
Abstract
In a cohort of HIV-infected patients of sub-Saharan origin we describe the incidence of metabolic syndrome, insulin resistance, and lipodystrophy after 3 years of combined antiretroviral therapy, and model the 10-year risk of cardiovascular diseases, while taking into account environmental factors. This is a multinational, prospective cohort study conducted in HIV outpatient clinics from four tertiary care centers set in France and Côte d'Ivoire. The participants were HIV-infected, treatment-naive patients eligible to start antiretroviral treatment and were of sub-Saharan African origin. The main outcome measures were the incidence of metabolic syndrome, insulin resistance, and lipodystrophy, and the assessment of the 10-year risk of cardiovascular diseases using Framingham risk prediction, D.A.D. Cardiovascular Disease Risk, and WHO/ISH prediction charts. Of 245 patients followed for up to 3 years, the incidence of metabolic syndrome, insulin resistance, and lipodystrophy was 5.5, 8.5, and 6.8 per 100 person-years of follow-up (cumulative incidence: 14.4%, 19.2%, and 18.1%, respectively). Living in France as well as female gender and being overweight were risk factors for metabolic disorders as whole and only first generation protease inhibitors were marginally associated with metabolic syndrome. Cardiovascular risk as modeled through the three equations was high in all patients with the synergistic and deleterious effect of living in France compared to Côte d'Ivoire. This cohort study shows how the synergy between HIV, antiretroviral (ARV) exposure, and westernization of life style in a cohort of HIV-infected patients of sub-Saharan origin leads to a progressive increase in the risk of lipodystrophy, as well as metabolic syndrome and insulin resistance, all associated with increased cardiovascular risk.
Introduction
C
The fight against the HIV epidemic has involved the wide distribution of ARV agents now known to be implicated in the development of metabolic disorders 10,11 and this has lead to the suggestion that part of the increase in overall cardiovascular risk may be attributable to HIV and its treatment. 12 Many observers point equally to the entanglement of the HIV epidemic with the continuous urbanization and “westernization” of lifestyles as another accelerator of the CVD epidemic in sub-Saharan Africa. 1,13 To date, no data from cohorts of HIV-infected patients can confirm this hypothesis.
Two major components of metabolic disorders are the metabolic syndrome (MS), as defined by the International Diabetes Foundation (IDF) in 2005, 14 and insulin resistance (IR), considered a prediabetes condition. Conflicting data have been published in sub-Saharan Africa regarding the causality of HIV and ARV in the occurrence of both conditions. In a Nigerian cross-sectional study on 291 HIV-infected patients, the prevalence of an IDF-defined MS was estimated at 17.1%, with no link to ARVs. 15 However, in Benin, the incidence of MS in a cohort of 88 newly treated patients was 13% after a mean ARV duration of 15 months. 16
Regarding insulin resistance, a case-control study conducted in Senegal comparing 181 HIV-infected patients on long-term ARV to 180 gender-matched controls showed a significantly higher prevalence in the case group. 17 Data from well-conducted prospective cohort studies are sparse and none answers the question of the incidence of long-term metabolic disorders coupled with the impact of the sub-Saharan African environment. We have designed a prospective cohort study including ARV-naive HIV-infected patients of sub-Saharan origin living either in Côte d'Ivoire or in France. The goal of the cohort was to describe the 3-year incidence of MS, insulin resistance, and lipodystrophy after initiation of combined antiretroviral therapy (cART), while taking into account environmental factors. We also modeled the 10-year risk of CVDs in this population.
Materials and Methods
Study setting, population, and recruitment
The study took place within the Department of Infectious Diseases of three university hospital centers in Paris, France and at the Treichville University Hospital Center in Abidjan, Côte d'Ivoire, with a subsequent prospective follow-up of 3 years. To be included, the patients had to be HIV infected, 16 years or older, and of sub-Saharan African origin. They were also ARV naive but eligible to start cART according to the local guidelines at the time of the study design (i.e., World Health Organization ARV Guidelines for Côte d'Ivoire; French National Guidelines 18 ). Exclusion criteria were end-stage renal, liver, or cardiac disease, concurrent pregnancy, a Karnofsky index of less than 70%, clinical signs of lipodystrophy, a body mass index (BMI, kg/m2) greater than 30 or less than 16, the presence of an MS according to the IDF 23005 definition, diabetes (fasting glucose ≥6.1 mmol/liter), triglycerides >2.2 mmol/liter, and total cholesterol >5.5 mmol/liter. Patients with a current prescription for oral corticosteroids, lipid- or glucose-lowering agents, antihypertensive agents, immunomodulators, and/or antineoplastic agents were also excluded.
