
Abstract
Dizziness is a symptom in human T cell lymphotropic virus type-associated myelopathy/tropical spastic paraparesis (HAM/TSP) and may occur due to vestibulospinal tract dysfunction. This tract can be assessed by an electrophysiological test called vestibular-evoked myogenic potential (VEMP). The aim was to correlate the result of VEMP generated by acoustic stimuli and dizziness in individuals with human T cell lymphotropic virus type 1 (HTLV-1)-asymptomatic infection and HAM/TSP. VEMP was recorded from the sternocleidomastoid muscle of 60 HTLV-1-negative adults (60±8 years) and 60 individuals infected with HTLV-1, 30 being asymptomatic (59±8 years) and 30 with HAM/TSP (59±8 years). In all groups, 90% of the participants were women. VEMP was generated by acoustic stimuli (short tone bursts), with an intensity of 118 dBHL and band-pass filter from 10 Hz to 1,500 Hz, and presented 200 stimuli at a frequency of 1,000 Hz with a record time of 60 ms. Of 60 HTLV-1-negative individuals, 14 (23%) reported dizziness; VEMP was normal in all. In the HTLV-1-asymptomatic group, 11(37%) complained of dizziness (p=0.31); VEMP was altered in four (40%) subjects with dizziness and in one (5%) without dizziness (p=0.00). In the group with HAM/TSP, dizziness was reported by 17 (57%) subjects (p=0.002); VEMP was altered in 11 (64%) with dizziness and in 5 (38%) without dizziness (p=0.15). Dizziness without an apparent etiology in HTLV-1-asymptomatic carriers deserves attention in terms of a possible subclinical spinal cord involvement that can be clarified through spinal electrophysiological tests. Damage of the vestibulospinal tract seems to occur in the early stages of HAM/TSP.
Introduction
H
The aim of the present study was to compare the complaints of dizziness with the results of VEMP generated by acoustic stimuli in individuals with HTLV-1-asymptomatic infection and individuals with HAM/TSP, using a matched group by age and gender of healthy and HTLV-1-seronegative individuals.
Materials and Methods
Ethical aspects
Approval was obtained by the Ethics Committee of the Federal University of Minas Gerais, number 0437.0.203.000-10, and the Ethics Committee of the Hemominas Foundation, number 290. All participants gave voluntary written consent and declared they were aware of the procedures and their freedom to participate.
Subjects
The Interdisciplinary HTLV Research Group (GIPH) studies the natural history, the clinical manifestations, and the epidemiological aspects of HTLV infection. 10,11 This group has been following individuals infected with HTLV since 1997 in the state of Minas Gerais, Brazil, in an open cohort. As part of the cohort, over 637 HTLV-infected and 232 noninfected individuals were enrolled. 11
The present study is a transversal evaluation of 120 participants in the GIPH cohort. 2,11 The participants were randomly selected from the list of individuals enrolled in the cohort. The HTLV-1-seropositive participants fulfilled the criteria of either being asymptomatic carriers or having HAM/TSP. 12 The individuals were invited to participate by telephone for the HTLV-1-seropositive group and by personal contact before blood donation for the HTLV-1-seronegative group.
The participants were 60 healthy blood donors and 60 infected with HTLV-1. The latter group consisted of two subgroups, according to the Expanded Disability Status Scale (EDSS) 13 and OSAME scale 14 : 30 HTLV-1-asymptomatic carriers, from a neurological point of view (EDSS and OSAME – 0 in both scales) and 30 with a definite diagnosis of HAM/TSP (EDSS and OSAME greater than 2 on both scales). The 60 individuals noninfected with HTLV-1 were matched by gender and age with the individuals of the groups infected with HTLV-1.
