
Abstract
The purpose of this article is to describe mortality trends in different highly active antiretroviral therapy (HAART) periods and associated factors among AIDS patients in Guangxi, China. We prospectively analyzed AIDS patients in Guangxi between 2001 and 2011; demographic characteristics were compared among AIDS patients diagnosed in three treatment periods (pre-HAART: 2001–2004, early-HAART: 2005–2008, and late-HAART: 2009–2011). AIDS mortality was calculated by person-years, and treatment coverage was defined as the proportion of time that patients who were eligible for treatment received treatment. Factors of AIDS mortality were determined by a Cox proportional hazard regression. Of 19,020 AIDS patients, overall mortality declined from 41.1 per 100 person-years in 2001 to 13.3 per 100 person-years in 2011 with treatment coverage increasing from zero to 72.1%. The overall median survival figure was 5.6 years (95% CI: 4.4–6.8) with 60.3% for 5-year survival rate. After AIDS diagnosis, the mortality rate peaked in the first year, and 37.4% patients were still active in the ninth year. Protective factors for mortality were AIDS patients diagnosed from 2009 to 2011 (AHR=0.75, 95% CI: 0.58–0.89), having received HAART (AHR=0.71, 95% CI: 0.50–0.87), and having a CD4 count of higher than 350 cells/μl at AIDS diagnosis (AHR=0.79, 95% CI: 0.60–0.92). Risk factors for mortality included being male (AHR=1.28, 95% CI: 1.07–1.43), living in a rural area (AHR=1.40, 95% CI: 1.18–1.94), and being aged ≥60 years at AIDS diagnosis (AHR=1.36, 95% CI: 1.18–1.73). A decline in AIDS mortality was observed in Guangxi with a concomitant increase in treatment coverage. Some subpopulations of AIDS patients, such as males, rural residents, and the old, require more medical care.
Introduction
M
The first outbreak of HIV-1 infection was initially detected among injection drug users (IDUs) in Guangxi, which borders the drug-trafficking route known as the “Golden Triangle” 19 and serves to connect China with the Association of Southeast Asian Nations (ASEAN) countries. 20 The main route of HIV transmission in Guangxi shifted from IDUs during the period 1996–2005 to sexual transmission after 2005, and the AIDS epidemic began spreading from IDUs to other groups. 21 According to statistics from the Guangxi Center for Disease Prevention and Control (Guangxi CDC), there were at least 75,716 HIV/AIDS cases (51,062 HIV infections and 24,854 AIDS cases) in Guangxi in 2011, representing a 43.8% increase from 2009 (52,643 HIV/AIDS cases). The number of reported HIV/AIDS infections ranked second among 31 provinces in China.
Understanding mortality rates of AIDS patients is crucial for the assessment of the advantages and weaknesses of national HIV programs. Some cohort studies were previously conducted in parts of areas in China such as Shanxi, 22 Hunan, 23 and Wuhan 24 to reveal mortality rates among AIDS patients. However, the studies did not report the mortality trends with a concomitant increase in treatment coverage, and their study populations were small. Studies assessing mortality have never been conducted in Guangxi and, in addition, Guangxi belongs to the Zhuang autonomous region; whether the Zhuang population may have higher AIDS mortality rates in Guangxi was not studied before. A retrospective cohort study, therefore, was conducted among adult patients with AIDS in Guangxi to objectively and entirely assess mortality trends with increasing antiretroviral treatment coverage and assess the association between AIDS mortality and factors including individual characteristics, diagnosis time, treatment status, and CD4 levels at AIDS diagnosis.
Materials and Methods
Ethics statement
This study was reviewed and approved by the Institutional Review Board of the Institute for HIV/AIDS Control and Prevention, Guangxi CDC. All patients signed informed consent forms upon being initiated into the NFATP program. Because data used in this study were from a secondary analysis using an existing routine Guangxi HIV/AIDS surveillance program and the regular administration of the HAART program, no additional study-specific consent for this current study was sought.
