
Abstract
In Thailand, new HIV-1 infections are largely concentrated in certain risk groups such as men who have sex with men (MSM), where annual incidence may be as high as 12% per year. The paucity of information on the molecular epidemiology of HIV-1 in Thai MSM limits progress in understanding the epidemic and developing new prevention methods. We evaluated HIV-1 subtypes in seroincident and seroprevalent HIV-1-infected men enrolled in the Bangkok MSM Cohort Study (BMCS) between 2006 and 2011. We characterized HIV-1 subtype in 231 seroprevalent and 194 seroincident subjects using the multihybridization assay (MHA). Apparent dual infections, recombinant strains, and isolates found to be nontypeable by MHA were further characterized by targeted genomic sequencing. Most subjects were infected with HIV-1 CRF01_AE (82%), followed by infections with recombinants (11%, primarily CRF01_AE/B recombinants), subtype B (5%), and dual infections (2%). More than 11 distinct chimeric patterns were observed among CRF01B_AE/B recombinants, most involving recombination within integrase. A significant increase in the proportion of nontypeable strains was observed among seroincident MSM between 2006 and 2011. CRF01_AE and subtype B were the most and least common infecting strains, respectively. The predominance of CRF01_AE among HIV-1 infections in Thai MSM participating in the BMCS parallels trends observed in Thai heterosexuals and injecting drug users. The presence of complex recombinants and a significant rise in nontypeable strains suggest ongoing changes in the genetic makeup of the HIV-1 epidemic in Thailand, which may pose challenges for HIV-1 prevention efforts and vaccine development.
Introduction
D
Because of variability of the HIV-1 genome, the distribution of viral genetic polymorphisms may vary significantly between different geographic regions, and between different risk groups within the same area. This may reflect founding viral strains at the time of introduction, diversification over time, and behavioral factors determining cross-exposure between risk groups. 13 –16 Knowledge of circulating HIV-1 viral strains and subtypes is also considered fundamental for the development of effective HIV-1 prophylactic vaccines 14,15,17 designed to elicit cytotoxic T lymphocyte responses to relevant epitopes, 18 –21 or antibodies capable of neutralizing a broad range of possible infecting viruses. 22 –24
Molecular epidemiological studies are an important tool to understanding patterns of transmission from region to region, defining transmission pathways between groups and individuals, and guiding development of interventions capable of eliciting protective adaptive immune responses.
Despite the potentially informative nature of viral genetic studies, compared to other risk groups in Thailand, 25 –32 the subtype distribution of HIV-1 strains prevalent among MSM has not been well characterized. Only one previous study identified 99 MSM from among many clients attending an HIV-1 voluntary counseling and testing clinic in Bangkok. 33 While limited due to its cross-sectional nature and possible inclusion of repeat clients, a higher prevalence of non-CRF01_AE infections in MSM compared to other risk groups was found. The data also suggested that some MSM may have had dual infection, but this was not definitively evaluated using gene sequencing methods.
Given the increasing importance of HIV-1 transmission among MSM in sustaining the overall HIV-1 epidemic in Thailand and on a global level, it is vital to develop a clear picture of the molecular epidemiology of HIV-1 infection in MSM and to understand the significance of regional and temporal trends in this group. Though typically more resource intensive and challenging to implement, cohort studies distinguish themselves from cross-sectional studies in providing an opportunity to evaluate HIV-1 genetic epidemiology in a well-characterized population over time. We previously established an MSM cohort study in Bangkok, Thailand. 9 Enrollment began in 2006 and accrued 1,744 participants. Over 5 years of follow-up (2006–2011), we documented a high HIV-1 prevalence (22.4%) and incidence (5.9/100 person-years) in this population. 9 In this article, we characterize seroprevalent and seroincident infecting HIV-1 subtypes by a multiregion hybridization assay (MHAbce) in this cohort. We further evaluate possible dual and recombinant infections by gene sequencing, and present trends over time among seroprevalent and seroincident cases over 5 years of follow-up.