HTLV-1 diagnosis
All the participants were submitted to serological screening for blood-borne pathogens, regularly applied in blood centers. The HTLV-1 infection in blood was based on two positive examinations using different samples. The individuals with a reactive HTLV screening test (enzyme-linked immunosorbent assay, ELISA, Bio-Rad, USA) were tested by Western blot (WB-MP Diagnostics, Singapore); those with any other positive results in the screening tests were excluded. 10
Study design
The study was a sectional analysis of the GIPH cohort. The risk factor was HTLV-1 infection and the dependent variables were manifestations of dizziness and VEMP analysis. All participants underwent a medical interview concerning their general health status and otoneurological manifestations and were evaluated by the otolaryngologist, neurologist, and audiologist and submitted to specific tests to exclude any clinical cause of dizziness. 15 –17
All the participants underwent VEMP and all the individuals with dizziness were submitted to a clinical and otoneurological examination along with specific examinations in order to clarify the causes related to peripheral labyrinth disease and related to neurological, psychiatric, cardiovascular, endocrinological, and orthopedic diseases that may present dizziness. 16
Vestibular-evoked myogenic potential
VEMP testing has been used to evaluate diseases related to the peripheral vestibular system, mainly the saccule and its afferents. 18 This evoked potential is activated by either sound or galvanic stimulation and both stimuli trigger the vestibulospinal myogenic reflex. 9,18 The pathways of VEMP activated by sound are the saccular macula in the internal ear, the inferior vestibular nerve, the medial vestibular nucleus in the brainstem, the vestibular spinal descending pathways, and finally the motor neurons of the ipsilateral sternocleidomastoid muscle. 19 As the neural pathway includes the vestibulospinal tract, this testing can also be used to evaluate the integrity of the spinal cord. 20
The VEMP response consists of two waves of reversal polarity at 13 ms and 23 ms. 21 The first wave is positive (P13) followed by a second negative wave (N23). 21 The changes of the amplitude are the most reliable measure to evaluate diseases of the internal ear 22 and the prolonged latency, mainly of P13, can be found in central disturbances. 23
The use of VEMP in the evaluation of patients with HAM/TSP has previously been described. 6,8,9 In the present study, high-intensity sound was used to activate the reflex, and the response was recorded by surface electromyography electrodes on the sternocleidomastoid muscle. 18,19,21 The eletromyographic (EMG) activity was recorded from the upper half of the sternocleidomastoid (SCM) muscle using surface electrodes, with a reference on the upper sternum and a ground electrode on the forehead. 9,20 During each recording session, in seated position, the subject was instructed to rotate the head toward the contralateral side of the tested ear to keep the SCM muscle under tension (Fig. 1). VEMP was generated by acoustic stimuli (short tone bursts), with an intensity of 118 dBHL and band-pass filter from 10 Hz to 1,500 Hz, was presented 200 stimuli at a frequency of 1,000 Hz with a record time of 60 ms, and the electromyographic signals were amplified (model MASBE/ActPlus, Contronic, BR). The response was recorded from the SCM muscle on each side. The examination was replicated to confirm the eletrophysiolological origin.

Technical execution of vestibular-evoked myogenic potential (VEMP): ear phones and electrode position. GE, ground electrode; AE, activity electrode on sternocleidomastoid muscle; R, reference electrode on sternum.
Data analysis
The analysis of VEMP results was masked and was done by two examiners in a blind way. The measured parameters were the peak latency of the two waves P13-N23. 19,21 The accepted variation of normality was two standard deviations of P13-N23 values of the uninfected group, which was latency ≤15 ms for P13 and ≤26 ms for N23.
The results of VEMP were classified as normal (Fig. 2A) or abnormal (Fig. 2B and C). The abnormal VEMP showed either prolonged latency (Fig. 2B) or undetectable response (Fig. 2C). The results of VEMP were compared with the complaint of dizziness for each group (HTLV-1 asymptomatic, HAM/TSP, and healthy individuals).