Study design and population
All HIV-positive individuals in China are reported to the National Center for AIDS/STD Control and Prevention, China CDC. 25 Baseline data from these individuals, including demographic characteristics, the date of diagnosis, the route of HIV infection, and CD4 count at first diagnosis and at every 6-month follow-up, are recorded in the national HIV epidemiology database. HIV-positive individuals who meet the Chinese national treatment criteria (having AIDS or a WHO disease at stage 3 or 4 or a CD4 count of less than 350 cells/μl) are referred for treatment with a standard three-drug therapy; the subsequent treatment outcomes are recorded in the national HIV treatment database. 25 –27
We obtained data from AIDS patients in Guangxi from the national HIV epidemiology and treatment databases and prospectively analyzed mortality rates among this population from January 1, 2001 to December 31, 2011. AIDS patients were defined with reference to the 1993 clinical criteria of the CDC of the United States. 28 In this study, AIDS patients aged ≥15 years, with confirmed survival time and at least one additional follow-up CD4 count test, were included, while patients with inconsistent or missing key data were excluded (Fig. 1). AIDS patients included in the final analysis were sorted as either active (last contact within the past year), dead, or lost to follow-up (last contact over 1 year ago) by the end of 2011. One year was selected to classify active patients as opposed to those lost to follow-up. 29 Three treatment periods were grouped according to the date the AIDS diagnosis was given (pre-HAART: 2001–2004, early- HAART: 2005–2008, and late-HAART: 2009–2011).
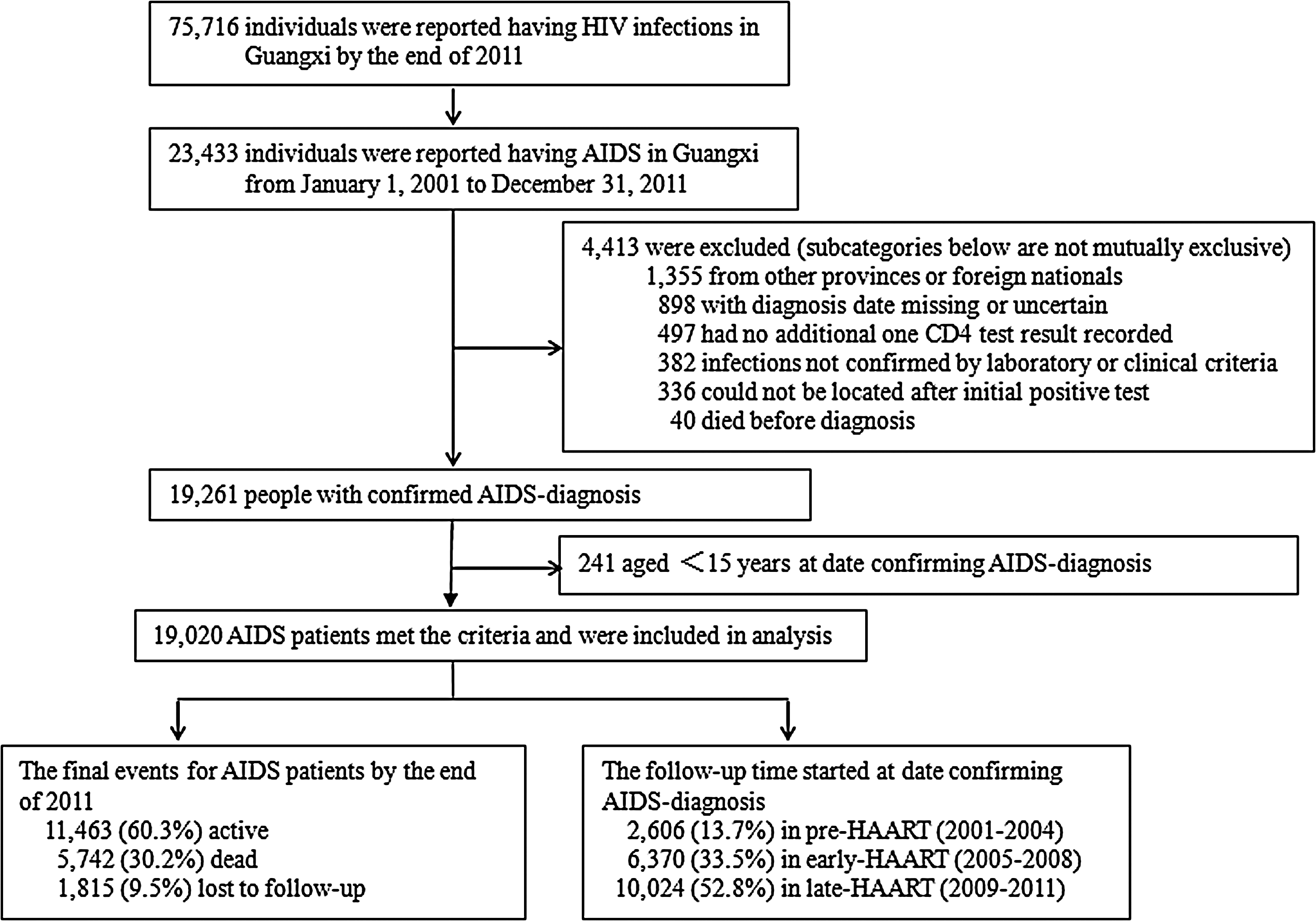
Study flowchart.
Treatment coverage was defined as the proportion of person-years spent on HAART from the treatment-eligible date to last contact and expressed as a percentage of person-years. The linkage between the treatment database (the numerator) and the epidemiology database (the denominator) was used according to the individuals' national identification numbers or unique treatment numbers. A total of 2,355 patients could not be linked. Of them, 1,470 patients in the treatment database could not be linked to the epidemiological database and 985 patients in the epidemiological database could not be linked to the treatment database. To correct the underestimation of the numerator caused by unlinked personal information in the two databases, treatment coverage was calculated by taking the midpoint between the proportion of linked individuals that the numerator included (presumes that all unlinked individuals were treatment naive) and the proportion of all unlinked individuals that the numerator included (presumes that all individuals were treated). 11,30