This study conformed to ethical standards as set out in the Declaration of Helsinki. It received approval from both Ivorian and French national ethics committees. All patients gave written informed consent for participating in the study. Illiterate patients were required to have an independent witness with them during the information session. After receiving the patient's oral approval of their study participation, the witness was required to sign and date the informed consent form alongside with the research physician.
Clinical and laboratory examinations
Patients were assessed by the same medical team during the whole study period. Demographic data, smoking status, and personal and family medical histories were collected at inclusion. A complete physical examination, including blood pressure, weight, height, and anthropometric measurements (waist, hip, mid-thigh circumferences, bicipital and tricipital skin folds), was performed at inclusion and every 3 months. 19 A history of ARV prescriptions including discontinuation and switch was recorded prospectively, using both drug international common denomination and drug classes: protease inhibitor (PI), nonnucleoside reverse transcriptase inhibitor (NNRTI), and nucleos(t)ide reverse transcriptase inhibitor (NRTI). Signs of regional body fat changes defined as lipodystrophy were noted and characterized as lipoatrophy, lipohypertrophy, or mixed lipodystrophy, according to the definition used by Carr et al. 20 The severity of lipodystrophy was defined by four grades: Absent (score of 0), Mild, noticeable on close inspection (score of 1), Moderate, readily noticeable by the patient or physician (score of 2), and Severe, readily noticeable to a casual observer (score of 3). Only grades moderate or severe were considered cases of lipodystrophy.
Laboratory examinations were performed at baseline and every 6 months and included CD4 cell count, HIV-1 RNA, a fasting glucose and lipid panels, liver enzymes, serum creatinine, and complete blood counts. The results of the latter, coupled with anthropometric and blood pressure measurements every 6 months, were used to determine the presence of the 2005 IDF MS. This was defined by the presence of a waist circumference >102 cm in males or >88 cm in females and two to four of the following criteria: a systolic blood pressure ≥130 mmHg or diastolic blood pressure ≥85 mmHg, fasting triglycerides >1.7 mmol/liter, HDL cholesterol <1.03 mmol/liter in males or <1.29 mmol/liter in females, or a fasting blood glucose ≥5.6 mmol/liter. 14
Protein electrophoresis, amylase, lactate, and fasting insulin levels were performed annually. Based on glucose and insulin levels, insulin resistance was assessed every year using the homeostatic model assessment (HOMA) equation [(fasting serum insulin×fasting serum glucose)/22.5]. 21 An HOMA score above 2.0 was considered as reflecting the presence of insulin resistance. 22 Other evaluations done during the study period included a quarterly adherence questionnaire and a nutritional survey performed at inclusion and every year. High fat-containing (≥35% of daily kilocalories intake), protein-containing (≥20% of daily kilocalories intake), and sugar-containing (≥55% of daily kilocalories intake) diets were characterized according to definitions used in the FRAM study. 19
Statistical analysis
The sample size calculation was based on the probability of showing a 20% prevalence of lipodystrophy in the study population. This was based on a precohort cross-sectional study in one of the recruiting centers in Paris, where 23% of HIV-infected patients originating from sub-Saharan Africa and starting cART were found to be lipodystrophic after a median treatment duration of 5 years. 23 Therefore, the inclusion of 200 patients would have led to at least 40 cases of lipodystrophy (α risk of 0.05 and 1-β power of 80%). Statistical analysis was performed using Stata Statistical Software for Professionals (Stata 10.0; Stata Corporation, College Station, TX).
Incidence rates of lipodystrophy and metabolic disorders were calculated as number of events per 100 person-years of follow-up using Kaplan–Meier estimates. The follow-up period started 6 months after the inclusion date and ended at the date of censoring or event (moderate to severe lipodystrophy, MS, or HOMA >2). The censoring date was the 36-month study visit. Other censoring events included death, pregnancy, and loss of follow-up.
Cox proportional hazards regression models were used to identify demographic, clinical, therapeutic, and metabolic factors associated with MS, insulin resistance, and progression to moderate and severe lipodystrophy. Univariate and multivariate analyses were performed both stratified and nonstratified by patients' country of residence.