Materials and Methods
Study subjects and specimen collection
Screening and enrollment of participants in the Bangkok MSM Cohort Study (BMCS) were conducted from April 2006 to January 2008 (period 1) and from September 2009 to November 2010 (period 2). 9 The present viral diversity study includes seroprevalent study subjects enrolled during period 1 and seroincident study subjects identified during follow-up of men enrolled during both periods until December 2011. Oral fluid, EDTA whole blood, and citrate plasma were collected from all participants at baseline and follow-up visits every 4 months. Blood specimens for MHA, CD4, and HIV-1 RNA viral load were collected at the time of enrollment from seroprevalent study subjects and from seroincident study subjects on the date of the first HIV-1-seropositive test or shortly thereafter.
Ethical review
The protocol of this study was reviewed and approved by the Thailand Ministry of Public Health Ethical Review Committee for Human Subjects Research, the Institutional Review Board of the U.S. Centers for Disease Control and Prevention, and the Human Subject Research Review Board of the U.S. Army Medical Research and Materiel Command. Informed consent was obtained from all participants prior to enrollment in the study.
HIV-1 testing
Subjects were screened for the presence of HIV-1 antibodies in oral fluid (OraQuick, Orasure Technologies, USA) at enrollment and every 4 months thereafter. HIV-1 reactive oral fluid tests were confirmed in blood using three consecutive HIV-1 rapid tests in accordance with Thai National Guidelines for rapid HIV testing (Determine, Abbott, USA; DoubleCheck, Orgenics Ltd., Israel, or SD Bioline, Standard Diagnostics, Inc., Korea; and Capillus HIV-1/2, Trinity Biotech, USA, or HIV1/2 Core, Core Diagnostic, UK). 9 From February 2010 onward, plasma samples from volunteers testing nonreactive on oral fluid were evaluated for acute HIV-1 infection using fourth-generation EIA (AxSym HIV 1/2 Ag/Ab Combo, Abbott, USA) and NAT (Aptima Genprobe, USA). Study subjects were considered to be seroprevalent if they were determined to be HIV-1 infected at the time of enrollment and seroincident if they were found to be HIV-1 infected during follow-up.
CD4+ cell count and plasma HIV-1 RNA viral load determination
CD4+ cell count was performed on EDTA whole blood by single platform volumetric flow cytometry (Guava Easy CD4, Millipore, USA). HIV-1 RNA was quantified in plasma using COBAS TaqMan HIV-1 version 1.0 (Roche Molecular Systems, USA). The lower limit of detection was 47 copies/ml. Plasma without HIV-1 RNA detected was recorded as 0 copy/ml.
HIV-1 Genotyping by MHA
HIV-1 RNA was extracted from 200 μl of plasma using the QIAamp Viral RNA Mini Kit (Qiagen, USA). HIV-1-negative samples and water were used as negative controls and previously characterized HIV-1-positive samples were used as positive controls. HIV-1 genotyping was performed by multiregion hybridization (MHAbce version 2), optimized for the detection of HIV-1 subtype B (referred to as the Western B strain), subtype C, and CRF01_AE, 34 using an ABI HT 7900 real-time PCR machine (Applied Biosystems, USA). Classification of circulating HIV-1 subtypes by MHAbce was identified according to established criteria. 33 A genotype was assigned when probe hybridization occurred in at least four of eight genomic regions: (1) a single subtype (B, C, or CRF01_AE) was assigned when all hybridizing probes were of the same subtype; (2) recombinant forms (BE, BC, CE, or BCE) were assigned when two or more different subtype probes hybridized in different regions of the genome; and (3) infection with multiple subtypes (for example, putative dual infection) was tentatively assigned when probes of two or more different subtypes hybridized in the same genome region (more than one subtype/region). We defined a strain as “nontypeable (NT)” when there was probe reactivity and/or sequence information in fewer than four genomic regions and as “nonamplifiable (NA)” when there was no evidence of PCR amplicons as determined by SyberGreen, a fluorescent dye staining double-stranded DNA.