Data analysis
Characteristics within three periods were compared with a chi-squared test for categorical variables, the Wilcoxon test for continuous variables, and a Poisson distribution to exact 95% confidence interval (CI) values. According to the calendar year, the proportion of mortality was calculated by the number of deaths and the sum of person-years for those who were diagnosed with AIDS in that year. The patients who received treatment and were lost to follow-up or died at any time within the year were calculated as half a person-year, and the rest were calculated as one person-year. The number of person-years for each individual receiving HAART was calculated using the same approach. Risk factors for mortality were determined by a Cox proportional hazards regression with patients still active or lost to follow-up on December 31, 2011 censored. The calendar year of follow-up (2001–2004, 2005–2008, and 2009–2011) was fitted as a time-dependent covariate to test the change in AIDS mortality over time. Significance was defined as a level of 0.05 (two-tailed), and statistical analyses were performed with SPSS version 16.0.
Results
Demographic characteristics of AIDS patients
The study cohort was composed of 19,020 AIDS patients with a mean observation duration of 2.1 years (SD=1.6, range 0–10.5) and a median CD4 count of 197cells/μl (IQR: 81–343) at AIDS diagnosis. The majority of subjects were males (75.1%), farmers (60.2%), and of the Han ethnic group (66.2%). Participants ranged in age from 16 to 85 years (median=38.0, IQR: 30–53). In total, 57.8% of the participants came from urban areas and 42.2% from rural areas; most of them had a primary school education (50.0%), followed by secondary school (31.8%) and no schooling (14.3%), and the rest had postsecondary schooling. Of all participants, 29.0% reported never having been married, 60.2% were married or cohabitated, and 10.8% were divorced, separated, or widowed. Of participants, 56.9% reported being infected by heterosexual contacts and 33.9% from injection drug use, 6.6% reported other transmission routes (blood or plasma transfusion, MSM or maternal), and 2.9% reported the cause as unknown (Table 1). Because of an increased emphasis on early diagnosis and treatment among HIV-1-positive individuals in China in recent years, 10,044 (52.8%) patients included in the analysis were identified from 2009 to 2011.