Ultimately, the prediction of 10-year cardiovascular risk (CVR) based on the characteristics of the study population was performed using three equations: the Framingham risk prediction
24
(available at
Results
Clinical and laboratory characteristics of the study population
The prospective cohort included 245 patients, 176 in Abidjan and 69 in Paris (Fig. 1 and Table 1). After a median follow-up of 37.9 months, 162 patients completed the last study visit (114 in Abidjan and 48 in Paris) for a total of 7,434.4 person-months of follow-up. Study participants living in France had emigrated from sub-Saharan Africa a median of 41 months earlier. HIV disease was more advanced in patients living in Côte d'Ivoire versus patients living in France (CD4 119/mm3 vs. CD4 199/mm3, p=0.001) with higher viral loads for patients in Côte d'Ivoire versus France (HIV-RNA: 5.32 log10 copies/ml vs. 4.62 log10 copies/ml, p=0.001).
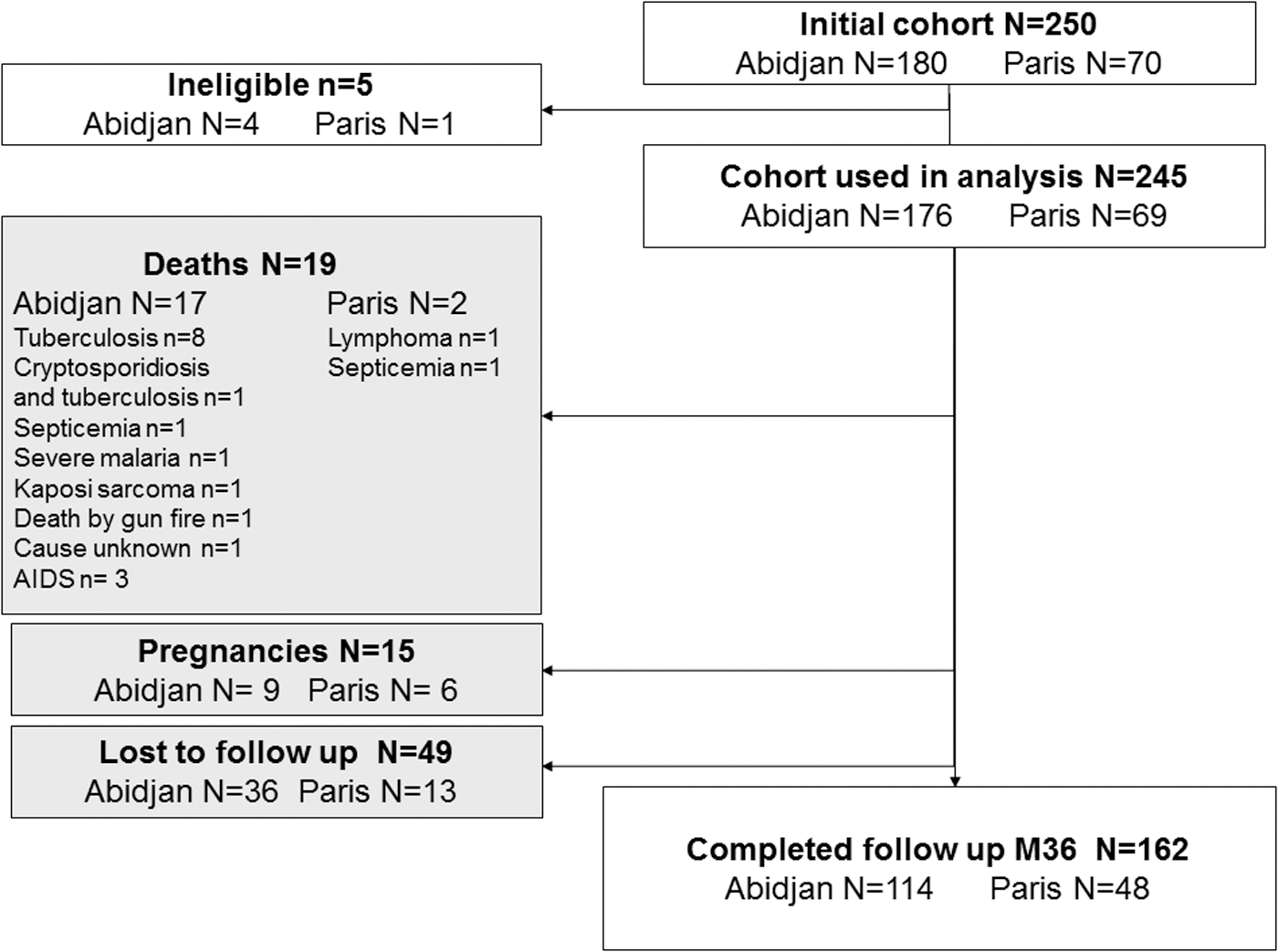
Patients flow chart.
