type) and reporting total number of patients and total number with NNRTI resistance, defined as the presence of any NNRTI mutation according to algorithm used in the study. Patient population of included studies was restricted to patients from a European country, United States, Canada, or multicenter international randomized clinical trials (RCTs). Studies were excluded that did not report resistance specific to the NNRTI class, reported prevalence of individual point mutations, and/or reported prevalence proportions without total number of patients sampled.
Titles and abstracts of each record identified from the search process were independently assessed by two researchers for further review. Selected full-text articles were also independently assessed for potential data extraction by two researchers using the aforementioned criteria. Inconsistencies were resolved by consensus. Manual searching of references of published systematic reviews and meta-analyses was also conducted to identify additional studies. Conference abstracts were searched by one reviewer for potential relevance. A second reviewer made the final selection for potential study inclusion. Authors of selected conference abstracts were contacted to request associated posters/presentations, if contact information could be obtained. Posters and full-text articles obtained directly from the authors were then evaluated for inclusion into the study.
Data extraction
Variables including country of data collection, year of sample, sample size, and number of patients with NNRTI resistance were extracted from all relevant studies into a structured Microsoft Access database designed for this study. Relevant data from each study were extracted by three reviewers, and results were compared to ensure accuracy.
Data analysis
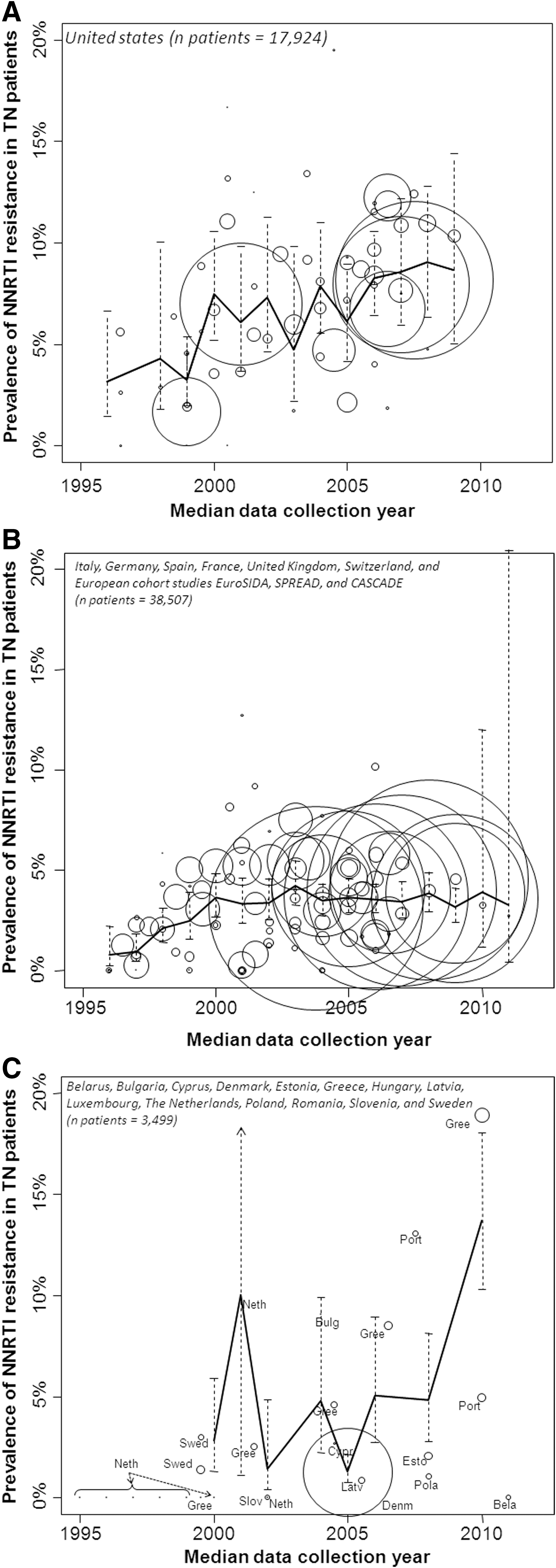
Analyses were stratified by patient type and geographic location: (1) treatment-naive patients in European countries with well-developed surveillance programs and large cohort studies providing data with larger sample sizes (“EU1”; Italy, Germany, Spain, France, United Kingdom, and the EuroSIDA, SPREAD, CASCADE, and Swiss HIV cohort studies); (2) treatment-naive patients in other European countries providing data from two or fewer studies (“EU2”; Belarus, Bulgaria, Cyprus, Denmark, Estonia, Greece, Hungary, Latvia, Luxembourg, The Netherlands, Poland, Romania, Slovenia, and Sweden) (Table 1); (3) treatment-naive patients in the United States; (4) treatment-naive patients in Canada; (5) treatment-experienced patients from any region; and (6) treatment-naive patients failing NNRTI treatments in randomized clinical trials.