Heterosexual intercourse refers to intercourse between opposite sex only.
IQR, interquartile range; HAART, highly active antiretroviral treatment.
The demographic characteristics of the AIDS patients from the three periods were similar in terms of ethnic group, marital status, occupation, and education, but also had some significant differences (Table 1). The AIDS patients in the last period were generally older than those in earlier periods and were predominantly infected by heterosexual contacts. This group also had a higher proportion of females and rural residents and higher CD4 counts at AIDS diagnosis.
Mortality in AIDS patients
Between 2001 and 2011, 5,742 deaths were identified in 40,096.6 person-years of follow up. Of the deaths, 3,762 (65.5%) could be ascribed to AIDS-related causes, 1,618 (28.2%) to non-AIDS-related causes, and 362 (6.3%) were unknown. The overall mortality rates of AIDS patients declined from 41.1 per 100 person-years (95% CI: 38.3–43.9) in 2001 to 13.3 per 100 person-years (95% CI: 9.6–17.0) in 2011 with treatment coverage concomitantly increasing from zero to 72.1%. Mortality rates in AIDS patients receiving HAART increased between 2004 and 2005 (when NFATP was initiated) and then decreased steadily in subsequent years (Fig. 2). When stratified for the HAART period during which AIDS diagnosis was given, the mortality rate declined from 12.7 per 100 person-years (95% CI: 11.3–14.1) in the pre-HAART period to 8.5 per 100 person-years (95% CI: 6.6–10.4) in the early-HAART period (p<0.0001), which further declined to 5.3 per 100 person-years (95% CI: 4.5–6.1) in the late-HAART period. When compared with the pre-HAART period, the adjusted hazard ratio (AHR) for AIDS mortality was 0.67 (95% CI: 0.56–0.78) for the early-HAART period and 0.48 (95% CI: 0.41–0.55) for the late-HAART period (Fig. 3).