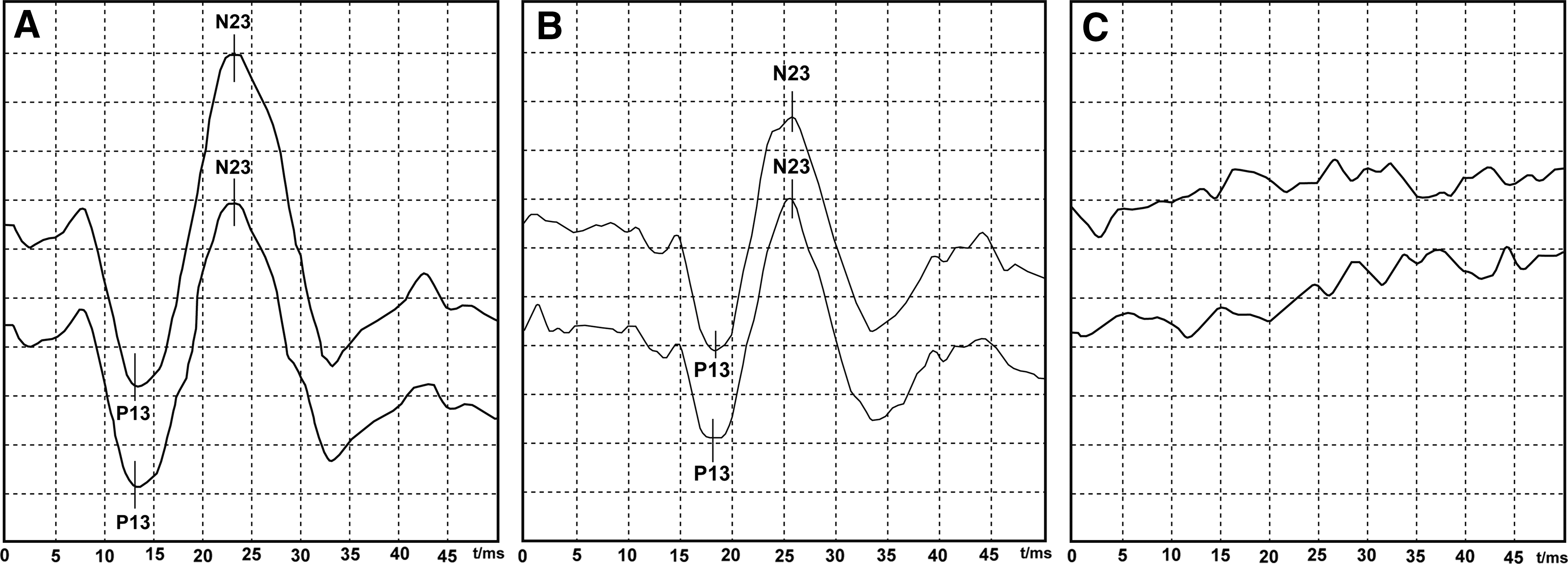
Examples of tracings obtained by vestibular-evoked myogenic potential (VEMP) recorded from the sternocleidomastoid muscle.
The statistical analysis was performed using the Statistical Package for Social Sciences, version 18.0 for Windows, SPSS (Chicago, IL). The between-groups comparisons for continuous variables were made through the Mann–Whitney test or t-test. The between-groups comparisons for categorical variables were made through the Qui-square Pearson test or Fisher test when samples with small frequencies were used. In the cross-analysis of correlations, a significance level of 5% (error type I) was considered and a power of 80% (type II error). Aiming at the magnitude of the association between exposure to the risk factor and the dependent variables, the prevalence ratio (PR) was calculated. The confidence interval (95%) was calculated in order to evaluate the sample variability.
Results
Among the 60 individuals uninfected with HTLV-1 (controls), the mean age was 60±8 (SD) years. Among the HTLV-1-infected individuals, the mean age was 59±8 years for the 30 asymptomatic carriers and 59±8 years for the 30 with HAM/TSP (p=0.733). In all groups, 90% of the participants were women.
In the uninfected group, VEMP was found to have the same pattern of wave for all individuals (Fig. 2A). In the HTLV-1-infected group, the most common pattern was prolonged latency for the asymptomatic group and undetectable response and prolonged latency for the HAM/TSP group.
In the HTLV-1 asymptomatic group, VEMP was abnormal in 5/30 (17%) participants. The characteristic of abnormal response was prolonged latency. In the HAM/TSP group, VEMP was abnormal in 16/30 (53%) participants. A prolonged response was observed in 12/16 (75%) participants and an undetectable response in 4/16 (25%) participants.
Figure 3 shows the frequency of dizziness in each group. Of 60 HTLV-1-uninfected individuals, 14 (23%) reported dizziness; VEMP was normal in all. In the HTLV-1-asymptomatic group, 11/30 (37%) complained of dizziness (p=0.31); VEMP was altered in 4/11 (40%) subjects with dizziness and in 1/19 (5%) subjects without dizziness (p=0.00). In the group with HAM/TSP, dizziness was reported by 17/30 (57%) subjects (p=0.002); VEMP was altered in 11/17 (65%) subjects with dizziness and in 5/13 (38%) subjects without dizziness (p=0.15).