Stratified resistance data were visualized using scatter plots of the reported resistance prevalence versus data collection year. The median year of data collection was used for studies reporting resistance measured over multiple years. For purposes of quantitative meta-analyses, median years ending in “0.5” (from a collection period of 2000–2001, for example) were rounded to the nearest even year.
Generalized linear mixed models (GLMMs) with the logit link function were used to generate a random effects estimate of overall resistance prevalence for each year in the United States and EU1 treatment-naive analyses and the treatment-experienced analysis. A random effects model has two components of variation: (1) random variation across the different studies due to differences in sampling methods, patient population, etc. and (2) the random variation resulting from the collection of the data from year to year. These two sources of variation are commonly known as between-study variability and within-study variability, respectively. The model of within-study variability was developed because several studies report data over multiple time periods and year-to-year variability and inherent correlation among multiple observations within the same study needed to be captured within the statistical model.
EU2 data were insufficient for a GLMM, and a generalized linear model (GLM) with the logit link function was used instead. The distinction between the GLMM and GLM is analogous to the distinction between the fixed-effect and random-effects model. The use of the GLM model is reasonable if no or few studies include data over multiple years and there is no need to account for within-study correlations.
GLMM/GLM analyses generated overall estimates and 95% confidence intervals (CIs) of the proportion of patients with NNRTI resistance by year for the treatment-naive and treatment-experienced strata. Overall resistance in patients failing treatment in RCTs was determined using the weighted average of the reported prevalence estimates; 95% CIs were generated using the pooled variance.
Results
Systematic search results
Study search results are shown in Fig. 1. Conference screening using EMBASE and keyword searches identified 149 abstracts, of which 77 were selected for potential inclusion and authors of 58 were contacted successfully by e-mail, from whom some full conference presentations were obtained. Forty-six abstracts or presentations were selected for extraction after which four were later excluded due to insufficient data, resulting in a total of 17 conference posters/presentations and 25 abstracts in the analysis. Full-text database searching identified 1,287 hits from which 170 full-text articles were evaluated for potential inclusion. These articles included 14 references identified from supplementary searching or received from authors of conference abstracts and 8 systematic reviews, which were screened for relevant references. Ultimately, 143 full-text articles and 42 conference posters were extracted for potential inclusion in the study (Table 2).

Published article and conference abstract literature search results.
NNRTI, nonnucleoside reverse transcriptase inhibitor.
