
Abstract

V
Figure 1 presents a lymphonodal biopsy showing a lymphoadenopathy sustained by Leishmania.
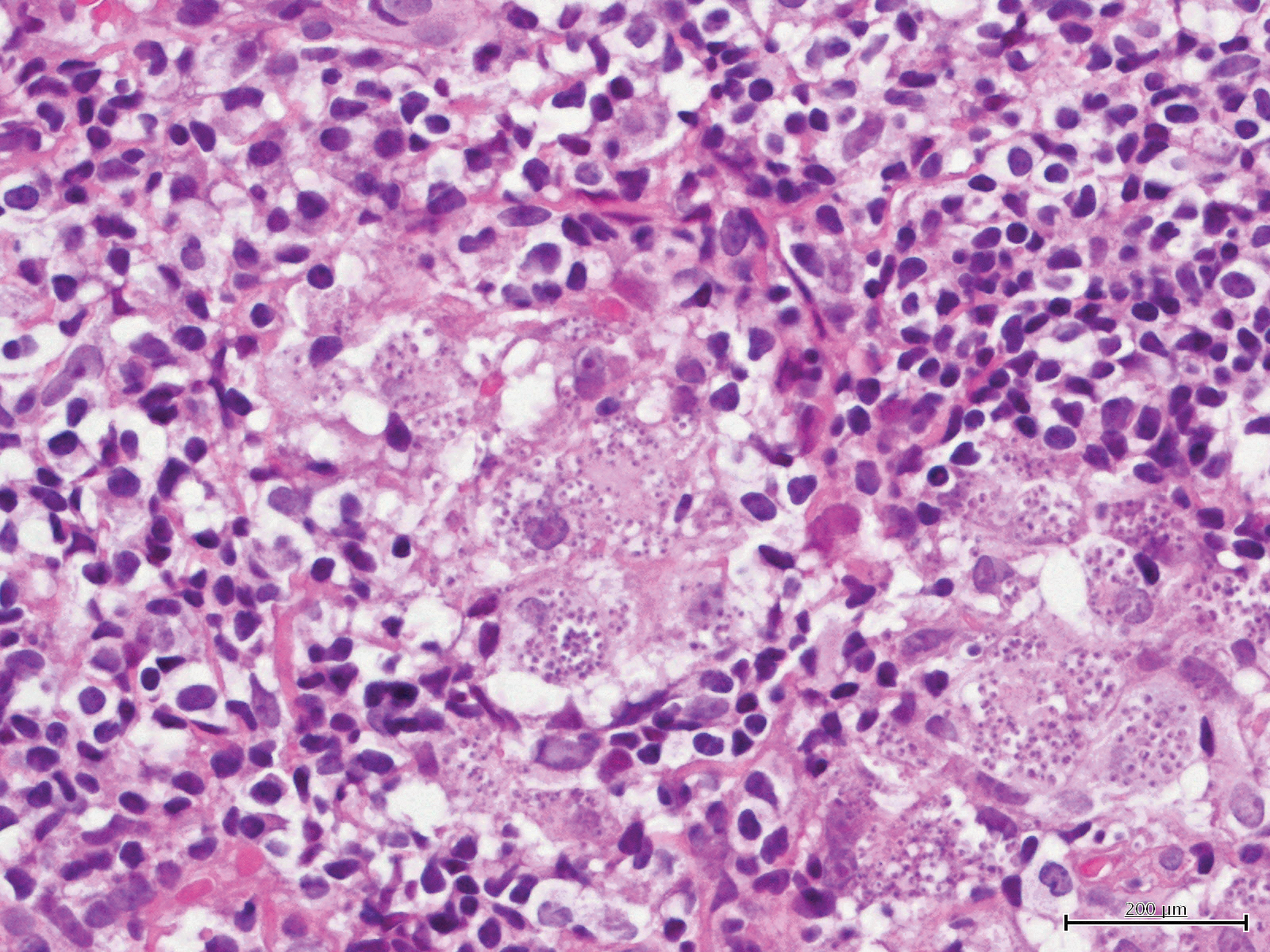
Lymph node. Leishmania organisms are within the cytoplasm of the macrophages. H&E 800×.
The patient, a 55-year-old man, had HIV and was receiving antiretroviral therapy with emtricitabine, tenofovir, atazanavir, and ritonavir. The treatment had been successful, achieving an undetectable HIV viral load (<50 HIV-RNA copies/ml); nevertheless, immunological discordance was observed with a modest immune recovery (CD4+ count always <300 cells/mm3). The patient was hospitalized because of persistent fever and leucopenia; during hospitalization splenomegaly and a generalized enlargement of the lymph nodes were detected and confirmed at CT scan, leading to a workup to investigate a possible hematological malignancy. A lymph node biopsy showed the presence of Leishmania spp. (Fig. 1). The biopsy showed a pattern characterized by Leishmania amastigotes.
In addition, Leishmania antigen was detected in urine samples and Leishmania serology (IFAT) was positive. A bone marrow biopsy revealed intracellular parasites on Giemsa staining. The patient was treated with liposomal amphotericin B and rapidly recovered. Thus, diffuse lymphoadenopathy sustained by Leishmania infantum does not always represent a benign localized disease, and may be associated with a complex clinical presentation as previously reported. 5 In immune-suppressed subjects with Leishmania lymphadenopathy, bone marrow and urinary antigen evaluation are indicated.
The present case was observed and evaluated within the frame of a clinical regional registry, Registro Ligure Leishmaniosi Viscerale (RiLLeVI). In areas of endemicity with a relatively low incidence, long-term registries collecting viral load cases are a useful tool to maintain a clinical perspective, to share experience concerning unusual manifestations of the disease, and to record specific local epidemiological trends.
Footnotes
Author Disclosure Statement
No competing financial interests exist.