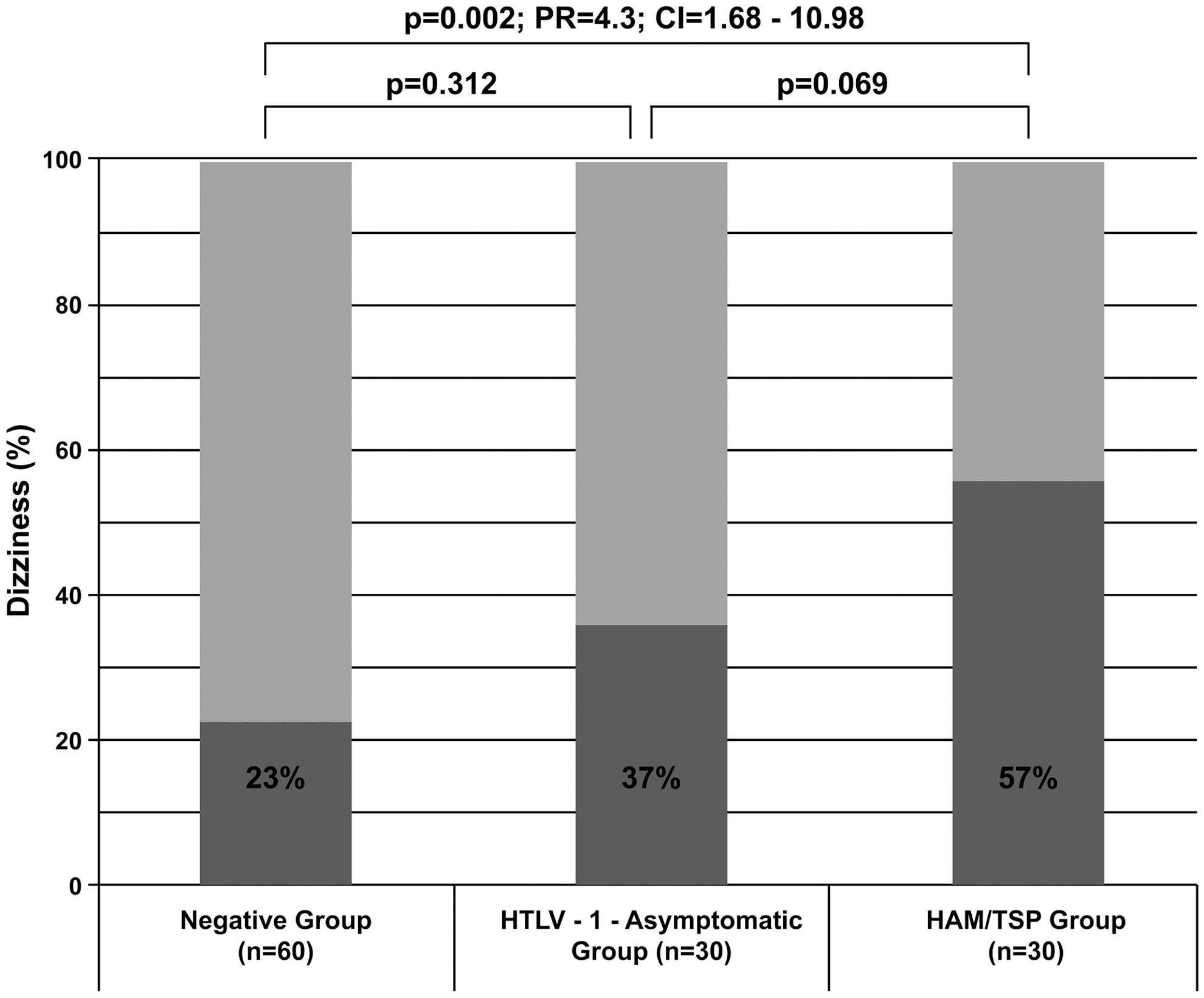
Dizziness among the groups: HTLV-1-asymptomatic carrier, HAM/TSP, and uninfected individuals. N=120. Light gray box, absence of dizziness; dark gray box, presence of dizziness; n, number of participants; PR, prevalence ratio; CI, confidence interval; p, p-value (Chi-Square test or Fisher's Exact test).
