
Abstract
The objectives were to (1) compare the frequency of contraindicated drug–drug interactions (XDDI) when simeprevir (SIM)- and sofosbuvir (SOF)-containing regimens are theoretically added to a patient's medication profile; (2) identify which hepatitis C (HCV) regimen is associated with the lowest frequency of XDDIs within different types of antiretroviral treatment (ART) regimens; and (3) determine the risk factors for XDDIs with each regimen. A cross-sectional study was performed among adult HIV/HCV-coinfected patients. Demographics, comorbidities, and medication lists were collected from medical records. Medication lists were entered into Lexi-Interact drug interaction software and XDDI before/after the addition of SIM- and SOF-containing therapy was documented. Classification and regression tree (CART) analyses identified breakpoints in continuous variables. Before the addition of any HCV therapy, XDDIs were present in 20% of the 335 included patients. After the addition of SIM-containing therapy, the frequency of XDDIs significantly increased to 88.4% (p<0.001). After adding SOF-containing therapy, the prevalence of XDDIs increased to 24.5% (p<0.001). The prevalence of XDDIs was significantly lower for SOF-containing HCV therapy within various types of ART regimens. Use of ≥7 non-HIV medications (CART breakpoint) was the only variable to predict XDDIs before the addition of any HCV therapy. Similarly, this was the only variable to predict XDDIs after the addition of SOF-containing therapy (PR: 4.80; 95% CI: 2.57–8.96, p<0.001). Variables independently associated with XDDIs after the addition of SIM-containing therapy were NNRTI regimen (prevalence ratio, PR: 1.62; 95% confidence interval, CI: 1.38–1.91, p<0.001), PI regimen (PR: 1.64; 95% CI: 1.40–1.93, p<0.001), and ≥7 non-HIV medications (PR: 1.06; 95% CI: 1.00–1.14, p=0.09). The addition of SOF-containing therapy was associated with a lower prevalence of XDDI than SIM-containing therapy.
Introduction
I
While the efficacy and tolerability of SIM- and SOF-containing treatment regimens are reasonably comparable, one differentiating factor of these two regimens is drug–drug interactions. This issue is particularly important for patients with human immunodeficiency virus (HIV) and HCV coinfection. Treatment of HIV infection requires the use of at least three fully active antiretroviral (ART) agents to maintain HIV virologic suppression and maximize HIV-related outcomes. 10 Many ART medications, such as the protease inhibitors and nonnucleoside reverse transcriptase inhibitors (NNRTIs), have been implicated in several drug–drug interactions because their metabolic pathways involve either CYP450 isoenzymes or p-glycoprotein. 11,12 Drug–drug interactions can have serious sequelae such as increased toxicity or loss of HIV or HCV virologic suppression. 13,14 To complicate matters further, the increasingly aged population of patients with HIV/HCV coinfection tend to have other comorbidities requiring medication therapy management, raising the likelihood of additional drug–drug interactions. 15
While pharmacokinetic drug interaction studies are performed between individual agents, it is unclear from a population-based perspective whether SIM- or SOF-containing therapy is associated with a lower frequency of drug–drug interactions. There are few data to suggest whether one or the other is preferable to coadminister with different types of ART. While it would seem plausible that SIM would be associated with more drug–drug interactions because it is metabolized by the cytochrome P450 isoenzyme system and SOF is not, the population-based risk of either agent has not been described in the literature. 1,2 Finally, no studies have quantified the risk factors for experiencing drug–drug interactions with each type of HCV regimen. This study is designed to inform these questions by (1) comparing the frequency of contraindicated drug–drug interactions (XDDIs) in the absence or presence of DAA therapy in an HIV/HCV-coinfected population, (2) determining risk factors for XDDIs associated with each DAA regimen, and (3) identifying which HCV treatment is least likely to be associated with significant interactions involving ART.
Materials and Methods
Study design and population
This cross-sectional study included patients who were coinfected with HCV and HIV and received care between 1/1/2000 and 7/31/2012 at the Upstate New York Veterans' Healthcare Administration (VISN-2) or Upstate University Hospital (Syracuse, NY). Patients meeting the following criteria were enrolled: (1) age ≥18 years, (2) documented HIV infection, and (3) laboratory-confirmed diagnosis of HCV infection (all genotypes). Those without a documented medication history were excluded from the study.
Data collection
The following was collected from patients' medical records: demographics, comorbidities, social history, and medication lists. Demographic variables were age, sex, race, weight, and years of HCV and HIV diagnoses. A list of all comorbidities from the medical record was documented. Acute or opportunistic conditions (e.g., oropharyngeal candidiasis, pneumonia) were not considered comorbid conditions. The most recent CD4 cell count, HIV-RNA, and HCV-RNA were included for laboratory values. For each medication in the most recent outpatient list (including nonprescription medications), the drug name, dose, strength, and frequency were documented. The drug class was used to categorize each medication in the medication list. The number of total and non-HIV medications was computed. Polypharmacy was defined as the use of multiple medications.
