
Abstract

E
In many earlier studies of antiretroviral treatment (ART) in Yunnan, follow-up was restricted to 2 years or less. 3,4 Because current ART only slows the progress of infection, short-term observations cannot present the full effects of treatment. Many domestic studies also focused on HIV-1 drug resistance, but data on modifying initial ART regimens in China are limited. 5 Modifying regimens during treatment is common, and exploring the incidence and causes of modification has real, far-reaching significance for HIV prevention and treatment policies.
A prospective cohort study of 144 treatment-eligible HIV patients was initiated in Yunnan in 2004. The study period extended from ART initiation to 2010, and the endpoints were either virological or immunological failure according to WHO guidelines. 6 The median length of follow-up per person was 4.24 years (IQR: 3.88–4.75).
Sixteen (11.1%) patients demonstrated virological failure and 34 (23.6%) experienced immunological failure during the study, for overall failure rates of 2.79 per 100 person-years (95% CI: 1.71–4.55) and 6.17 per 100 person-years (95% CI: 4.41–8.64), respectively (Figs. 1 and 2). The viral suppression rate (88.89%) in our study was higher than in a previous study in Yunnan (75.49%), while the immune reconstitution rate (79.16%) was comparable to previous studies in China. 3 –5
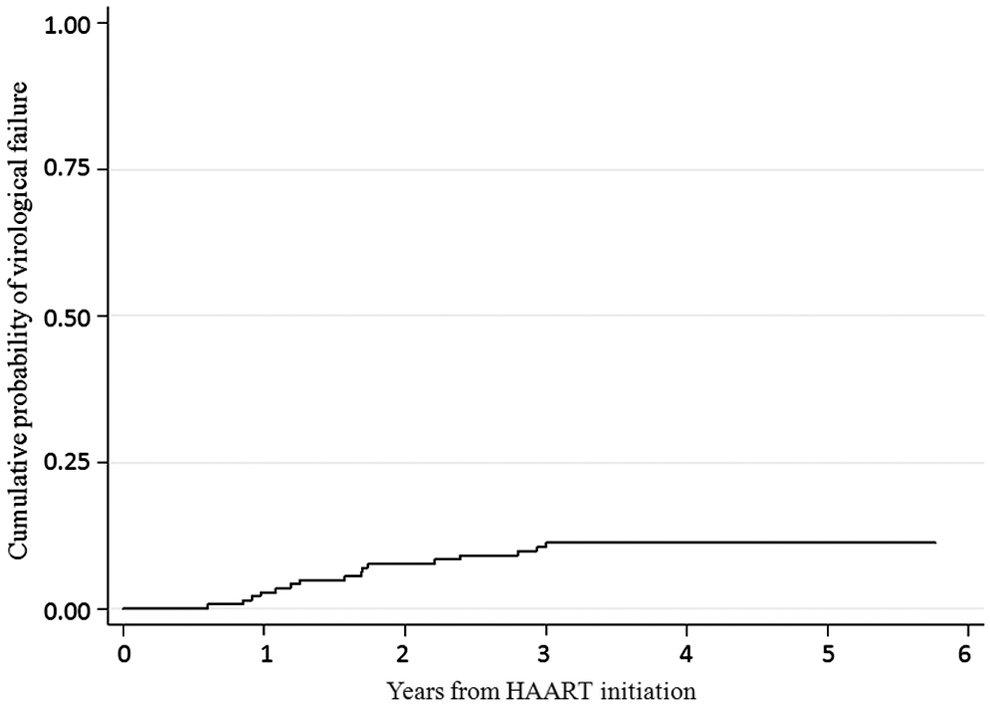
Kaplan–Meier curve of cumulative probabilities of virological failure.
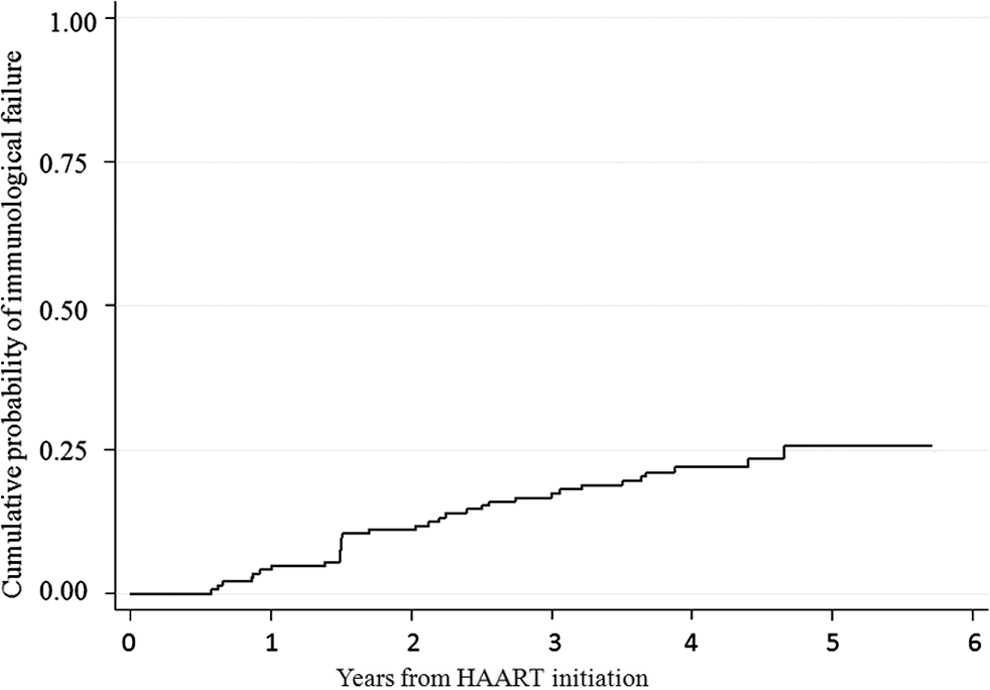
Kaplan–Meier curve of cumulative probabilities of immunological failure.