Several articles reported data from the same cohort of patients. Each extracted study was reviewed to identify like patient cohorts among the different articles. Twenty-seven articles and/or abstracts were found to contain duplicate data (duplicate patient cohorts and study collection years); thus, 158 records remained for inclusion into the meta-analyses. Six of these studies were excluded because the patient type could not be identified 9 or for reporting prevalence of resistance in a mixed population of treatment-naive and treatment-experienced patients. 10 –14
Among studies of treatment-naive patients, those reporting resistance to specific second-generation NNRTIs (rilpivirine, etravirine, or lersivirine) 15 –19 were excluded from the quantitative analysis, but reported separately. Studies reporting resistance identified by ultrasensitive sequencing methods, 20,21 or not reporting year of data collection, 22 –28 were also excluded, leaving 93 studies 8,14,26,29 –118 included in the treatment-naive meta-analysis. These 93 studies represented 84 patient cohorts from 22 countries reporting data from 1992 to 2011. The majority of studies included patients from EU1 countries (35 cohorts) and the US (33 cohorts), with two studies presenting data from both regions. Seventeen cohorts were from EU2 countries and one cohort was from Canada. The overall treatment-naive analysis consisted of data from 60,645 patient samples.
Five studies of treatment-experienced patients were excluded for reporting resistance specific to the second-generation NNRTI, etravirine (results reported separately). 18,119 –122 An additional 10 were excluded for not reporting years of data collection, 55,123 –131 leaving 23 studies 14,58,59,94,132 –150 representing 21 patient cohorts from nine countries reporting data from 1996 to 2010 for the quantitative analysis. These data included 12 EU1 cohorts, 5 US cohorts, 3 EU2 cohorts, and 1 Canadian cohort totaling 41,666 patient samples.
Of the 17 randomized controlled trials (RCTs) reporting resistance at time of treatment failure, nine were not included into the quantitative analyses due to not reporting the total number of patients failing treatment, 151,152 trial not conducted in treatment-naive patients, 153,154 both, 140,155 –157 or not reporting the time point of assessment. 56 The remaining eight studies 158 –165 included 613 treatment-naive patients failing treatment by weeks 48, 96, or 144 of the trials.
First-generation NNRTI resistance
Overall prevalence estimates by year and geographic region are shown in Fig. 2 superimposed onto scatter plots of the reported data. NNRTI resistance was more prevalent in treatment-naive US patients than treatment-naive EU1 patients for nearly all observation years. From 1995 to 2000, the prevalence of TN-associated resistance increased in US and EU1 from 3.1% to 7.5% and from 0.8% to 3.6%, respectively. The estimated mean prevalence was more stable from 2006 to 2009 in the US (range: 8.3–9.1%) and from 2006 to 2011 in EU1 (range: 3.2–3.9%). From 1995 to 2000, data identified from EU2 countries included a longitudinal study from the Netherlands and a Greek study, both containing samples from fewer than 25 patients and reporting 0% prevalence of resistance. TN-associated resistance in EU2 increased from 2006 (5.0%) to 2010 (13.7%), driven by data from Greece and Portugal. One Canadian cohort was identified reporting a prevalence of 8.1% in 2006, consistent with US findings.
Scatter plot of reported resistance and meta-analytic trends in
Data of reported resistance in patients previously exposed to treatment from all geographic areas were analyzed together due to the relatively small number of studies. These results showed an increasing trend from 1998 to 2001 (10.1–44.0%), followed by a decrease in resistance prevalence after 2004 (44.8–36.8% in 2009) (Fig. 3).