Figure 4 shows the comparison of VEMP latency among the groups with and without dizziness. The participants with undetectable response were not plot in the figure and the statistical significance was reached considering the results in which latency was record. The results show that the latency of VEMP was higher in HTLV-1-asymptomatic (p=0.02) and HAM/TSP groups with dizziness (p=0.03).
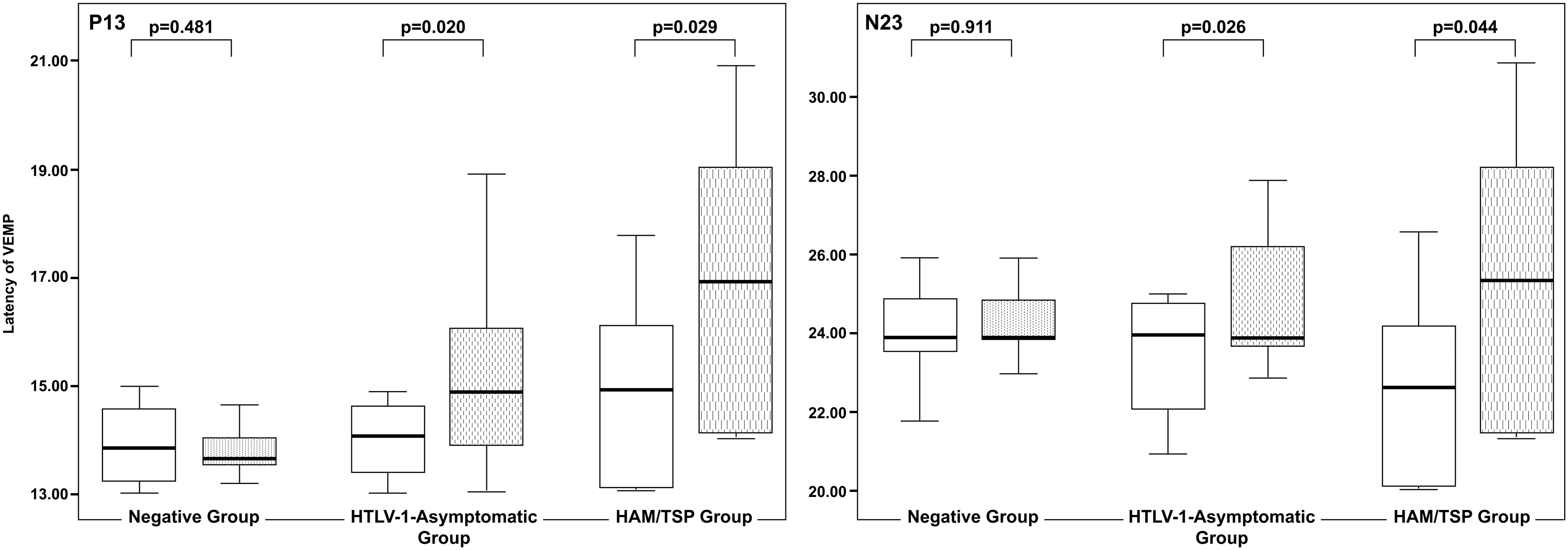
Comparison of the vestibular-evoked myogenic potential (VEMP) latency among the groups: HTLV-1 uninfected, HTLV-1-asymptomatic carrier, and with HAM/TSP. N=120. Blank box, individuals without dizziness; dashed box, individuals with dizziness; p, p-value (Mann–Whitney test).