Three (4.4%) cases of HIV-2 monoinfection in Paris.
IQR, interquartile range; HIV, human immunodeficiency virus; CDC, Centers for Disease Control and Prevention; BMI, body mass index; WHR, waist-to-hip ratio; LDL-c, low-density lipoprotein cholesterol, HDL-c, high-density lipoprotein cholesterol; HOMA-IR, homeostatic model assessment-insulin resistance; HIV, human immunodeficiency virus.
The initial clinical, laboratory, and diet evaluation revealed that patients living in France were more likely to be current smokers and alcohol drinkers, had a higher total caloric intake (although excessive dietary consumption of fat, protein, and sugar did not differ between sites), and had a higher baseline BMI, blood pressure, baseline triglycerides, fasting glucose, and HOMA than patients from Côte d'Ivoire (Table 1).
Combined antiretroviral therapy (cART) during follow-up
The cART regimen prescribed in France was PI based in 71% of patients, with either ritonavir-boosted atazanavir (ATZ/r) or lopinavir (LPV/r) given in combination with a tenofovir (TDF)/emtricitabine (FTC) or abacavir (ABC)/lamivudine (3TC) backbone (Supplementary Table S1; Supplementary Data are available online at
One-third (33.5%) of the 245 patients in the cohort reported ARV-associated adverse events. More than half (54.9%) of patients with a reported adverse event experienced a Grade 1 or 2 event, while 44% experienced a Grade 3 event, most commonly rash, diarrhea, peripheral neuropathy, and insomnia. There was only one reported Grade 4 event in a patient from Abidjan who developed life-threatening AZT-associated anemia. There was no significant difference in the frequency of Grade 1 or 2 reported side effects between the two sites (p<0.2), but Grade 3 side effects were reported more in Abidjan than in Paris, at a frequency of 17.0% versus 7.3% (p<0.001).
Incidence and determinants of lipodystrophy
In total, 39 patients developed a moderate to severe case of lipodystrophy (cumulative incidence: 18.1%), with an overall incidence rate of 6.8 per 100 person-years of follow-up for patients having more than two study visits (n=215). The incidence rate in France over the 3-year period was 14.2 per 100 person-years of follow-up, more than three times the rate in Côte d'Ivoire (4.4 per 100 person-years of follow-up, p<0.001) (Fig. 2a). The incidence of lipohypertrophy was higher in France (11.8 compared to 1.4 per 100 person-years of follow-up in Abidjan, p<0.001), whereas there was no difference between incident cases of mixed lipodystrophy (1.2 per 100 person-years of follow-up in Paris versus 2.5 in Abidjan, p=0.4) and lipoatrophy (0.6 per 100 person-years of follow-up in Paris versus 0.5 in Abidjan, p=0.7). Lipodystrophic patients tended to have a higher BMI (47.2% had a BMI above 25, compared to 8.7% in nonlipodystrophic patients, p<0.001) and a higher HOMA score at baseline (33.3% had an HOMA index >2, compared to 12.9% in nonlipodystrophic patients, p<0.001).