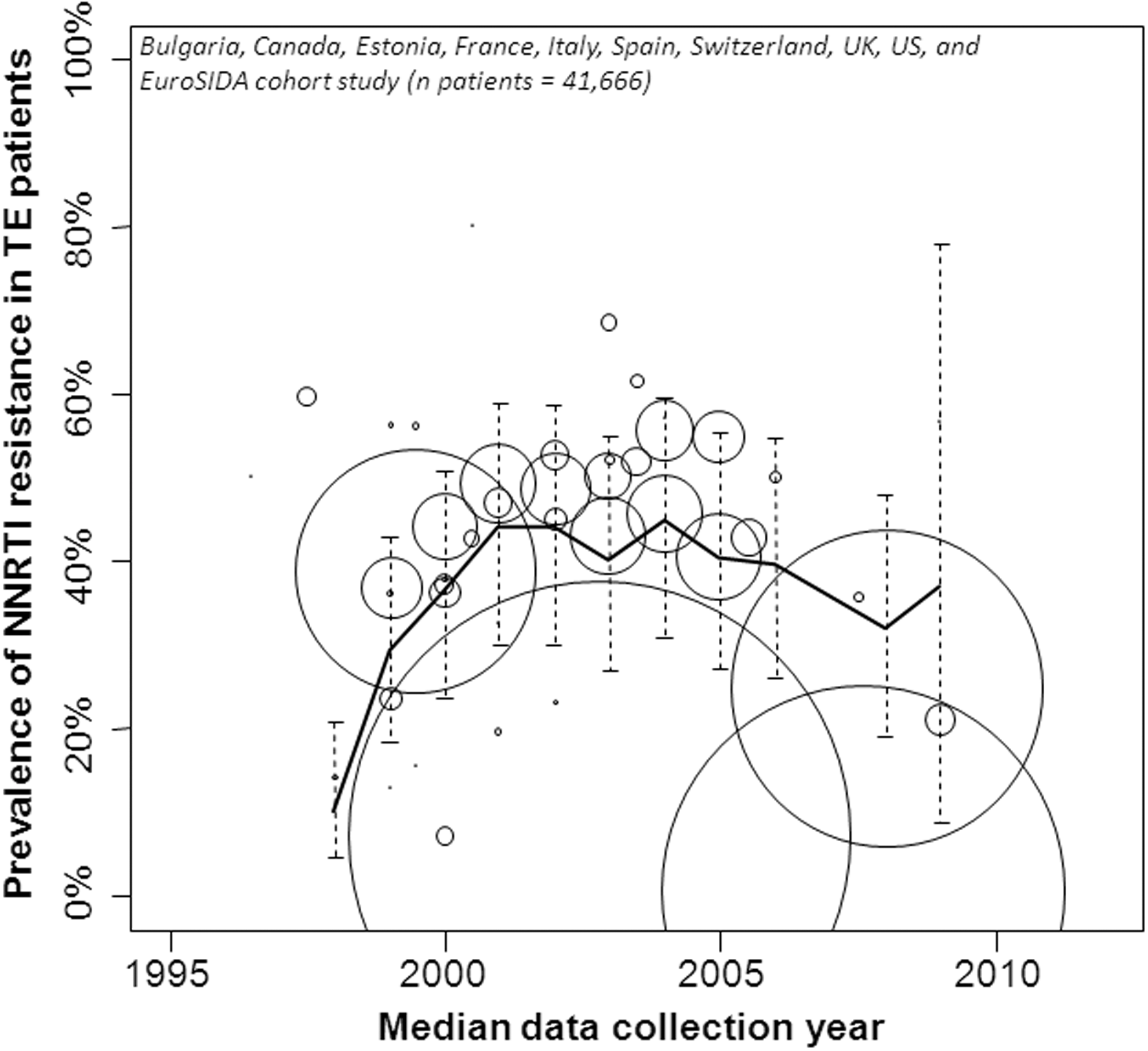
Scatter plot of reported resistance and meta-analytic trends in treatment-experienced patients. The center of each circle represents the prevalence estimate for each study and time point. The size of each circle is proportional to the study's sample size. The solid line represents the overall estimates for each year and dotted lines describe each estimate's 95% confidence interval.