Mortality and midpoint treatment coverage for newly diagnosed patients with AIDS by year. Color images available online at
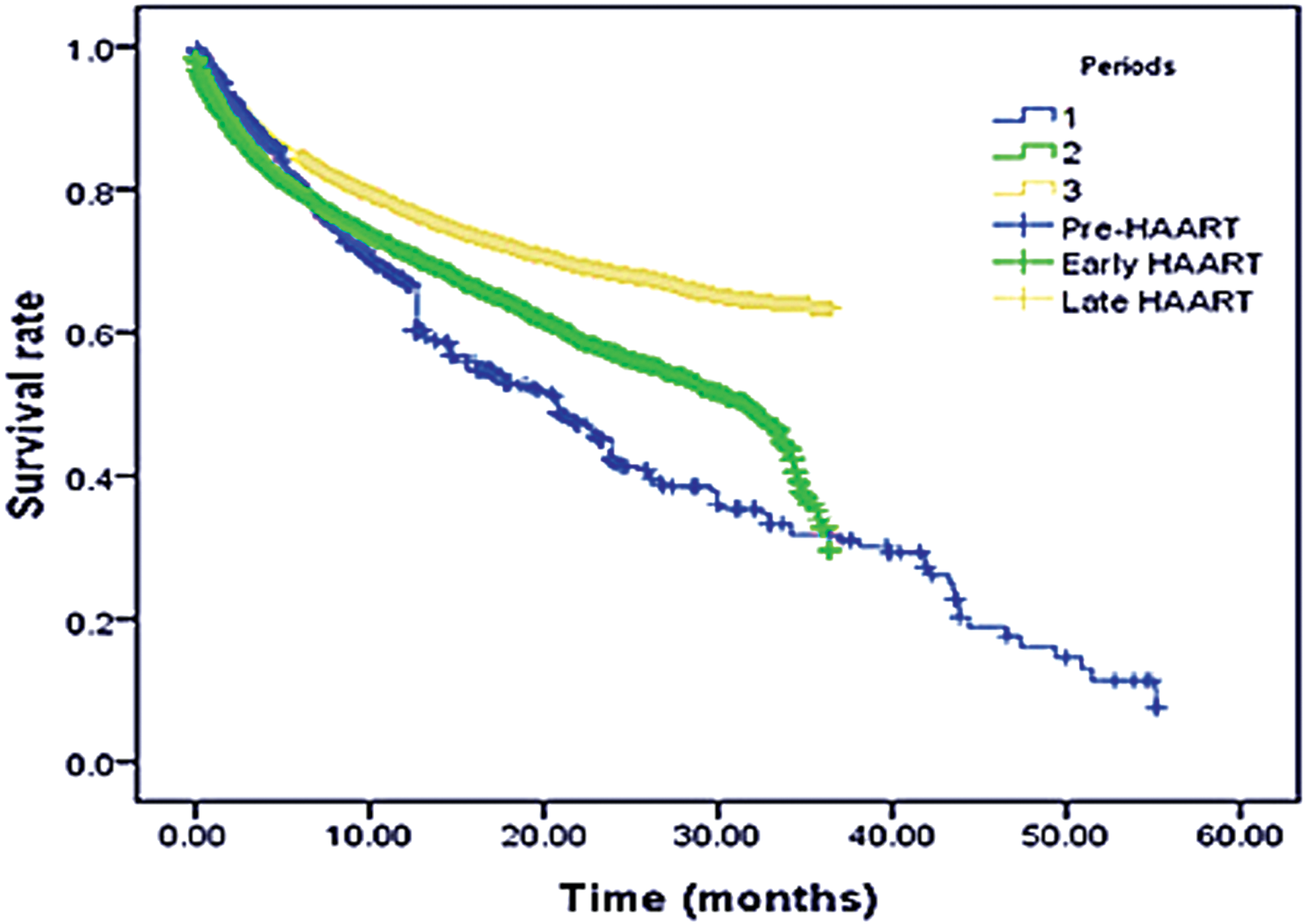
Kaplan–Meier survival plot for AIDS patients diagnosed from each highly active antiretroviral therapy (HAART) time period. Color images available online at
When stratified for causes of death, the mortality rate for AIDS-related deaths (9.4 per 100 person-years, 95% CI: 7.5–11.3) was significantly higher (p<0.0001) than that for non-AIDS- related deaths (4.0 per 100 person-years, 95% CI: 2.5–5.5). The main cause was opportunistic infection (51.2%), including tuberculosis, bacterial pneumonia, and sepsis. But the proportion of non-AIDS-related deaths increased from 18.7% in the pre-HAART period to 34.2% in the late-HAART period with the most likely causes of death being viral hepatitis B or C (39.4%), associated cancers (15.3%), and cardiovascular diseases (14.1%).
Survival time of AIDS patients
Results of life-table analysis showed that the overall median survival time of AIDS patients was 5.6 years (95% CI: 4.4–6.8). The 5-year survival rate was 60.3% (95% CI: 52.0–68.6). When stratified by treatment status, the median survival time of treatment-naive patients was 14 months (95% CI: 12.8–15.2) and that of treated patients was 6.4 years (95% CI: 5.0–7.8) with 73.4% (95% CI: 70.2–76.6) for the 5-year survival rate. After AIDS diagnosis, a peak of the mortality rate was seen in the first year, and 37.4% patients were still active at 9 years (Fig. 4).