All putative multiple infections identified by MHAbce were confirmed by cloning of PCR-amplified nucleic acids, followed by repeated MHAbce on individual clones. Briefly, PCR amplicons corresponding to regions showing dual probe reactivity in MHAbce were ligated into TOPO vector (TOPO TA cloning, Invitrogen, USA) carrying plasmid encoding antibiotic resistance, and then transformed into competent cells. Transformants carrying ligated plasmids were selected on LB plates containing 50 μg/ml kanamycin and β-galactose. Subsequently, 16–32 ligated clones were used for repeated genotyping by MHAbce and for sequencing, 35 as specified below.
Genotyping by targeted genomic sequencing
All samples classified as “putative dual infections” and seroincident samples classified as “recombinant” and “nontypeable” by MHAbce were further characterized by targeted genomic sequencing. For apparent dual infections by MHAbce, 2–12 transformed clones were used for sequencing. For samples designated as “recombinant,” amplicons from all gene regions showing possible recombination by MHA were used for bulk sequencing. For samples designated as “nontypeable” by MHAbce, amplified DNA from all gene regions without MHA results were used for bulk sequencing. All sequencing was performed with Big Dye terminators on an ABI 3130 Capillary sequencer (Applied Biosystems, USA) as previously described. 34 Target gene sequences from the HIV-1, rt, int, tat, gp120, gp41, and nef were aligned with reference strains from the Los Alamos HIV-1 database, including representative HIV-1 CRF01_AE, subtype B strains, subtype C strains, and recombinant strains circulating in Thailand and neighboring countries. Alignments were made using Clustal W, 36 and manually edited using Genetic Data Environment (GDE 2.4, Rockville, MD) or MacClade 4.08a.
Maximum-likelihood phylogenetic analyses were performed using the best-fit model of molecular evolution estimated by Moldeltest using the Akaike Information Criterion (AIC). 37 Phylogenetic trees were reconstructed under the general time reversible model of nucleotide substitution, with proportion of invariable sites and gamma distribution rate heterogeneity (GTR+I+G) using PAUP* 38 within Geneious Pro5.5.6 (Biomatters). Bootstrap resampling was performed with 500 replicates. A bootstrap value of ≥70% was considered to be evidence of monophylogeny. 39 Confirmed dual infections were defined as the presence of two different sequence subtypes or circulating recombinant forms in one sample.
Statistical analyses
Differences in median age, CD4+, and viral load between seroprevalent and seroincident study subjects were evaluated with the Wilcoxon rank-sum test using SAS version 9.3 (SAS Institute, Cary, NC). We evaluated trends in HIV-1 subtype distributions over time using the chi-square test with StatCalc (Epi Info 7). p-values <0.05 were considered statistically significant. Nontypeable and nonamplifiable samples were excluded from the denominator in calculations of HIV-1 subtype distributions.
Results
HIV-1 prevalence, incidence, and participant characteristics
Of the 1,292 men who enrolled during period 1, 290 (22.4%) tested positive for HIV-1 infection. Of the 1,372 men testing negative for HIV-1 infection at enrollment during periods 1 and 2, 216 seroconverted for HIV-1 infection during follow-up until December 2011 (HIV-1 incidence: 5.9 per 100 person-years). Blood samples for laboratory testing were collected on the same day as first HIV-1-seropositive testing (61% of all subjects) or as soon as possible thereafter (median duration: 13 days; range 1–487 days). The median CD4 cell count was higher in seroincident men (479; range 5–1,105 cells/μl) than in seroprevalent men (424; range 28–1,712 cells/μl; p<0.05). The median HIV-1 RNA viral load (VL) was also higher among seroincident men (79,600; range 0–85,600,000 copies/ml) than seroprevalent men (43,550; range 0–2,010,000 copies/ml; p<0.05). There was no significant difference with respect to median age between the two groups of men (26 years; range 18–52 years).