Second-generation NNRTI resistance
Etravirine (ETR) resistance in treatment-naive patients was reported to be 9.5% 18 in Switzerland, 10.3% 16 in France, and 11.8% 48 in an international RCT. Rilpivirine resistance was reported to be 4.9% in France, 15 6.3% in Portugal, 17 and 20.7% in the treatment-naive screening population of a clinical trial. 19 Lersivirine resistance was reported to be 1.4% at baseline of an international clinical trial. 48
Four studies reported ETR resistance in patients exposed to or failing NNRTI treatment 18,120 –122 ranging from 22.1% to 64.9%. The overall prevalence of at least one ETR resistance mutation among those data was 53.6% [95% CI (31.5%, 75.7%)]. Studies providing these data were conducted in Switzerland (years 1999–2008), Portugal (2000–2010), Italy (up to 2010), and Spain (2000–2009). As ETR was approved in the US in early 2008 and in Europe in late 2008, it is unlikely that any of the patients in these treatment-exposed cohorts are ETR-experienced.
Eight studies reported the prevalence of NNRTI resistance after failure of EFV-based 48,159 –164,166 or rilpivirine (RPV)-based 161,162,166 treatment regimens in clinical trials. Approximately 50% of patients had resistance to these agents after failure (Fig. 4). One of these studies also examined ritonavir-boosted lopinavir (LPV/r) in combination with EFV without cotreatment with NRTIs, where approximately two-thirds of patients failing treatment by week 144 had at least one NNRTI mutation. 164
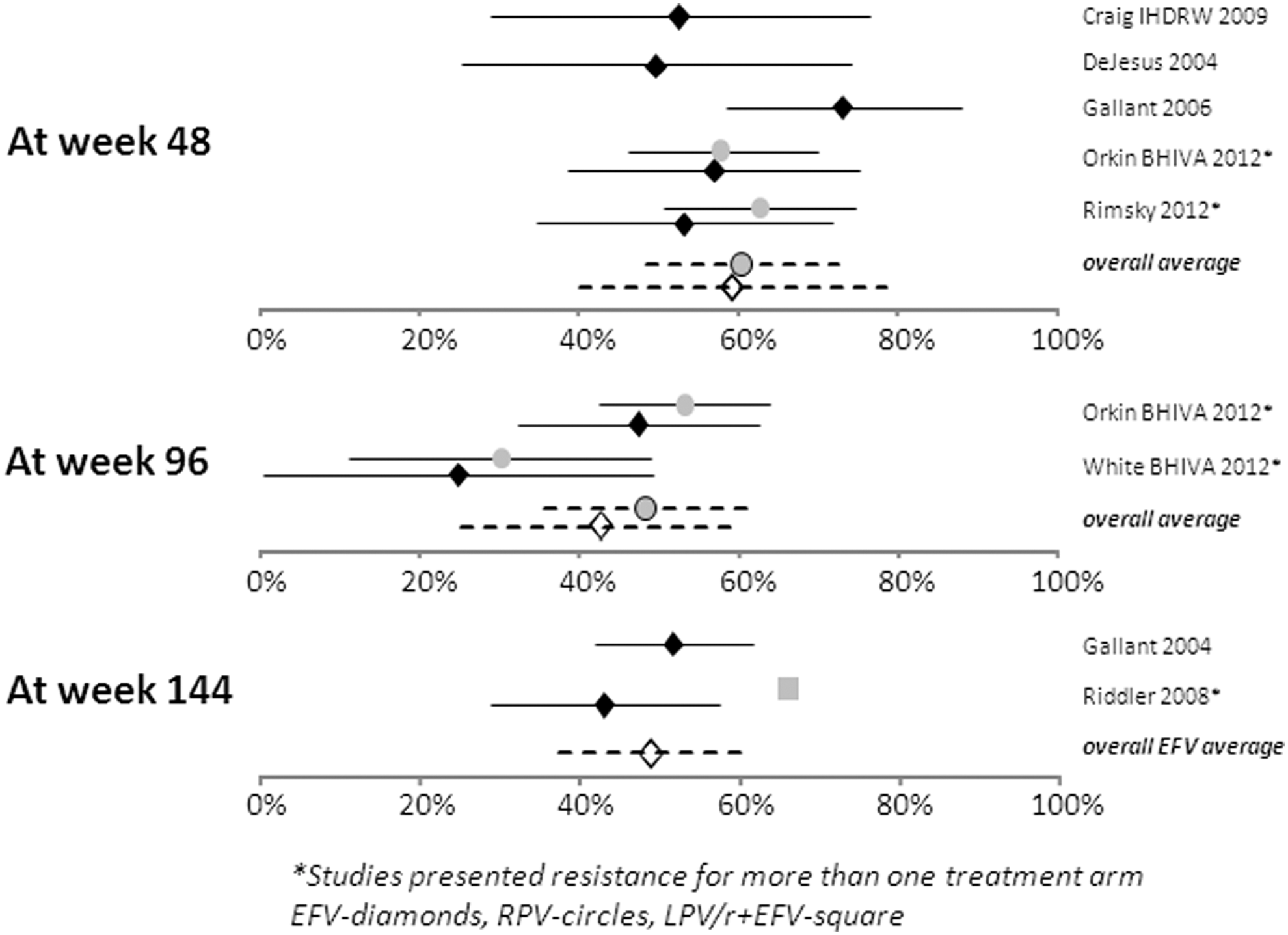
Prevalence of nonnucleoside reverse transcriptase inhibitor (NNRTI) resistance and 95% confidence intervals after failure of efavirenz (EFV)-, rilpivirine (RPV)-, and ritonavir-boosted lopinavir (LPV/r)+EFV-based first-line treatment identified from clinical trials.
Discussion
In this analysis of the published prevalence of NNRTI resistance, increased resistance was observed in the US and EU1 countries (those with larger surveillance networks and more available data) from the mid to late 1990s. This increase later stabilized in EU1 countries around 2000, but did not do so in the US until the late 2000s. Prevalence data in EU2 countries (those providing fewer data) were very limited prior to the year 2000 and studies reported very low to no levels of NNRTI resistance among treatment-naive patients. In contrast, EU2 data after the year 2000 showed a rapid and sustained increase in prevalence.