Discussion
In HTLV-1-endemic areas, HTLV-1 seroprevalence increases with age and is higher in women than in men. 11,24 The increase of prevalence with age may be explained by the accumulation of seroconversions over the lifetime; the higher prevalence in females may be due to a more efficient male-to-female transmission during sexual intercourse. Hormonal effects may also play a role in female susceptibility. 24
In the present study, the frequency of dizziness was approximately four times higher in those with HAM/TSP compared to the HTLV-1-seronegative individual. Interestingly, for the HTLV-1-asymptomatic carriers, the complaint of dizziness was similar in frequency when compared to the general population in which this symptom is mentioned by 20% to 30% of individuals aged 60 years. 25
The normal balance takes for granted the correct interaction of the vestibular mechanisms with the visual perception and with the proprioception. 20 The lesion or dysfunction of any of these mechanisms can trigger disturbances in balance control. 16,17 Dizziness presented as vertigo is usually related to the impairment of unilateral peripheral vestibular pathways while instability is more commonly related to direct or indirect damage of CNS vestibular projections, including the vestibulospinal tracts. 17 Characteristically, HAM/TSP affects the motor tracts and tracts nearby, including the vestibulospinal and reticulospinal tracts. 26
The complaint of dizziness was shown to be mentioned early in the spectrum of the neurological symptoms related to HAM/TSP. 7 In the present study, the electrophysiological examination of the vestibulospinal tract through VEMP showed altered responses in the HTLV-1-infected individuals with dizziness either with HAM/TSP or asymptomatic carriers. The stronger statistical association between the complaint of dizziness and the altered VEMP in the group of HTLV-1-asymptomatic carriers emphasizes the value of this symptom as a possible neurological manifestation related to incipient damage of the vestibulospinal tract.
Individuals with HAM/TSP complain more frequently of dizziness than individuals with other nontraumatic myelopathies, as, for example, in schistosomiasis myeloradiculopathy. 27 The difference in the pathophysiology explains the higher occurrence of dizziness in HAM/TSP, while the damage of the motor tract in the schistosomiasis myeloradiculopathy is due to the parasite's eggs obstruction of the inferior spinal vascular system, which causes a well-delimitated inflammation. 28 In HAM/TSP, the damage of the spinal cord is due to the predominance of inflammatory cytokines and chemokines in the spinal cord causing damage to the motor tract and nearby areas. 24 Although the focus of the damage is the inferior spinal cord, all the neuroaxis is affected. 23
The morphological alterations related to HAM/TSP allow speculative explanations about the cause of the dizziness. 5,24 HAM/TSP is an inflammatory myelopathy that predominates at the descending spinal pathways. The damage of the reticulospinal and the vestibulospinal tracts, both related to balance control, may explain the high frequency of dizziness in individuals with HAM/TSP. 6 Subclinical alterations can occur in apparently asymptomatic HTLV-1-infected populations. 9 This finding was confirmed by the present study.
VEMP has previously been shown to be more altered in patients with HAM/TSP when compared to the HTLV-1-asymptomatic carriers, although the correlation with dizziness had not been set. 8,9 The delay in the vestibulospinal reflex may be the explanation for this finding. The integrity of corticospinal tract in individuals with HAM/TSP was scrutinized using the motor-evoked potentials elicited by transcranial magnetic stimulation and the results were consistent with a delay in the motor responses. 29 VEMP is an objective test and the association of altered results with the complaint of dizziness may be an indication of early neurological damage caused by HTLV-1. 6,8,9 The next question to be answered concerns the value of an altered VEMP in an HTLV-1-asymptomatic carrier as a prognostic sign of HAM/TSP development.
About 5% of the individuals infected with HTLV-1 develop HAM/TSP, usually after the fourth decade. Numerous studies have been looking for a immunological or clinical prognosis biomarker. 2,30 The HAM/TSP diagnosis has usually been late and has been made when the person gradually evolves to symmetrical paraparesis of the lower limbs with signs of pyramidal tract involvement. 3 The first symptoms have been related to urinary and sexual problems. 12 Based on the present study, dizziness may precede the described initial symptoms.
Conclusions
Dizziness without an apparent etiology in HTLV-1-asymptomatic carriers deserves attention in terms of a possible subclinical spinal cord involvement and should be clarified through spinal electrophysiological tests. Damage to the vestibulospinal tract seems to occur in the early stages of HAM/TSP.
Footnotes
Acknowledgments
This work was supported by the CNPQ, FAPEMIG, Fundação Hemominas, Faculdade de Medicina–Programa de Pós Graduação em Infectologia e Medicina Tropical da FM/UFMG, CAPES. The authors would also like to thank the remaining participants of the GIPH cohort study for their support.
Author Disclosure Statement
No competing financial interests exist.