Performance of MHAbce version 2
A total of 278 (95.9%) seroprevalent and 211 (97.7%) seroincident study subjects had samples available for HIV-1 subtyping by MHAbce. Of these 489 samples, 425 (86.9%) were successfully genotyped by MHAbce and sequencing. Among seroprevalent subjects, 83% could be typed, 12% were successfully amplified but HIV-1 subtype could not be assigned (nontypeable by MHAbce only), and 5% failed PCR amplification (NA) due to low HIV RNA VL. Among 211 seroincident subjects, 92% could be typed, 6% were nontypeable (by MHAbce and sequencing), and 2% failed PCR amplification (Supplementary Table S1; Supplementary Data are available online at
HIV-1 subtype distribution, patterns of HIV-1 recombination, and dual infections
The distribution of HIV-1 genotypes in seroprevalent and seroincident subjects is described in Table 1. Overall, most MSM (82%) were infected with CRF01_AE. Non-CRF01_AE strains accounted for 18% of infections, among which 11% were recombinants, 5% were subtype B, and 2% were dual infections. Recombinant infections were primarily CRF01_AE/B. Using MHAbce, 18 putative dual infections were detected. Of these, seven (three among incident infections and four among prevalent infections) were confirmed to be dual infections by phylogenetic analysis of gene sequences (Table 1 and Fig. 1). In the remaining 11 cases, which did not meet the criteria for dual infections, phylogenies were characterized by relatively long-branch lengths reflecting highly diverse populations (mean genetic diversity=0.043; range 0.002–0.24; data not shown).
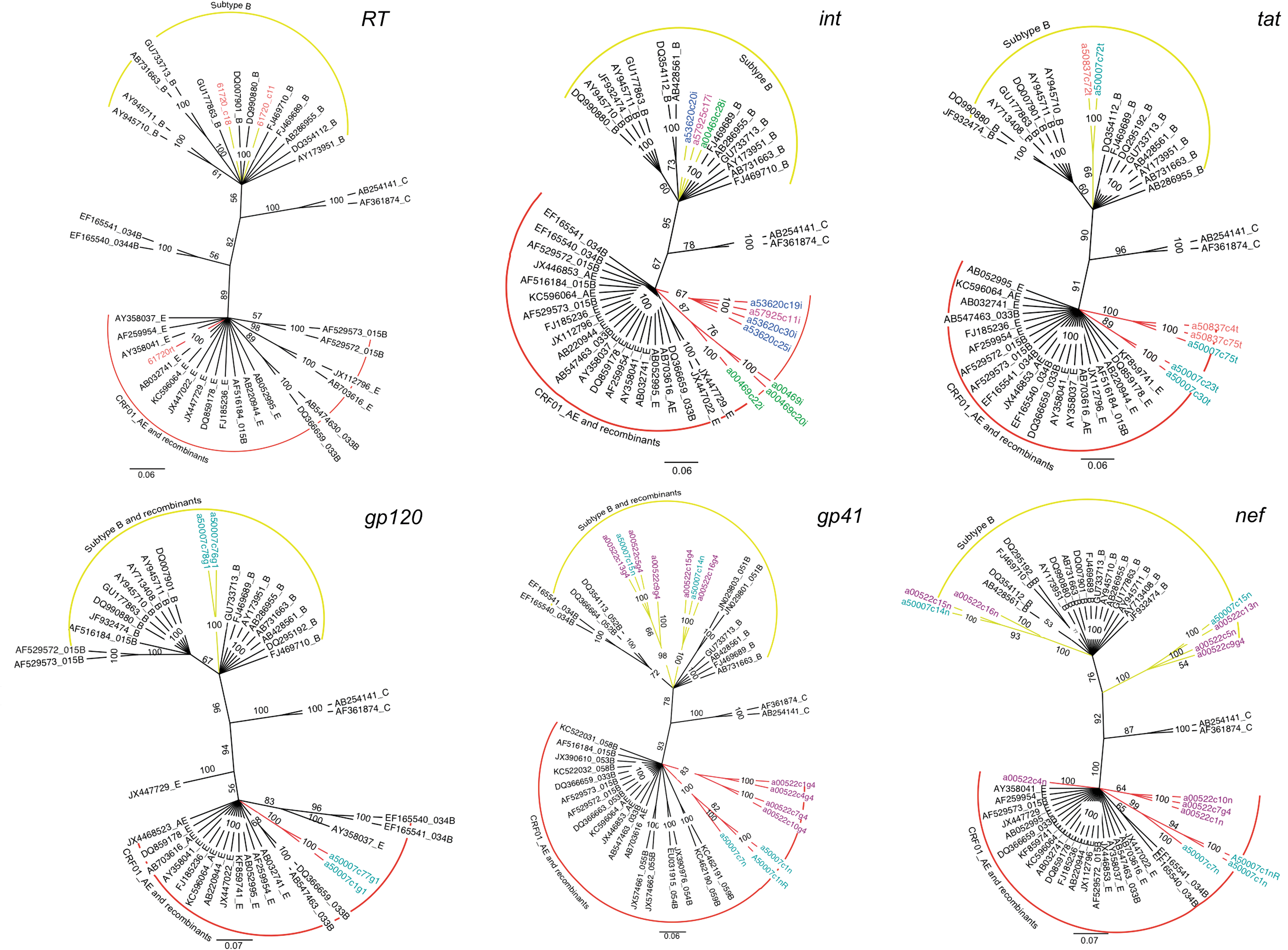
Maximum-likelihood phylogenetic analysis of HIV-1 rt, int, tat, gp120, gp41, and nef sequences from seven individuals showing multiple infections. Taxa from study subjects are color coded by subject (subtype is indicated by branch colors). Reference isolates (black taxa) are represented by accession numbers and their subtypes. Values at the nodes show percent bootstrap support (500 replicates). The scale bar indicates substitution per site.