In our study, male gender [hazard ratio (HR)=5.22, 95% CI: 1.58–17.21] was a risk factor for immunological failure, while infection through injection drug use (HR=0.27, 95% CI: 0.08–0.92) or having a baseline CD4 cell count >200 cells per μl (HR=0.29, 95% CI: 0.09–0.90) was a protective factor. Fifty-four (37.5%) patients modified their initial regimen at a median of 20.9 months (IQR: 6.9–33.4) after treatment started. At 3 months after initiating ART, 92.75% of patients alive and in active control remained on their initial regimen, at 1 year, 84.72% remained on their first regimen, and at the end of the study, 62.5% remained (Fig. 3). The reasons for modification included adverse reactions to ART (77.78%) and other reasons (22.22%). The most common adverse events were myelosuppression (16%), abnormal liver function (15%), and peripheral neuritis (15%). Among patients who had substituted first-line regimens, only four had theirs changed to a second-line treatment. Most regimen changes were simple drug substitutions, followed by other unspecified changes.
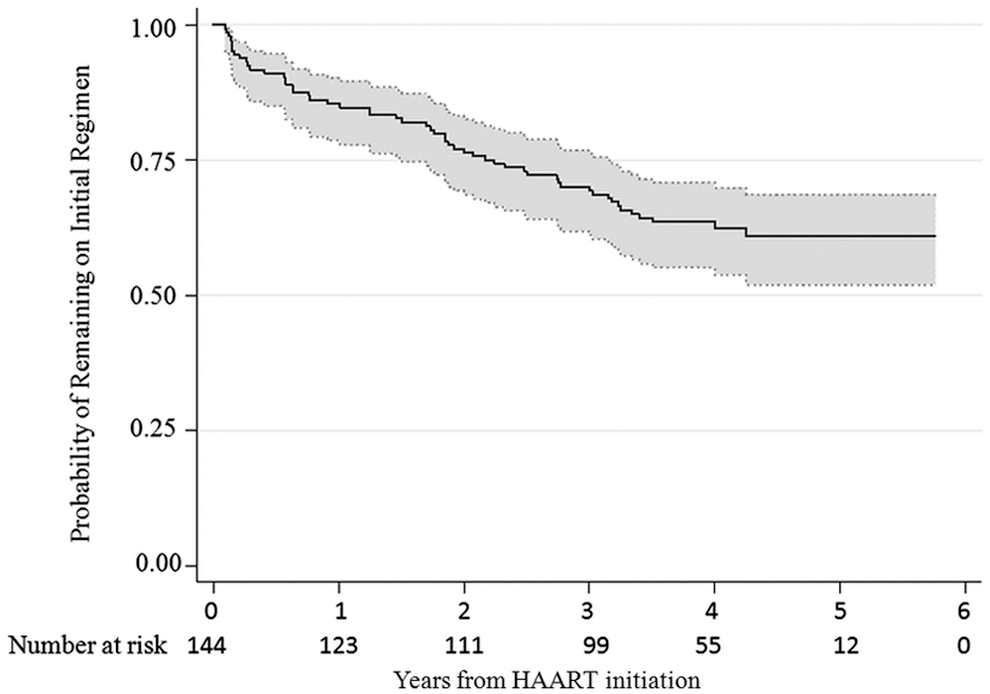
Kaplan–Meier curve of probability of maintenance in the first antiretroviral regimen.
Previous studies have suggested that adverse drug reactions are a key factor affecting treatment adherence. Magnano et al. 7 reported a significant association between adherence and successful treatment outcomes. The results of our study support this conclusion to some degree. With a high retention rate (97.9%) in treatment, although regimen modification occurred at a relatively high frequency due to adverse reactions, the effect of ART was satisfactory compared with previous similar research. 3 –5
The results indicate the importance of managing adverse reactions, preferably by diversifying ART regimens. Based on the wide range of options, clinicians can individualize treatment regimens according to patients' characteristics. Timely monitoring and management of adverse events during treatment are also practical.
Footnotes
Acknowledgments
This work was supported in part by the Natural Science Foundation of China (81001288, 11171268), the National S&T Major Project Foundation of China (no. 2012ZX10001-001), and the Priority Academic Program Development of Jiangsu Higher Education Institutions (PAPD).
The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author Disclosure Statement
No competing financial interests exist.