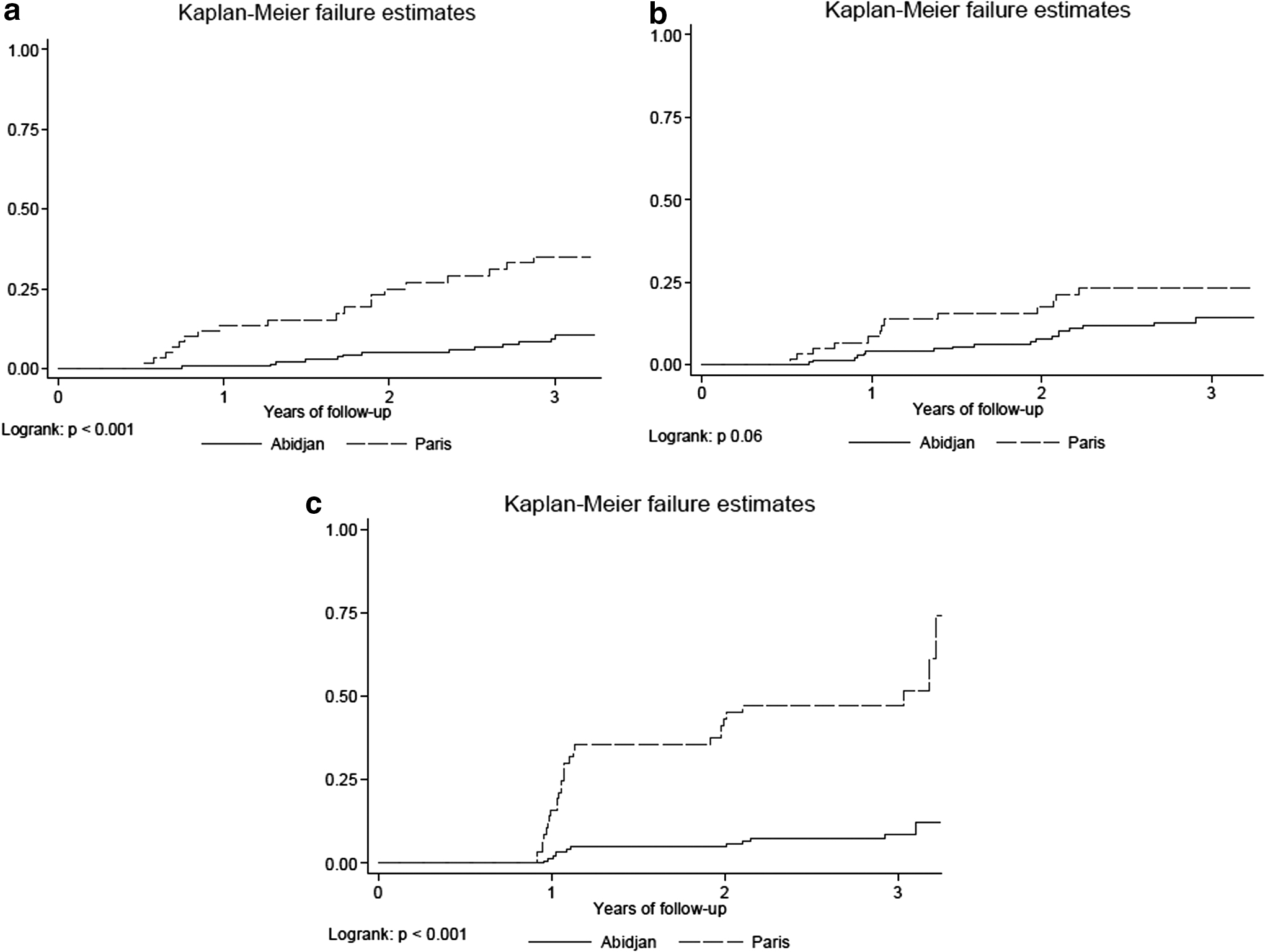
Survival curves of patients with metabolic disorders.
In multivariate analysis, risk factors for lipodystrophy in the whole population were a baseline BMI ≥25 kg/m2 (OR: 4.45, CI 95% 1.88–10.52), while residence in Côte d'Ivoire was a protective, yet marginally significant factor (OR: 0.4, CI 95% 0.15–1.03). Stratification on country of residence showed in univariate analysis that a BMI ≥25 kg/m2 was a risk factor for lipodystrophy in both countries, whereas an HOMA score >2 and triglycerides >1.7 mmol/liter were highly predictive factors only for patients living in France (Supplementary Table S2). An exposure to LPV/r and saquinavir (SQV) of more than 18 months was also associated with a higher risk of lipodystrophy in Côte d'Ivoire. However, after adjustment, only BMI remained associated (yet marginally for Abidjan) with the occurrence of lipodystrophy in both cohorts.
Incidence and determinants of the metabolic syndrome
Overall, 31 patients developed the MS (cumulative incidence: 14.4%), with an incidence rate of 5.5 cases per 100 person-years of follow-up and no significant difference between countries (8.8 per 100 person-years of follow-up in France versus 4.3 in Côte d'Ivoire, p=0.06) (Fig. 2b). Almost all cases were females with 45% of cases having a baseline BMI of 25 kg/m2 or more.