Number of samples genotyped by multihybridization assay (MHA) and number of samples that could be typed. Dual infections were classified separately from recombinants.
Number and percentage (%) of given HIV-1 subtype (nontypeable and nonamplifiable samples are excluded from the denominator).
NT, nontypeable samples, NA, nonamplifiable samples presented by number and percentage (%) where number of samples genotyped was used as the denominator.
Seroprevalent samples were defined as HIV-positive samples identified at screening; seroincident samples were defined as HIV-positive samples identified after enrollment; all samples included both seroprevalent and seroincident samples.
Among the 43 CRF01_AE/B recombinants identified, 11 distinct patterns of intersubtype recombination were observed, including eight possible novel forms. Five recombinants involved substitution within the integrase gene (Fig. 2) and accounted for the majority (33/43) of recombinations observed. In each case, sequences consisted of a predominant CRF01_AE background with one or more subtype B fragments in integrase with or without recombination in other regions: int only (20/43, 47%), int and nef (2/43, 5%), int and rt (5/43, 12%), int, rt, and tat (2/43, 5%), int, rt, and gp120 (3/43, 7%), and int, rt, tat, and nef (1/43, 2%). The remaining recombinants had subtype B fragments in other regions: rt (5/43, 12%), nef (2/43, 5%), gp120 (1/43, 2%), gp41 and nef (1/43, 2%), and tat (1/43, 2%). Three recombinants involving subtype C were identified by MHA. In all cases, these consisted of a subtype B background with a subtype C integrase fragment (B/C recombinant), with or without CRF01_AE fragments in p17 and gp41 (B/C/CRF01_AE recombinant).