The resistance observed in treatment-naive patients will have arisen mostly through transmission either from a treated person with suboptimal viral suppression or from a person who in turn was infected by an individual with transmitted resistance. 167 However, the nature of the information reviewed here did not permit an assessment of the prevalence of transmitted resistance using designated mutations. 168 Thus, the overall prevalence of resistance transmission (or transmission of potential resistance) is likely greater than the prevalence of resistance reported here.
The reason for different trends for resistance prevalence over time among the US, EU1, and EU2 regions is complex. Different and changing availability of therapies and prescribing patterns in the populations during and prior to the period reviewed may be key factors in determining the prevalence of resistance. The stabilization of resistance in EU1 countries near the year 2000 coincides with the introduction of more potent ritonavir-boosted PIs. The data examined here primarily include surveillance periods prior to 2008 when newer second-generation NNRTIs were unavailable. The introduction of these and other novel drug classes into routine clinical practice could change future resistance trends, as has been observed previously. 169
Studies have shown that transmission of drug resistance correlates with population-level ARV utilization. 169 Thus, the more widespread use of NNRTIs in the United States compared to some European countries could have contributed to the greater prevalence of resistance and slower stabilization observed here. Furthermore, variation in NNRTI usage among European countries could also lead to differences in resistance prevalence noted between the EU1 and EU2 regions, or even unobserved differences within those regions not explored within this analysis. These factors would be best explored with patient-level data of transmitted resistance at the country level.