In the total cohort, female gender (OR: 6.4, CI 95% 1.9–21.8) and BMI ≥25 kg/m2 (OR: 3.7, CI 95% 1.7–8.3) were highly significant predictors for the development of the MS in the multivariable model. Multivariate analyses stratified on countries of residence revealed that baseline BMI ≥25 kg/m2 and female gender were both significant predictors of the development of the MS in patients from Côte d'Ivoire, but an overweight baseline BMI showed a trend toward significance only in patients from France (Supplementary Table S3). In addition, for those patients taking SQV for 18 months or more, it was the only ARV significantly predictive of the MS in France, whereas in Côte d'Ivoire, there was a trend toward significance for taking nelfinavir for 18 months or more.
Incidence and determinants of insulin resistance
Insulin resistance developed in 47 patients, 17 in Côte d'Ivoire and 30 in France (cumulative incidence: 21.9%), with an overall incidence of 8.48 cases per 100 person-years (24.2 in France versus 3.95 cases per 100 person-years in Côte d'Ivoire, p=0.0001) (Fig. 2c). Patients with acquired insulin resistance were significantly older (37.4 vs. 35.2 years, p=0.03), more overweight before treatment initiation (31.9% had a BMI >25, compared to 10.9% in patients without IR, p<0.001), had a better immune status at baseline (38.3% had a total CD4 count vs. 22.7% in patients without IR, p=0.03), and had a longer exposure to PIs, especially second- and third-generation PIs such as LPV/r, ATZ/r, ritonavir-boosted fosamprenavir (FPV/r), and ritonavir-boosted darunavir (DRV/r) (42.4 months of exposure vs. 35.4 months in patients without IR, p≤0.001).
Multivariate analysis for risk factors of insulin resistance in the entire cohort showed that a BMI ≥25 kg/m2 (OR: 2.3, CI 95% 1.09–2.7) was a strong risk factor of an HOMA ≥2, whereas living in Côte d'Ivoire (OR: 0.12, CI 95% 0.05–0.3), an exposure to nevirapine (NVP) and efavirenz (EFV) of more than 12 months (OR: 0.22, CI 95% 0.06–0.9 and OR: 0.22, CI 95% 0.08–0.6, respectively), and an exposure to second- and third-generation PIs (LPV/r, ATZ/r, FPV/r, DRV/r) of more than 24 months (OR: 0.23, CI 95% 0.09–0.6) were protective factors against IR. Analysis stratified by country revealed that an SQV exposure of ≥18 months was a significant risk factor for insulin resistance in Côte d'Ivoire, but showed only a trend in patients living in France (Supplementary Table S4).
Prediction of cardiovascular risk
The estimation of 10-year cardiovascular risk based on the study population and stratified by country of origin was very low when using the Framingham equation, almost constant around 3% during follow-up, and did not differ by country (Fig. 3a). When using the D.A.D. equation (Fig. 3b), a significantly higher risk was calculated at baseline and throughout follow-up for patients living in France (2.43% vs. 1.37% at baseline for patients from Côte d'Ivoire, p<0.001), but a steady increase was observed in patients from Côte d'Ivoire (1.37% vs. 2.45% at 36 months, p<0.001); at the end of follow-up, the risk was equal in both countries (2.93% in France vs. 2.45% in Côte d'Ivoire, p=0.3). Survival analysis based on the results from the D.A.D. score showed that around 50% of the whole study population had a 50% increase in CVR after 3 years of follow-up (Supplementary Fig. S1). When using the WHO/ISH CVR prediction charts, estimated CVR remained in the <10% category for all participants in France and Côte d'Ivoire until 2 years, when there was a notable increase in the 10–19% and 20–29% risk in the Abidjan site (Fig. 3c).