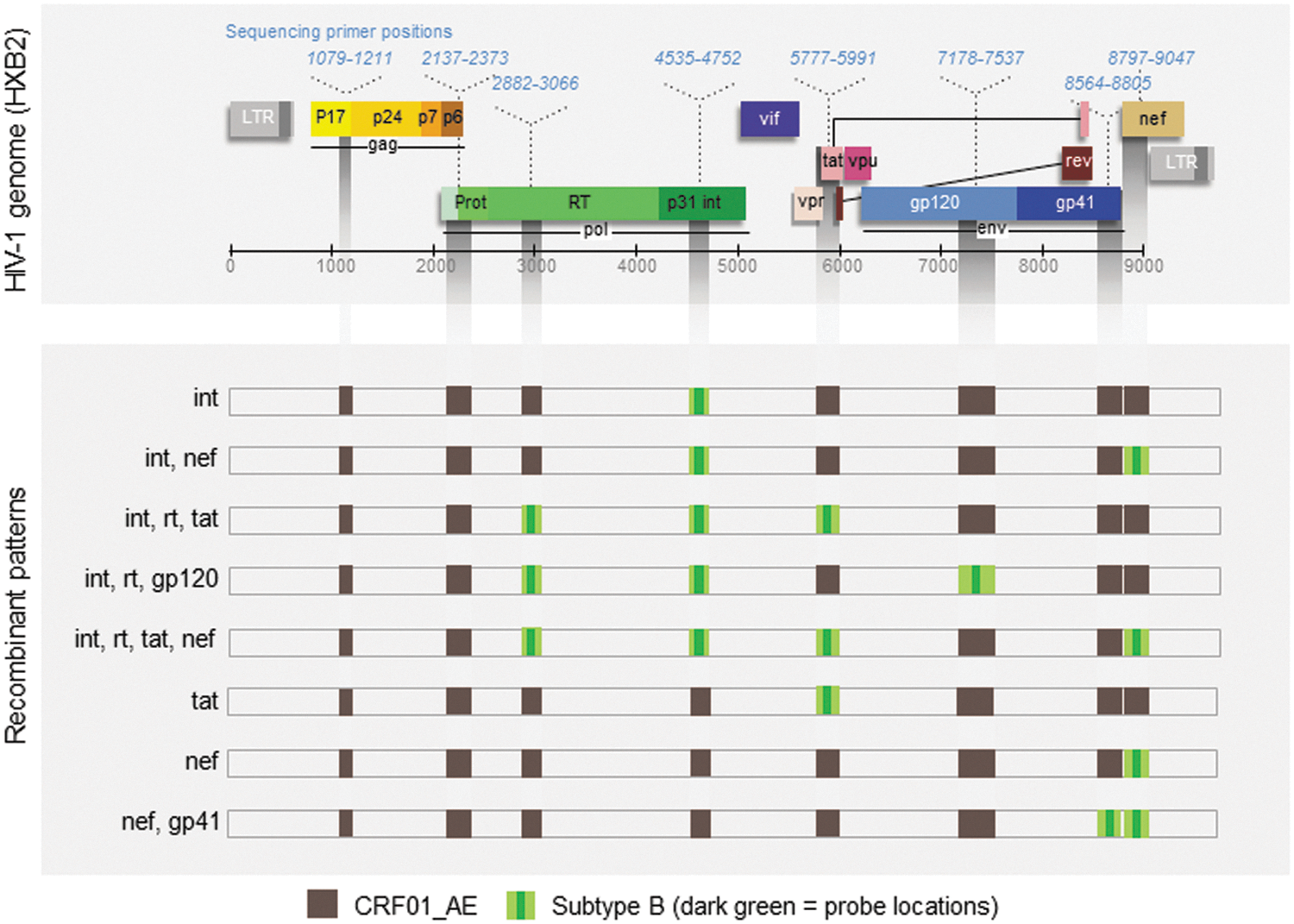
Multiplex hybridization assay approach and observed novel recombinants. Strain-specific probes permit characterization of HIV-1 subtype at eight genomic locations. Eight possibly novel patterns of recombination (horizontal bars) between CRF01_AE/B and HIV-1 subtype B were observed by the multihybridization assay (MHA) and confirmed by sequencing. Recombinant patterns consisted of a predominant CRF01_AE backbone (brown regions) with subtype B replacements (green regions) in various gene locations. Nucleotide positions for confirmatory sequencing are indicated relative to the HXB2 genome (blue numbering, top).