Antiretroviral therapy was classified by type of regimen, which was composed of two nucleoside reverse transcriptase inhibitors (NRTIs) plus one of the following: (1) nonnucleoside reverse transcriptase inhibitor (NNRTI), (2) protease inhibitor (PI), or (3) integrase strand transfer inhibitor (INSTI). Any combination ART not classified as one of the above was considered a mixed/multiple class ART regimen. Treatment-naive/experience status was also captured.
Outcome assessment
The outcome of interest in this study was the prevalence of XDDIs between the medications in the patient's profile and the theoretical addition of either SIM- or SOF-containing HCV therapy. The four guideline-recommended regimens that were assessed were (1) simeprevir, pegylated interferon (PegIFN), and ribavirin (SIM+PR), (2) sofosbuvir, PegIFN, and ribavirin (SOF+PR), (3) simeprevir, sofosbuvir and ribavirin (SIM+SOF+R), and (4) sofosbuvir and ribavirin (SOF+R).
Prior to the addition of SIM- or SOF-containing therapy to a patient's medication profile, XDDIs were identified. After SIM- or SOF-containing therapy was added, additional XDDIs involving HCV therapy were identified. This was accomplished with Lexi-Interact drug interaction software, 16,17 which records the number and nature of the XDDIs. For the purposes of these analyses, XDDIs were those that Lexi-Interact reported as X-rated (contraindicated interactions). 16,17 After capturing XDDIs that existed within the patients' medication lists, the HCV treatment regimen of SIM+PR was added to the existing medication profile in Lexi-Interact and the number and nature of XDDIs were recorded. This process was repeated for SOF+PR, SIM+SOF+R, and SOF+R regimens.
Because interaction studies were on-going during the study period and to mimic what would occur in clinical practice, the output from Lexi-Interact was cross-matched with the current prescribing information for simeprevir (Olysio) and sofosbuvir (Sovaldi). 1,2 Any new drug–drug interaction data that became available during the study period were included in the analysis.
Statistical analyses
Bivariate analyses assessed covariates and XDDIs after the addition of a SIM- or SOF-containing HCV regimen. Categorical variables were evaluated using the χ2 or Fisher's exact test; continuous variables were compared using the Student's t or Mann–Whitney U test. Due to the inherently matched sample (before/after addition to HCV therapy), McNemar's test was used to assess the frequency in XDDIs before and after the addition of different types of SIM- and SOF-containing HCV regimens. The Wilcoxon signed rank test was used to compare the frequency of XDDIs between the different types of HCV regimens. Classification and regression tree (CART) analysis was used to identify breakpoints in continuous variables where the probability of XDDI differs.
Variables associated with an XDDI in the bivariate analyses (p<0.25) were considered for inclusion in the multivariate regression analyses. Effect modification was evaluated by including interaction terms in the multivariate model. We selected log-binomial regression with robust variance estimates because a high proportion of patients (>10%) were expected to have the outcome. 18 The most parsimonious model was derived using a backward stepwise procedure. Variables with a p-value less than 0.05 remained in the final model. After the final set of covariates was identified, all potential confounders were reentered and retained only if the resulting prevalence ratios were adjusted by more than 10%. All calculations were computed using SPSS version 11.5 (SPSS Inc., Chicago, IL), SAS version 9.3 (SAS Institute, Cary, NC), and CART software (Salford Systems, San Diego, CA).
Sample size justification
A minimum of 234 patients was needed to detect an effect size of 20% for XDDIs under the assumption that the type I error frequency was 5% and 80% power.
Results
Of the 335 patients who met the inclusion criteria, 244 (72.8%) were from VISN-2 and 91 (27.2%) patients were from Upstate University Hospital. Most patients (87.2%) were male and the mean (standard deviation, SD) age was 55.6 (7.3) years. Median (IQR) durations of HIV and HCV infections were 18 (13–23) and 13 (10–17) years, respectively. The median (interquartile range, IQR) number of comorbidities was 8 (6–12). The most common comorbidities were a history of substance abuse (61.2%), depression (40.3%), and hypertension (36.4%). Polypharmacy was expected in this population; patients were prescribed a mean (SD) of 11.2 (4.9) medications. Among the 306 (91.3%) patients receiving combination ART, the most frequent regimen types were NNRTIs (39.9%), PIs (38.6%), mixed/multiple class ART regimen (17.0%), and INSTIs (4.6%). Among the non-HIV medications being utilized, central nervous system (CNS) depressants (47.8%) and antidepressants (30.7%) were the most commonly utilized drug classes.