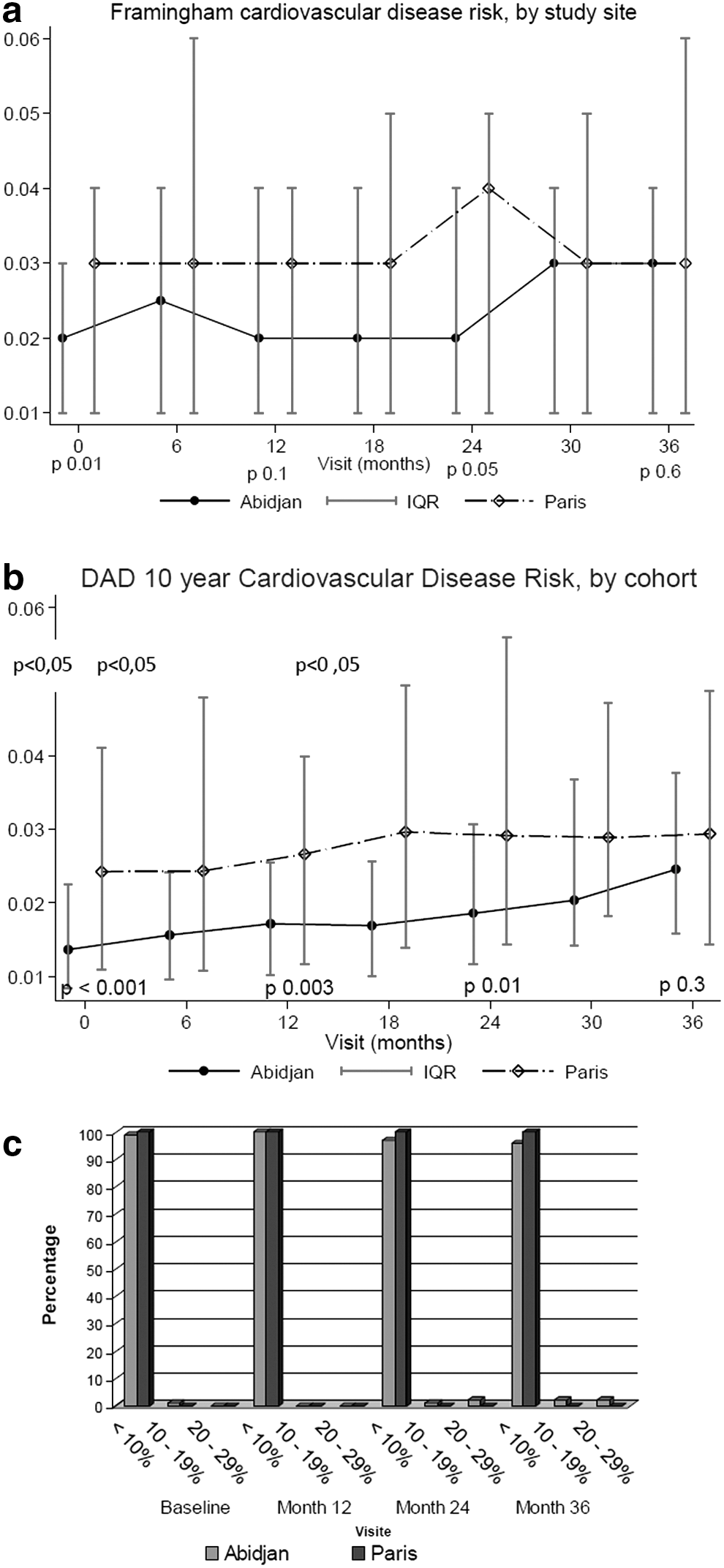
Ten years cardiovascular risk prediction in the study population.
Discussion
This prospective international cohort study provided cardiovascular risk estimations and documented the incidence and risk factors of ARV-associated lipodystrophy and other metabolic disorders in HIV-infected patients of sub-Saharan African origin and initiating ARV. The stratification on the country of residence at time of ARV treatment made it possible to specifically study the impact of the environment on the onset of metabolic ARV-associated side effects.
While the global incidence of lipodystrophy is in the range of what has been observed in other African settings (Benin: 1.72 per 100 person-months of cART 16 ; Malawi: 11.4 per 100 person-months of cART 28 ), it greatly differed between both groups of patients, with a 3-fold increase in HIV-infected patients residing in France compared to that of patients residing in Côte d'Ivoire. The lower global incidence rate may be partly explained by the fact that in other settings such as Malawi and Benin, patients were mostly given a first-line stavudine-containing regimen, known to induce high rates of metabolic toxicity, 29,30 while patients from France did not receive stavudine and patients living in Côte d'Ivoire were switched to a stavudine-free regimen very early during the course of ARV therapy. In both study cohorts, metabolic characteristics such as the level of BMI and HOMA before treatment were determinants of subsequent lipodystrophy.