The goal of this research was to quantify the prevalence of transmitted NNRTI resistance over time in the geographic regions of interest. Thus, no attempt was made to identify causes or correlates of resistance, such as patient management practices, modes of transmission, surveillance infrastructure, or social attitudes, which might be contributory. Viral subtype differences have also been linked to differential transmitted drug resistance (TDR); however, some suggest this difference is better attributed to location of infection. 107,170,171 Another possible factor contributing to differential TDR prevalence is the level of population-wide virologic control in the HIV-infected populations of interest. Poor population-level viral suppression in regions of the US and the EU2 countries is a possible consideration as TDR prevalence has been shown to be linked to the proportion of HIV-infected individuals with detectable HIV RNA. 49
Data were sparse for the EU2 countries, and the analysis was limited to a small number of studies published in different countries where the patient populations and HIV treatment patterns may not be comparable. Publication bias must be considered, where the data were taken from countries in which HIV was endemic and patients in other EU2 countries were not represented. The recent increase in treatment-naive resistance in EU2 countries was driven, in part, by Greek data. In a recent publication, Skoura et al. (2013) 172 discuss the high rates of resistance among newly diagnosed patients in Greece from 2009 to 2011. The authors note that the rise in all-class TDR was driven by increases in NRTI and NNRTI resistance and that it coincided with an HIV outbreak affecting intravenous drug users and the profound Greek financial crisis, which resulted in drastic cuts in health expenditures. Other factors affecting adherence to therapy and retention to HIV care, as well as high-risk sexual behaviors, were also hypothesized to be responsible for the spread of TDR in this population.
It is interesting to note that while all-region NNRTI resistance in treatment-experienced patients decreased in recent years, no region showed a simultaneous decrease in resistance among treatment-naive patients. This observation supports the possibility of a scenario where, despite good control of the local epidemic through good antiretroviral drug use, transmission of resistance can be perpetuated by treatment-naive patients who were infected with resistant strains themselves. 6 This highlights the importance of early diagnosis and control of viral replication in these patients with fully active treatment regimens.
Reported resistance to the second-generation NNRTIs ETR and rilpivirine in treatment-naive patients was equal to or higher than the reported prevalence of first-generation NNRTIs. Additionally, reported data showed that prior exposure to NNRTIs results in a substantial prevalence of ETR resistance mutations. The data presented here include the prevalence of one or more mutations against these treatments, but it is not known whether the presence of only one mutation has the same impact on drug efficacy as is possible with a single first-generation NNRTI mutation. One study reports that at least three ETR mutations may be required to impair drug efficacy. 173,174
The results of our study are consistent with previous reports of HIV drug resistance. The study of patients screened for clinical trial participation by Rahim et al. 8 reported a higher prevalence of transmitted NNRTI resistance in North America compared to Western Europe. Frentz et al. 7 conducted a systematic review and meta-analysis of global resistance prevalence up to 2009. The authors found NNRTI resistance to be higher in North America than in Europe and an increasing time-based trend among North American studies for the year strata <2001, 2001–2003, and >2003. The corresponding NNRTI resistance trend for Europe was more stable.
Meta-analytic results in treatment-experienced patients are also consistent with a recent study identifying a decreasing trend in Western EU countries. 175 Gupta et al. (2008) 176 conducted a systematic literature review and meta-analysis of patients failing HAART treatment among clinical trials to estimate resistance to the NNRTI third agent occurred in 53% of patients after 48 weeks of follow-up, consistent with our study.
This study provides an assessment of the published literature and conference abstracts identifying reports of the prevalence of NNRTI resistance in several patient populations in 22 countries in Europe and North America. Resistance data were statistically aggregated by year of data collection to provide year-by-year trends of the prevalence of resistance in treatment-naive and treatment-experienced patients from three geographic regions, not previously found in the published literature. Understanding the magnitude and direction of TDR is important for public health officials to quantify the burden of drug resistance in the HIV population, which could call for the development of new treatment guidelines, changed patient monitoring practices, or identification of novel therapies not affected by NNRTI TDR.
Footnotes
Acknowledgments
The authors would like to thank Jing Li for statistical assistance and John A. Carter and Varun Ektare of Pharmerit International for manuscript review and critical appraisal. This work was presented at the 2013 IAS Conference on HIV Pathogenesis, Treatment and Prevention in Kuala Lumpur, Malaysia.
Author Disclosure Statement
This study was funded by Pfizer Inc and funded by ViiV Healthcare.