
Abstract
Monotherapy with boosted protease inhibitors has emerged as an antiretroviral therapy simplification alternative for selected patients, endorsed by the results of some randomized clinical trials. However, there are some concerns about the efficacy of such a strategy in achieving successful viral suppression in those anatomic compartments or reservoirs in which antiretroviral drug penetration is lower, such as the central nervous system (CNS). Several studies have demonstrated better neurocognitive performance in patients receiving antiretroviral drugs with better cerebrospinal fluid (CSF) penetration. Nevertheless, cases of CSF viral escape accompanied by moderate or severe neurological symptoms have been reported with both standard triple therapy and boosted protease inhibitor (PI) monotherapy, and it is not well established whether ritonavir-boosted protease inhibitor (PI/r) monotherapy is associated with a higher risk of symptomatic CSF viral escape or not. Herein, we present a case of viral rebound and resistance emergence exclusively in CSF associated with an unusual clinical manifestation of focal encephalitis in a patient with plasma HIV-1 RNA suppression while receiving lopinavir/ritonavir monotherapy. Clinical resolution and CSF viral suppression were observed after switching to a genotype-guided combined antiretroviral regimen with good CSF penetration.
Introduction
T
Ritonavir-boosted protease inhibitor (PI/r) monotherapy with lopinavir/r or darunavir/r is a treatment simplification strategy that may reduce drug-related toxicity while maintaining viral suppression in selected patients. 12 –15 Despite the poor blood–brain barrier penetration of lopinavir/r and darunavir/r, CSF concentrations of both drugs seem sufficient to exceed the IC50 of a wild-type virus. 16,17 Cases of symptomatic CSF viral escape have been reported with both standard triple therapy and PI/r monotherapy, 9 –11,18,19 and it is uncertain whether PI/r monotherapy is associated with a higher risk of symptomatic CSF viral escape. 20
We present a case of focal encephalitis due to CSF viral escape associated with resistance emergence exclusively in CSF in a patient on lopinavir/ritonavir (LPV/r) monotherapy with virologic suppression in plasma.
Case Report
We report the case of a 44-year-old woman diagnosed with HIV-1 infection in 1992. She started ART in 1996 after being diagnosed with Pneumocystis jiroveci pneumonia. Her CD4+ T cell count nadir was 58 cells/μl (12%) and her highest plasma viral load (HIV-1 RNA) before ART was 22,700 copies/ml. She received stavudine, lamivudine, and ritonavir followed by stavudine, lamivudine, and nelfinavir between 1996 and 2000 with persistent virological failure, but genotypic resistance testing was not available.
In 2000, salvage therapy with stavudine, lamivudine, and lopinavir/r was initiated, achieving a plasma viral load under the limit of detection. Since then, her plasma viral load has remained undetectable. ART was switched to tenofovir, lamivudine, and lopinavir/r in 2006 and tenofovir/emtricitabine plus lopinavir/r in 2008. In 2011, therapy was simplified to lopinavir/r monotherapy. Treatment adherence and tolerance were good. In the last control, 2 months before hospital admission and 7 months after switching to monotherapy, her CD4+ cell count was 810 cells/μl (45%) and her plasma HIV-1 RNA was below the limit of detection (less than 40 copies/ml). In addition, the patient had chronic hepatitis C virus coinfection with mild to moderate liver fibrosis and depression, which was currently stable on citalopram treatment.
The patient was admitted to the hospital with a 5-day history of clonic movements associated with paresthesia in the left upper and lower limbs and ultimately generalized seizures, followed by paralysis of the left limbs. At arrival she had a well-preserved general status, was apyretic, and was conscious and oriented. The general physical examination was normal, but the neurological examination showed left brachiocrural paresis (4/5). During the first 48 h of hospitalization, clonic movements in the left limbs persisted. With the diagnosis of partial status epilepticus, levetiracetam 1,500 mg bid+oxcarbazepine 600 mg tid were prescribed, achieving remission. In addition, the patient presented with fever (37.7°–38°C), progression of left brachiocrural paresis (upper limb 2/5, lower limb 1/5), and left perioral paresthesia. Laboratory tests showed a CD4 count of 576 cells/μl (48%), a CD4/CD8 ratio of 2.6, plasma HIV-1 RNA of 216 copies/ml (poor compliance with ART during the past days because of neurological symptoms), and polyclonal hypergammaglobulinemia. All other hematological and biochemical parameters were normal.