The finding of an elevated BMI as a predictor of hypertrophic or mixed type lipodystrophy echoes that seen in the Benin cohort. 16 Overweight and obesity are becoming common features of urbanization in sub-Saharan Africa, 2,31 and precede ARV initiation in most HIV settings. 32 In our cohort, patients living in Paris, France, had a higher BMI at inclusion and higher subsequent rates of lipodystrophy than those living in Abidjan, suggesting that the impact of environment is indeed important relative to the risk of being overweight. As the African patients in the Paris cohort had a median residency in France of almost 3.5 years, it might be postulated that these patients had developed a more European way of life in terms of how they ate and exercised. This is also reflected in the higher calorie intake in the patients living in Paris.
The fact that an HOMA >2 before treatment initiation (associated with insulin resistance, known to be a component of LPD 17 ) is also a prognosis factor of LPD after treatment initiation further suggests that the onset of LPD is conditioned in Africa by metabolic factors that affect the population as a whole, and not only HIV-infected patients. 2 Of note, no ARV was seen as a predictor of lipodystrophy. The fact that the analysis might have a lack of power to see an effect of treatment on LPD due to the rather small number of patients goes along with other recent cohort studies that have not found a relationship between ARVs and LPD. 16,33
In addition to LPD, we also estimated the incidence of insulin resistance, which has not previously been reported in HIV-infected patients living in Africa after treatment initiation. The cumulative incidence after 3 years of ARV exposure is close to what has been observed in cross-sectional cohorts. Of note, the incidence of insulin resistance is higher in patients living in Paris compared to those living in Abidjan by 6-fold and is very close to what has been reported in a cohort of white HIV-infected patients living in Spain. 34 Determinants of insulin resistance were mostly related to ARV regimen, particularly with saquinavir in the Abidjan setting. This is in line with published scientific data showing that saquinavir impairs glucose-stimulated insulin secretion from INS-1 beta cells after a 48-h incubation period with noncytotoxic concentrations. 35 Newer second- and third-generation PIs were found to be protective, opposed to first-generation PIs, which are known to be toxic for cell metabolism. 36
The MS is closely related to insulin resistance and prospective data regarding its incidence in cohorts of treated HIV-infected patients living in sub-Saharan Africa are very scarce. In the Benin cohort, 16 it has been estimated to average 6.2 per 100 person-years of follow-up, similar to the rate observed in our cohort. Of note, there was no difference in the MS rate between Paris and Abidjan. Overweight and female gender were also associated with MS in cohorts from Benin 16 and Nigeria, 15 as they were in our cohort. The impact of ARV treatment seemed to be marginal, with a slight reported effect of the exposure to saquinavir or nelfinavir. This is in line with the now commonly accepted fact that MS is secondary to the use of first-generation PIs. 37
Finally, the estimation of cardiovascular risk by different risk equations further points out how much HIV-infected patients from sub-Saharan origin are exposed to an increasing risk of developing cardiovascular disease after ARV introduction, with a synergistic effect of environment, as suggested by the higher rate observed in patients living in Paris compared to those in Abidjan. This increasing risk slope parallels that of the LPD, MS, and IR, reflecting and strengthening the known association between the onset of metabolic disorders and cardiovascular morbidity. 38,39
Our study involves some limitations that need to be acknowledged. First, there has been a shift in treatment guidelines during the course of the study, and most of the patients treated with stavudine have been switched to less toxic NRTIs. 27 This explains the absence of association found between the risk of LPD and use of stavudine, as evidenced in many other studies. 28,29 However, this finding indirectly strengthens the fact that a lower exposure to stavudine leads to a decreased risk of LPD. 40 Second, a 3-year follow-up is too short to demonstrate cardiovascular events in a 245 patient-cohort, leading us to use prediction models in order to evaluate cardiovascular risk in this population. As for all data acquired through modeling strategies, results should be validated later in larger cohorts with a longer follow-up. However, data regarding the prediction of cardiovascular risk in a population of sub-Saharan HIV-infected patients are to our knowledge lacking so far and this study provides the first evidence of the magnitude of the awaited and feared epidemics of cardiovascular disease in the HIV population, as part of the large spectrum of noncommunicable diseases that will be affecting Africa in the coming decades. 41
In conclusion, this cohort study has shown how the synergy between HIV, ARV exposure, and westernization of life style in a cohort of HIV-infected patients from sub-Saharan origin has led to a progressive increase in the risk of lipodystrophy as well as metabolic syndrome and insulin resistance, all associated with cardiovascular risk, as depicted in the literature from non-HIV-infected patients.
Footnotes
Author Disclosure Statement
This study has been partly funded by a grant from the Bristol Myers Squibb “Secure the Future” program.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.