Trends in HIV-1 subtype distribution during 2006–2011
The distribution of identifiable HIV-1 subtypes was similar between seroprevalent and seroincident subjects. CRF01_AE was the most common while subtype B was the least common strain. Among seroprevalent infections, there was no significant temporal trend in subtype distribution from 2006 to 2008 (p>0.05). There was likewise no significant change in subtype distribution over 5 years of follow-up among seroincident subjects, although in each group there was some fluctuation in strain prevalence from year to year. We noticed a significant rise in the proportion of nontypeable strains among seroincident subjects, from 0% in 2006 to 11% in 2011 (p=0.02) (Table 1).
Discussion
Our study is the first to describe the molecular epidemiology of HIV-1 infection among Thai MSM in detail, and to characterize changes in subtype distribution over time. In this study, we report HIV-1 genotypes circulating among MSM in Bangkok from 2006 to 2011. The most common infecting viral strain was CRF01_AE, followed by recombinants involving CRF01_AE, subtype B and subtype C, HIV-1 subtype B, and dual infections. The distribution of viral strains was similar between seroprevalent and seroincident HIV-1 infections in our population. Dual infection was confirmed in 2% of the study participants. In this study, we observed several previously unreported patterns of recombination between CRF01_AE and HIV-1 subtype B. Lastly, we observed a significant increase in the proportion of nontypeable strains among HIV-1 seroincident subjects over the study period.
HIV-1 molecular genotyping has been conducted in Thai MSM in only one other study. 33 Arroyo et al. performed subtyping using MHAbce without confirmatory sequencing on specimens collected from 99 MSM attending HIV voluntary counseling and testing services in Bangkok between 2006 and 2007. 33 In these MSM, CRF01_AE was identified as the infecting strain in 75%, subtype B in 7%, and CRF01_AE/subtype B recombinants in 15%. The distribution of HIV-1 subtypes found in the present study are consistent with those of Arroyo et al. and provide a robust contemporary confirmation of this pattern in seroprevalent and seroincident MSM over an extensive sampling period. Both studies identified a high proportion of complex recombinant forms, and we note a significant rise in the frequency of nontypeable strains. Sequence analysis in nontypeable study subjects suggests that one reason for failure of MHA to provide subtype classification is the increasing divergence within probe binding regions over time (data not shown).
In the present study, we observed at least 11 distinct intersubtype recombinants. Most of these involved subtype B replacement within integrase on a CRF01_AE background, either alone or in combination with additional replacements within nef, tat, gp120, and rt (Fig. 2). One recombinant had a pattern similar to CRFs 55 (int, rt) while the others may be new unique recombinant forms (URF). CRF01_AE is a widely circulating strain prevalent in Southeast Asia generally thought to be a complex chimeric virus composed of subtype A and E parental subtypes, though this has been questioned.
40
The first recombinant between CRF_01AE and subtype B was identified in Thailand in 2003 (CRF15_01B), and was shown to be composed of a predominant CRF01_AE background with an HIV-1 subtype B segment within the viral env gene.