Mortality and survival rate by years after AIDS diagnosis. Color images available online at
Factors associated with AIDS mortality
Univariate and multivariate Cox hazard regression analysis showed no significant difference in terms of ethnic group, marital status, occupation, education, and HIV infection routes on AIDS mortality. However, the mortality rate of the AIDS patients diagnosed from 2009 to 2011 was significantly lower than that of those diagnosed from 2001 to 2004 with an overall 25% reduction in the risk of AIDS mortality (AHR=0.75, 95% CI: 0.58–0.89). The other two protective factors related to AIDS mortality were having received HAART (AHR=0.71, 95% CI: 0.50–0.87) and having a CD4 count higher than 350 cells/μl (AHR=0.79, 95% CI: 0.60–0.92) at AIDS diagnosis. The factors associated with higher mortality included being male (AHR=1.28, 95% CI: 1.07–1.43), living in a rural area (AHR=1.40, 95% CI: 1.18–1.94), and being aged ≥60 years at AIDS diagnosis (AHR=1.36, 95% CI: 1.18–1.73) (Table 2).
HR, hazard ratio; AHR, adjusted hazard ratio.
Discussion
Our study showed that with a concomitant increase in antiretroviral treatment coverage, the overall mortality rate among AIDS patients declined from 41.1 per 100 person-years in 2001 to 13.3 per 100 person-years in 2011. The rate was comparable to mortality rates among HIV individuals who were eligible for HAART in China overall (14.2 per 100 person-years), 11 while much higher than for mortality rates among HIV-infected cases on HAART in Europe (4.1 per 100 person-years) 31 and the United States (8.8 per 100 person-years). 32 All of these findings show the beneficial role of HAART and increased treatment coverage in diminishing both HIV and AIDS-related mortality. Nevertheless, under the 2013 WHO guidelines, HIV treatment coverage in low- and middle-income countries represented only 34% (32–37%) of the 28.6 million eligible people in 2013. 33 Our study estimated that the treatment coverage of Guangxi AIDS patients reached 72.1% in 2011, which was lower than the reported treatment coverage in Cambodia (90%) 34 and Lusikisiki (95%), 35 based on results of studies of HIV patients who were registered in hospitals or health care clinics.
In view of better access to HAART and fewer losses to follow-up being observed in patients who registered in a hospital, 34,35 China began piloting a one-stop service program to deliver HIV testing and treatment through hospitals in two counties of Guangxi in 2013. This has allowed the time from screening to treatment to be shortened to an average of 11 days, compared with an average of 8 weeks before this program, with treatment coverage reaching 90% (Guangxi CDC, unpublished data, 2013). Therefore, scaling up this new approach in local hospitals may be helpful to increase the percentage of treatment coverage among treatment-eligible patients in Guangxi in the future.
We reported that the overall median survival of AIDS patients was 5.6 years, which is obviously longer than the natural median survival time of disease progression (0.9–2.4 years) for those who were treatment naive. 36 Stratified by treatment status, the median survival time of treated patients (6.4 years) was much higher than that of treatment-naive patients (14 months), but the 5-year survival rate (73.4%) was lower than that for a cohort in Brazil of AIDS patients with treatment (82.0%). 6 Several important points are considered in interpreting the fact that mortality is greatest in the first year after AIDS diagnosis. First, in line with standard development, since Guangxi reported the first native HIV infection in 1996, 21 HIV/AIDS cases should have reached peak rates of morbidity and mortality in recent years. Second, almost half of the patients had absolute CD4 counts below 50 cells/μl, meaning severe immune deficiency at HAART initiation. Lastly, the Guangxi provision of NFATP to HIV-infected patients as a public service began in late 2004, much later than the case for western countries where access to HAART began in 1996. 37
Research in China and other countries 4,38 –41 has identified a drop in the proportion of deaths from AIDS-related diseases and an increase in non-AIDS-related diseases among HIV/AIDS cases, expanding with antiretroviral treatment coverage. The most likely causes of non-AIDS-related deaths were viral hepatitis B or C, 38 associated cancers, 39,40 and cardiovascular diseases. 41 Our data are in accord with the results of these studies. The fact that international bodies have not formulated a specific definition and classification for the causes of AIDS deaths in China and that there has been limited data collection on HIV/AIDS deaths in China indicates that further analyses need to be done on whether non-AIDS-related deaths might also arise more frequently in Guangxi after the better method of CODE for HIV/AIDS deaths reported in foreign countries 42 is applied nationwide.