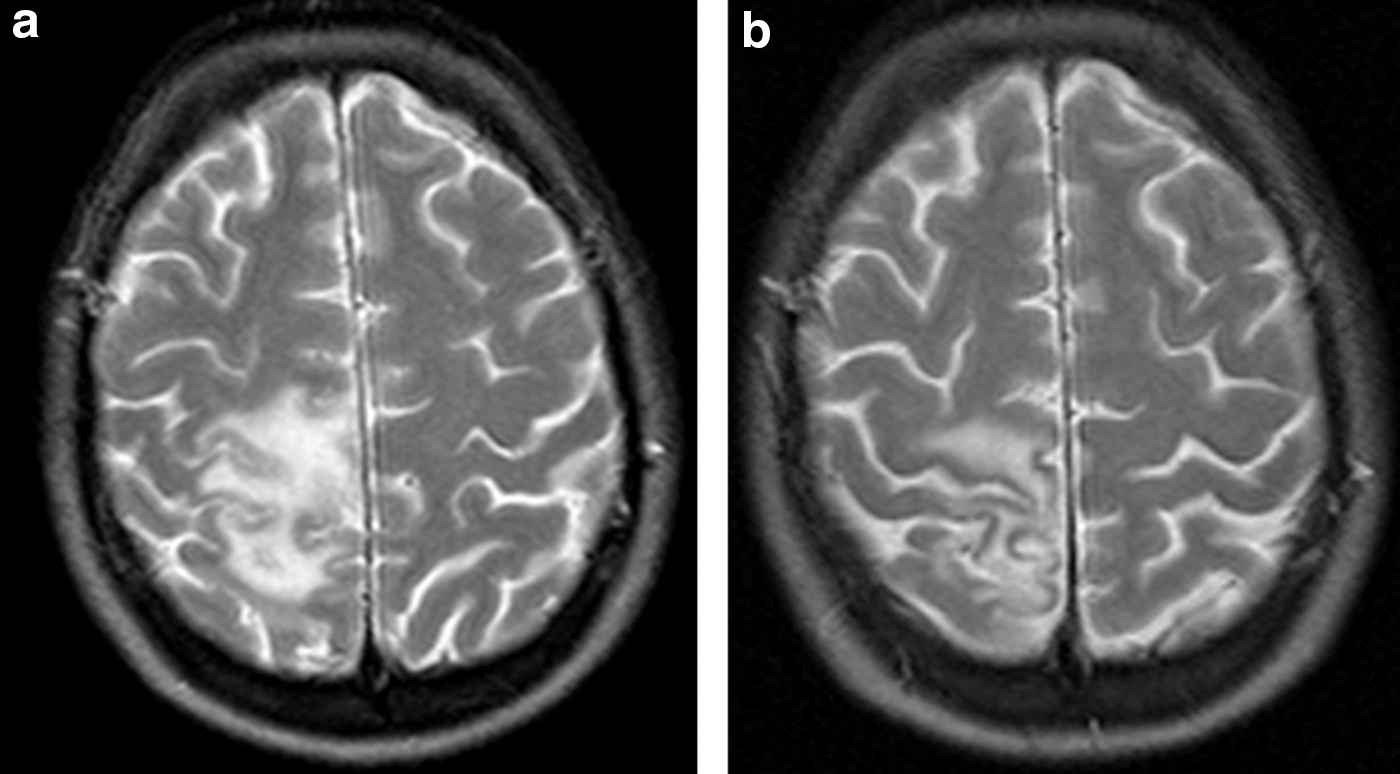
A cranial computed tomography (CT) study showed no abnormalities. However, magnetic resonance imaging (MRI) of the brain depicted a large area of confluent signal change, mainly affecting the subcortical white matter of the right parietal region, with no mass effect. The lesion was hyperintense on T2, FLAIR, and isotropic diffusion-weighted images, and hypointense on T1-weighted images. The lesion and adjacent perivascular areas showed a slight enhancement following gadolinium injection (Fig. 1a). Dynamic perfusion and spectroscopic findings were not suggestive of a brain tumor.
At the third day of admission, a lumbar puncture was performed. CSF findings included leukocytes 130/μl, 99% lymphocytes, proteins 0.71 g/liter (normal range 0.15–0.45), and normal glucose levels. Based on the fever and CSF data, empirical treatment with acyclovir and ampicillin IV was started. Blood cultures were negative. CSF microbiological testing was negative [bacterial culture, cryptococcal antigen, polymerase chain reaction (PCR) for Toxoplasma gondii, herpes simplex virus, cytomegalovirus, JC virus, and Mycobacterium tuberculosis complex] with the exception of PCR for Epstein–Barr virus (EBV; 1,304 copies/ml) and HIV-1 RNA 24,016 copies/ml. Genotypic resistance testing (GRT) of HIV-1 RNA from CSF showed several drug resistance-associated mutations in both the reverse transcriptase (T69N, V108I, M184V) and protease (V32I, L33F, I54V, L63P, A71V, V82A, L90M). A neoplastic origin of the brain lesion was ruled out by cytology and flow cytometry, and a diagnosis of HIV-1 encephalitis was established. Antiviral and antibacterial treatments were withdrawn, and ART was modified to active antiretroviral drugs according to the GRT findings, with good penetration through the blood–brain barrier: abacavir/lamivudine, ritonavir-boosted darunavir, and raltegravir (2010 CPE score: 10). 21
The lopinavir unbound concentration in CSF, determined by liquid chromatography–tandem mass spectrometry (LC-MS/MS) in a sample collected 3 days after hospital admission (6 h after drug intake), was 29 ng/ml (lopinavir CE50 for wild-type virus, 1.9 ng/ml). 16 Due to the low plasma HIV-1 RNA level, GRT was not performed on the plasma sample. To determine whether HIV-1 replication and resistance selection were restricted to the CSF, GRT was carried out in proviral DNA from peripheral blood mononuclear cells and no resistance-associated mutations were found.
