
Abstract

A 37-
He started oral fluconazole (100 mg/24 h) and HAART with tenofovir (300 mg)+emtricitabine (200 mg)+efavirenz (600 mg). Increasing dyspnea and a radiologic interstitial lung pattern developed in the following week. No microorganisms were found in the induced sputum. Empirical therapy for Pneumocystis jiroveci pneumonia with intravenous cotrimoxazol [trimethoprim (TMP) 240/sulfamethoxazole (SMX) 1,200 mg/6 h] was started. Dyspnea did not improve and small, painless, nodular skin lesions appeared in his trunk and limbs. Pancytopenia developed and cotrimoxazol was stopped. Increasing vision loss, mostly of the left eye, was reported.
A fundoscopic examination showed multiple choroidal nodules, binocular hemorrhages in the posterior and middle poles, and extensive left eye retinal necrosis. Blood CMV antigenemia, blood and aqueous CMV, herpes simplex virus (HSV)-1, HSV-2, varicella zoster virus (VZV) DNA, and Mycobacterium tuberculosis and Toxoplasma detection by polymerase chain reaction (PCR) were negative. The following days he became progressively lethargic. Head magnetic resonance imaging (MRI) showed increased T2 periventricular intensity and white matter peripheral nodules suggestive of cryptococcomas. A fine needle aspiration biopsy (FNAB) of an enlarged cervical lymph node showed encapsulated yeasts and fungal spores (Fig. 1). A normotense cerebrospinal fluid (CSF) with 4,000 red cells/μl, 976 leukocytes/μl [92% polymorphonuclear (PMN) and 8% lymphocytes], glucose 25 mg/dl, and proteins 62.4 mg/dl was obtained. Cryptococcus neoformans grew from the CSF. Blood (titer 1/8,148) and aqueous Cryptococcus antigenemia were also positive.
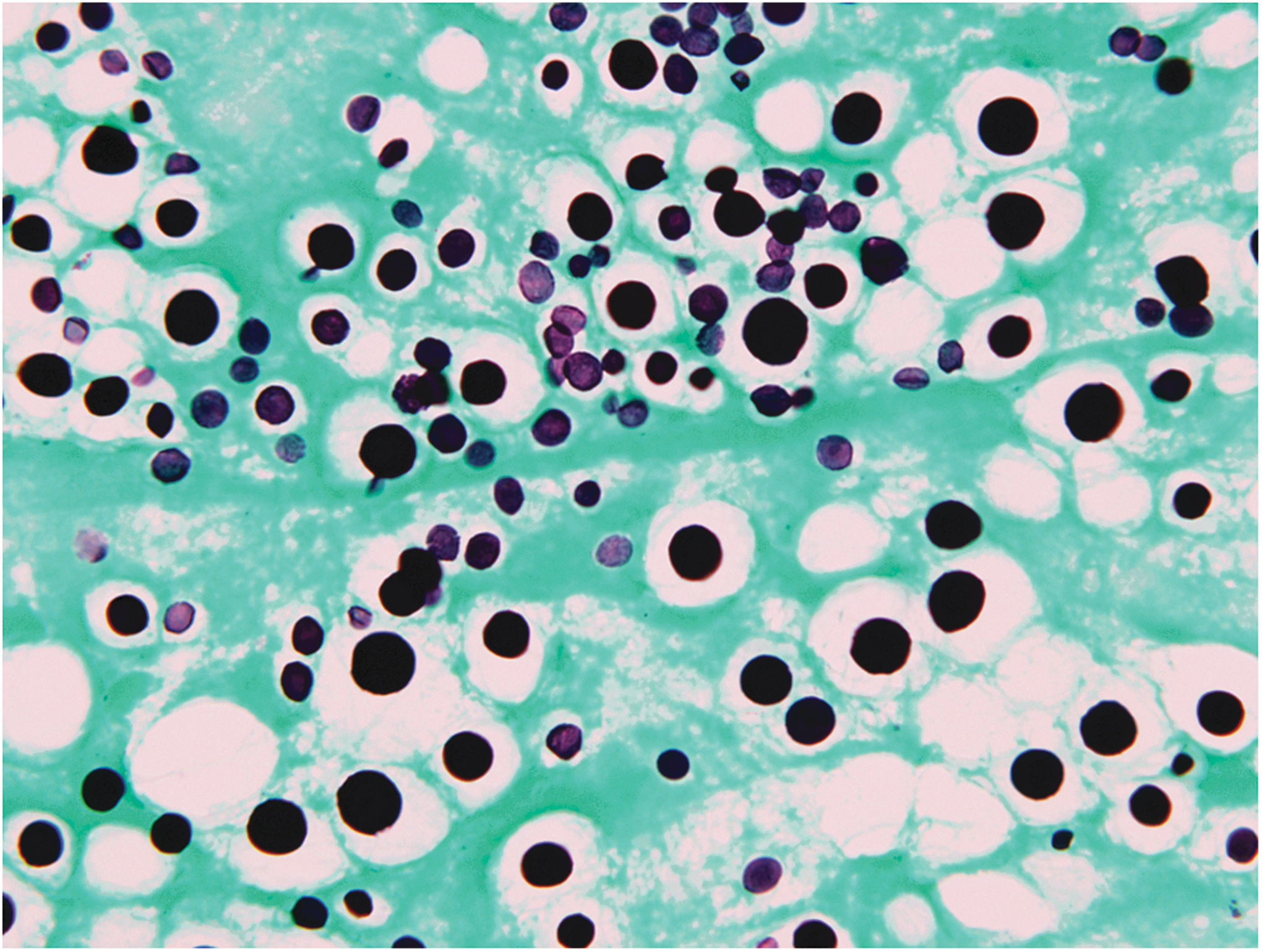
Cervical lymph node fine needle aspiration biopsy (FNAB). Grocott's methenamine silver stain (original magnification ×100). Numerous spores of different size, from 6 to 15 μm, are shown. The unstained peripheral halo corresponds to the polysaccharide capsule.
The patient was diagnosed with disseminated (neuromeningeal, lymphadenopathic, occulary, and probably skin and pulmonary) cryptococcal infection as manifestations of an immune reconstitution inflammatory syndrome (IRIS) after starting HAART. He underwent 5 weeks of intravenous therapy with liposomal amphotericin B (4 mg/kg/24 h), fluconazole (400 mg/12 h), dexamethasone (4 mg/6 h), and five intravitreal injections of voriconazole (100 μg/0.1 ml). Skin lesions and lymphadenopathies disappeared and full consciousness returned. CSF fungal culture after 5 weeks of antifungal therapy was negative. Blindness of the left eye persisted and the visual acuity in the right eye fell to 6/24. A CD4+ cell count of 60/μl (5%) and an HIV viral load of 1,230 copies/ml were obtained. He was discharged home with oral fluconazole (400 mg), cotrimoxazol (TMP 160/SMX 800 mg/three times a week), and HAART based on abacavir (600 mg)+lamivudine (300 mg)+darunavir (800 mg)+ritonavir (100 mg).
IRIS might unmask a latent disseminated cryptococcal infection in AIDS patients starting HAART. 1,2 Cryptococcal endophthalmitis is very rare, with only five cases reported in AIDS patients, with one associated with IRIS as this patient. 3,4 Choroidal nodules, retinal hemorrhages, and necrosis have been shown in cryptococcal endophthalmitis. Severe vision loss resulted in all the reported cases of AIDS cryptococcal endophthalmitis in spite of adequate antifungal therapy. 4
Footnotes
Author Disclosure Statement
No competing financial interests exist.