A previous study reported that with the use of HAART, better survival was observed in patients diagnosed with AIDS after 1996 than before. 16 Similarly, compared with AIDS patients diagnosed from 2001 to 2004, lower mortality rates were observed in those diagnosed from 2009 to 2011 in our study. Consistent with relative studies, 17,18 having received HAART and having a high CD4 count at AIDS diagnosis were found to be strongly correlated with AIDS mortality. Our results confirmed that earlier initiation of antiretroviral treatment and increased treatment coverage are remarkable factors to lower AIDS mortality. Other factors associated with higher AIDS mortality in our study included being male, being aged over 60 years at AIDS diagnosis, and living in a rural area.
As opposed to other studies that have shown that there was no difference between females and males in AIDS survival, 12,43 or that females have a shorter survival rate for AIDS than males, 44 our study showed that female patients had an overall 28% reduction in the risk of AIDS mortality as compared to male patients. Additional research should, thus, explore this discrepancy between the results of different studies. With a few expectations, we had hypothesized that socioeconomic AIDS mortality inequalities should have narrowed after HAART was free of charge for all patients due to the existence of NFATP, but AIDS patients living in rural areas had a higher mortality than those from urban areas. Potential explanations may involve AIDS patients from rural groups having a lack of access to treatment despite its being free 45 or having more difficulties adhering to the long and complex treatment. 46 Although the reasons for the differences in AIDS mortality between rural and urban groups still remain unclear in Guangxi, the administration of HAART therapy to poor populations should be considered when implementing preventive and treatment strategies. Our study found that patients aged ≥60 years at AIDS diagnosis constituted a group with a greater vulnerability for mortality, owing to a rise in comorbidity with the time delay of treatment 47 and a weaker immune response to antiretroviral drugs. 48 Therefore, efforts in large-scale HIV screening to identify substantially more individuals with undiagnosed HIV and to adopt earlier treatment for eligible patients are crucial in enhancing care for all people living with HIV/AIDS.
Our study has several limitations. First, the median duration of follow-up was fairly short (2.1 years) due to the fact that more than half of the participants included were identified in the previous 2 years (2009–2011). Further studies should be taken into account to confirm the long-term durability of the treatment protectiveness. Second, we failed to link all of the treated patients with the epidemiology database and could, therefore, have underestimated treatment coverage, particularly for individuals who were infected sexually or by injection drug use. As such, comprehensive treatment coverage for the entire infected population of Guangxi needs to be verified by additional studies. Third, the definition and classification of the causes of AIDS deaths are not standardized and are unclear in China at present; this leads to a certain number of flaws and limitations in the analysis of causes of deaths in our study. Finally, our results were based on observational data, and, thus, have inherent biases. For example, the female AIDS cohort had an associated survival bias. One reason for this is that the males who infected them had AIDS much earlier when access to treatment was limited. The other reason is that more HIV-infected males were infected through injection drug use, while this population has a low treatment coverage of 75.4% in Guangxi (Guangxi CDC, unpublished data, 2013).
A decline in the overall mortality was observed among the Guangxi AIDS patients with a concomitant increase in antiretroviral treatment coverage. Guangxi needs to strengthen its HIV screening to identify more undiagnosed HIV individuals and to adopt earlier treatment for eligible patients before they become severely immune suppressed. Because some subpopulations of AIDS patients, such as males, rural residents, and the old, require more medical care, the pattern of the causes of AIDS deaths should be continually monitored when implementing HAART.
Footnotes
Acknowledgments
The authors thank staff members who have been involved in the surveillance, laboratory testing, and treatment of HIV/AIDS patients in Guangxi. We also thank Zhenzhu Tang and Zhiyong Shen at Guangxi CDC, Nanning, for their generous support of this study. This study was supported by the Mathematical Epidemiology Studies for HIV/AIDS in Guangxi under Health and Family Planning Commission of Guangxi Zhuang Autonomous Region (grant S201310-06).
Author Disclosure Statement
No competing financial interests exist.