
Abstract

E
The patient is a 38-year-old treatment-naive female originally from Cameroon. She was diagnosed with HIV-1 infection in 1998 in Cameroon, and first presented to the United States in 2004 with an initial CD4 count of 576 and a viral load of <50 copies/ml as measured by the Roche AMPLICOR HIV-1 MONITOR 1.5 ultrasensitive assay. She maintained stable CD4+ T cell counts and viral loads of <50 copies/ml in the absence of ART (Fig. 1A) over the next 6 years. The rate of CD4+ T cell decline was calculated as described previously. 5 We found that there was no significant decline in CD4+ T cells between 2005 and 2010 (p=0.0615). HLA typing revealed that she was HLA-A*02/66 and HLA-B*42/53 positive.
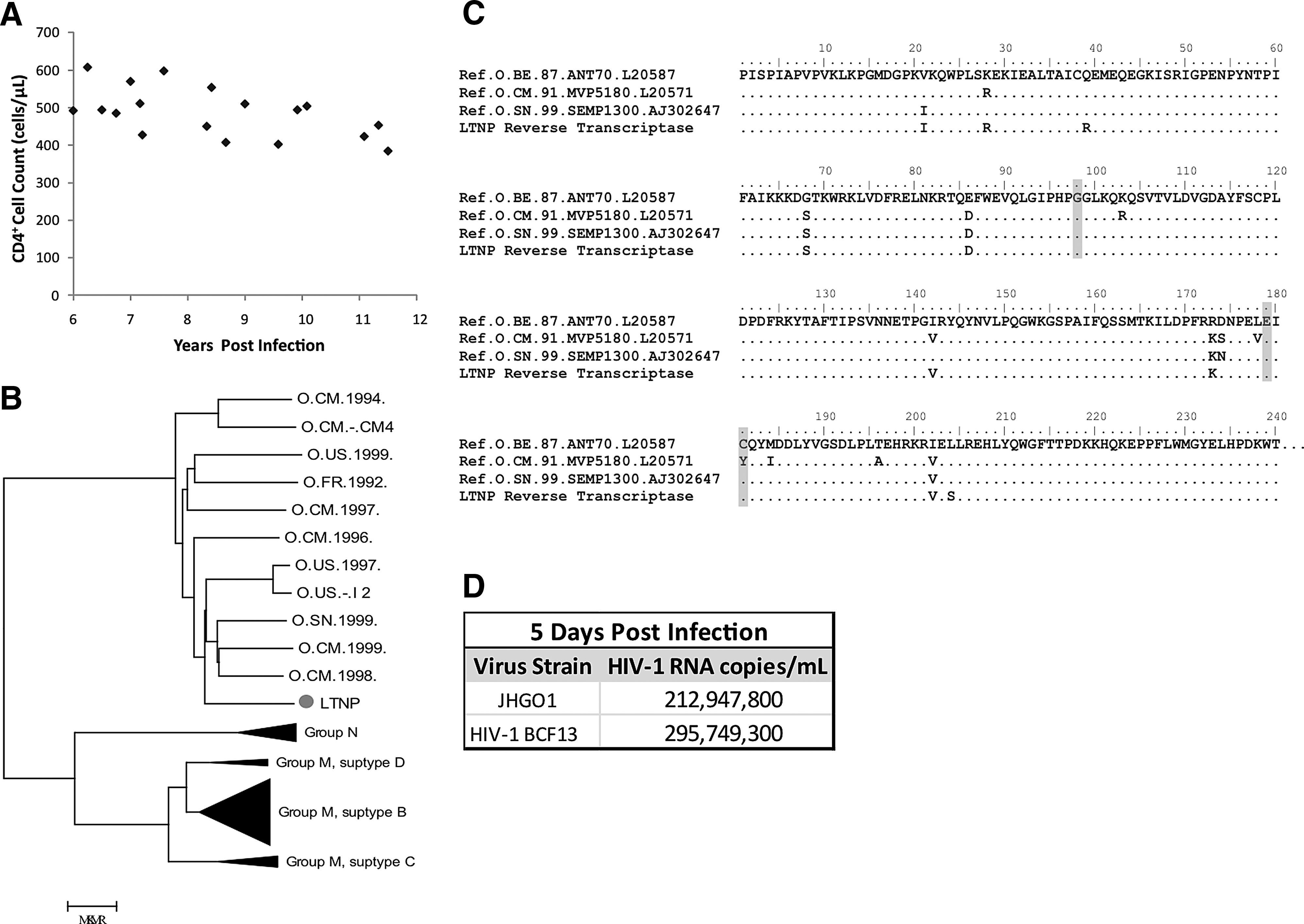
Virus was cultured from the patient's latent reservoir as previously described 6 in 2010 and designated JHGO1. Phylogenetic analysis was performed on full length env sequences of the patient's virus compared to Group O, N, and M isolates. Classical, maximum likelihood, and Bayesian phylogenetic analysis was performed. The patient's virus was most closely related to HIV-1, Group O (Fig. 1B). Group O nested-PCR primers were developed utilizing full genome Group O sequences from the Los Alamos HIV Sequence database and full genome sequencing was performed (GenBank accession number JN571034). No gross sequence defects were seen compared to other Group O viral sequences. Evolutionary differences in Group O reverse transcriptase (RT) have resulted in resistance to nonnucleoside reverse transcriptase inhibitors (NNRTIs) in many treatment-naive patients. 7 The patient's virus had mutations A98G, V179E, and Y181C in RT (Fig. 1C), all of which have been reported to confer resistance to NNRTIs. 7 The virus isolated from the patient's latent reservoir was found to be as replication-competent as a Group O HIV-1 laboratory strain (HIV-1 BCF1 8 ) in a viral fitness assay where activated CD4+ T cells from seronegative donors were infected with 200 ng/ml p24 of either the patient's isolate or the laboratory strain as previously described 6 and HIV-1 RNA in culture supernatant was quantified on day 5 postinfection with the Abbott m2000 RealTime HIV Assay (Fig. 1D). 9
The patient's plasma viral load was subsequently determined to be 2,682 RNA copies/ml by the Abbott m2000 RealTime HIV Assay. The Roche AMPLICOR HIV-1 MONITOR test remained <50 copies/ml consistent with studies showing that the latter test does not routinely detect Group O HIV-1 isolates. 9
Taken together, although this patient was initially misclassified as an elite controller, her stable CD4+ T cell counts and low viral load indicate that she is a long-term nonprogressor (LTNP). LTNPs have previously been identified in Group M infection, but to our knowledge, long-term nonprogression in patients infected with a Group O virus has not been previously reported. Infection with a defective virus accounts for some cases of long-term nonprogression, 10 but multiple studies have also shown that replication-competent virus can be isolated from some LTNPs and elite controllers. 11 It is clear that host factors, such as protective HLA types and HIV-specific CD8+ T cells, play a large role in the control of HIV-1 infection. 12 This patient possessed no previously reported protective HLA alleles, but a substantial proportion of LTNPs and elite controllers (EC) do not have these alleles. 13 Our fitness assay results suggest that this patient is not infected with a defective virus. While we were not able to study HIV-specific CD8+ T cell function in this patient, it appears that host factors were responsible for control of viral replication. This case suggests that some Group O-infected individuals can partially control fully pathogenic virus.
Footnotes
Acknowledgments
The following reagent was obtained through the NIH AIDS Reagent Program, Division of AIDS, NIAID, NIH: HIV-1BCF13 from Drs. Sentob Saragosti, Françoise Brun-Vézinet, and François Simon.
Author Disclosure Statement
No competing financial interests exist.