41
Several other CRF01/B recombinants have since been noted in Thailand
32
42
and other parts of Southeast Asia including CRFs33, 34, 48, 51, 52, 53, and 54 (
This analysis offers several strengths over previous studies. Our data were derived from a large and well-characterized longitudinal cohort study, including both seroprevalent and seroincident infections, and we performed targeted viral genetic sequencing in all cases in which results could not be unambiguously determined by sequence-specific hybridization methods. This study design eliminates the possibility of confounding due to repeat visits, and allows for robust characterization of epidemiological trends in our population. However, several limitations should also be considered. The gold standard for characterizing the subtype origins of an individual virus is full-length genomic sequencing, but this technique is currently not practical for larger studies. The probe-hybridization approach used here allows for high-throughput analysis but might fail to detect viral strains present at very low frequency or novel recombinant forms with short recombinant segments falling outside of the genomic regions studied. Although MHAbce has been designed to detect currently recognized viral strains circulating in Asia, 34 some specimens may have been misclassified due to nonspecific probe binding or failure to classify variant B strains. In addition, our study participants may imperfectly represent regional MSM populations due to self-selection leading to overrepresentation of men with characteristics associated with the outcomes studied here. For example, clustered HIV transmission events occurring within relatively closed local sexual networks may increase the apparent prevalence of certain HIV-1 genotypes. 44
During the early HIV-1 epidemic, HIV-1 subtype B′ predominated among intravenous drug users (IDUs) 30,45 whereas CRF01_AE infection was characteristic among those likely to have been exposed through sexual contact. 26,46 However, more recently an increasing number of infections with CRF01_AE and recombinant forms has been noted in all populations, with an associated decline in the proportion of subtype B infections. 27 –29,31,33,47 Other reports in the region have suggested similar shifts in favor of CRF01_AE over HIV-1 subtype B. In China, subtype B infections have declined dramatically from 90% in 2006 to only 20% in 2009, with a concomitant rise in the proportion of CRF01_AE from 4% to 50%. 48 –51 CRF01_AE also appears to have made a recent incursion into Japan, where HIV-1 infection had been nearly uniformly due to HIV-1 subtype B. 52
The reasons for this shift are unclear but could be related to subtype-specific differences in viral load during early infection 53 or behavior differences between risk groups. 13 The results obtained in our study suggest a continued trend toward a more complex epidemic with a rising number of recombinant forms and loss of pure subtype B infections. If these trends continue, we may anticipate a mature HIV-1 epidemic in the Asia-Pacific region in which CRF01_AE and complex CRF01_AE /B have displaced subtype B. These shifts will be of significance to efforts to develop regionally effective HIV prophylactic vaccines and other means of mitigating HIV transmission through epitope-specific immune responses.
Footnotes
Acknowledgments
The authors would like to thank the participants in this study, and acknowledge the support and funding from the U.S. military HIV-1 Research and the Henry M. Jackson Foundation. We also thank Viseth Ngauy, Vatcharin Assawadarachai, Kultida Poltavee, Hathairat Savadsuk, and Suwittra Chaemchuen of the Armed Forces Research Institute of Medical Sciences, Thailand for their support of this study; Sodsai Tovanabutra, Gustavo Kijak, Eric Sander-Buell, Morgane Rolland, Francine McCutcheon, and Jerome Kim of the U.S. Military HIV Research Program for their technical and intellectual input; Jaray Tongtoyai, Atittaya Sangiamkittikul, Punneeporn Wasinrapee, Natthaga Sakulploy, Kusuma Auethavoranan, and Wanna Suwanaphan of the Thai MOPH US–CDC Collaboration (TUC) laboratory for processing and testing all the samples; Sarika Pattanasin, Boonyos Raengsakulrach, and Chonticha Kittinunvorakoon for helpful advice; and the remaining members of our collaborative study group.
The findings and conclusions in this article are those of the authors and do not necessarily represent the views of the U.S. Centers for Disease Control and Prevention or the official policy of the Department of Army, Department of Defense, or the U.S. Government.
Presented in part at the following: (1) the 5th Conference on HIV Pathogenesis Treatment and Prevention, Cape Town, South Africa, July 19–22, 2009. Abstract number CDA053. Title: “High HIV-1 genetic complexity in men who have sex with men (MSM) in Bangkok, Thailand.” (2) The 18th International AIDS Conference, Vienna, Austria, July 18–23, 2010. Abstract number WePe0010. Title: “High HIV-1 genetic complexity in men who have sex with men (MSM) in Bangkok, Thailand.” (3) AIDS Vaccine 2011, Bangkok, Thailand, September 12–15, 2011. Abstract number P20.04. Title: “Characterization of HIV-1 subtype distribution among Thai MSM using MHAbce, a high throughput approach for molecular epidemiology studies.” (4) The 20th Conference on Retroviruses and Opportunistic Infections, Atlanta, GA, March 3–6, 2013. Abstract number I-120. Title: “HIV-1 subtype and disease progression in seroincident HIV infections among MSM in Thailand.”
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.