The patient's clinical evolution was favorable. Eleven days after the change in ART the CSF characteristics were normal and CSF HIV-1 RNA was undetectable. The patient did not present new seizures, and left brachiocrural paresis improved except for a minimal residual motor impairment of the left foot. MRI performed 3 months later showed a decrease in the size of the frontoparietal lesion and contrast enhancement (Fig. 1b).
Discussion
We report a well-documented case of focal encephalitis related to viral escape and resistance emergence in the CSF of a patient with plasma HIV-1 RNA suppression on lopinavir/ritonavir monotherapy.
It is noteworthy that EBV activity was also observed in CSF. Although a wide spectrum of EBV-associated neurological diseases has been reported, neurological symptoms are rarely present in the absence of EBV systemic infection and CSF EBV activity occurs more frequently as intrathecal EBV reactivation in association with lymphoma or other CNS infections rather than as the primary cause of a CNS infection. 22 In our patient, plasma anti-EBV IgG antibodies had been tested in 2006 and they were positive. In addition, EBV viral load in CSF was not high, primary CNS lymphoma was ruled out, and neurological manifestations improved after optimization of ART. Therefore, EBV activity in CSF could be interpreted as a reactivation in the setting of HIV escape-related encephalitis.
The efficacy and safety of monotherapy with ritonavir-boosted lopinavir or darunavir have been assessed in clinical trials, 12 –14 and it can be considered an option for ART simplification in selected HIV-1-infected patients with sustained viral suppression and no previous failures with PIs, as is considered in some clinical guidelines. 23
Since a higher CSF penetration and effectiveness score have been associated with higher HIV suppression rates in CSF 5 –21 and better neurocognitive performance, 6,7 there is some concern about the capacity of PI/r monotherapy to effectively suppress HIV replication in this anatomical compartment. 20
Boosted lopinavir and darunavir both achieve CSF concentrations above the IC50 for the wild-type virus. 16,17 Viral load rebound in CSF accompanied by mild or moderate neurological symptoms, with or without viral suppression in plasma, has been observed in some PI/r monotherapy clinical trials, 14 –18 whereas others have reported no neurological problems. 12,13 In addition, more severe cases of encephalitis associated with viral escape in CSF and plasma HIV-1 RNA suppression have been described in patients receiving PI/r monotherapy and also in patients receiving standard triple ART. 9,11 Recently, the prevalence of neurocognitive impairment in virologically suppressed patients on PI/r monotherapy was evaluated in two observational studies, and PI/r monotherapy was not associated with poorer neurocognitive performance compared to triple therapy. 24,25
In our case, the patient had a low nadir CD4 cell count and previous treatment failure with nucleoside reverse transcriptase inhibitors (NRTIs) and unboosted PIs; hence, although plasma viral load remained below the limit of detection and the patient was asymptomatic for a long time, we must emphasize that PI/r monotherapy was not a good simplification alternative according to current recommendations. 15,23 The presence of the M184V mutation suggests resistance selection while receiving lamivudine.
The patient had been treated for years with tenofovir, a drug with poor CSF penetration, 15 lamivudine, or emtricitabine, an inactive drug (at least in the CSF) due to the M184V mutation, and lopinavir/ritonavir. We might speculate that she could have received functional monotherapy without viral escape during this period. However, tenofovir preserved at least some degree of activity, and the presence of M184V could have an additional effect on viral fitness. 26 In addition, the selection of PI resistance-associated mutations accompanying M184V while receiving lamivudine and unboosted PIs cannot be ruled out. In that case, the IC50 for lopinavir might be higher, the genetic barrier of resistance lower, and simplification to lopinavir/ritonavir could facilitate viral escape and accumulation of PI resistance mutations in the CSF, whereas plasma concentrations could suffice to maintain HIV-1 RNA under the detection level.
In conclusion, although there is no strong published evidence to date showing a higher risk of CSF viral escape and neurological problems with boosted PI monotherapy compared to standard combined ART, more studies are needed to clarify this issue. If PI/r monotherapy is considered a simplification strategy, rigorous patient selection is needed to guarantee optimal viral suppression in the most difficult to treat reservoirs, such as the CNS.
Footnotes
Acknowledgments
We thank Roger Paredes, MD, PhD, for his collaboration in sequencing HIV-1 DNA in PBMC and Adrian Curran, MD, PhD, for his contribution to the study of lopinavir concentration in CNS. We also thank Bellvitge Biomedical Research Institute (IDIBELL) for financial support for this article.
Author Disclosure Statement
No competing financial interests exist.