The prevalence of XDDIs before/after the theoretical addition of HCV therapy is displayed in Fig. 1a. Before the addition of HCV therapy, the prevalence of XDDIs was 20%. After the addition of both types of SIM-containing therapies, the frequency of XDDIs significantly increased to 88.4% for both regimens (p<0.001). After adding both types of SOF-containing HCV treatments, the prevalence of XDDIs increased to 24.5% for both regimens (p<0.001).
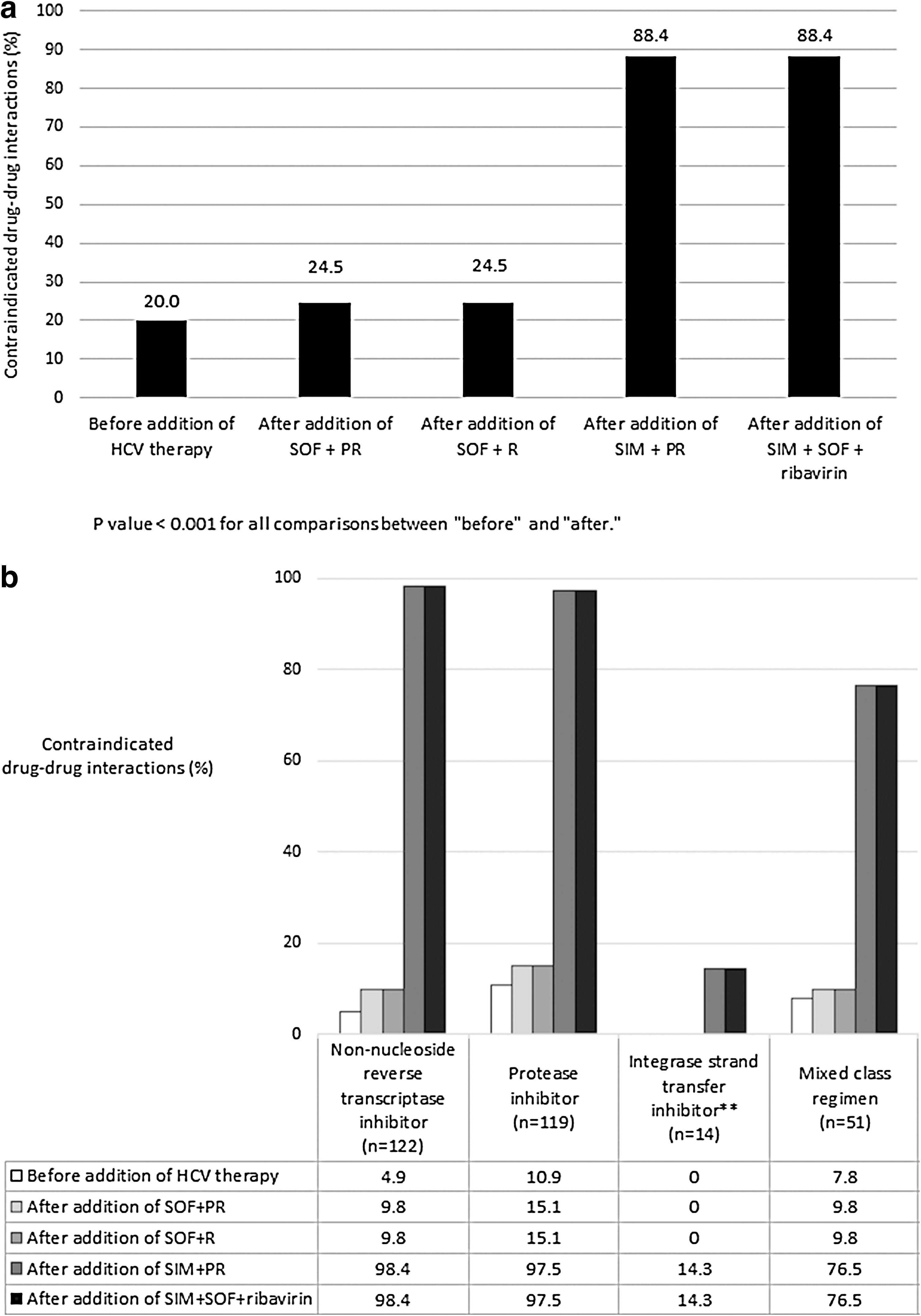
The prevalence of XDDIs, stratified by regimen type, is displayed in Fig. 1b. Before the addition of HCV therapy, the overall frequencies of XDDIs involving ART between the different regimen types were NNRTI (4.9%), PI (10.9%), INSTI (0%), and mixed/multiple class ART (7.8%). With the exception of INSTI-based ART regimens, the prevalence of XDDIs after addition of HCV therapy was significantly lower for both types of SOF-containing HCV therapies compared to both SIM-containing therapies for all types of ART regimens. For NNRTI-based (97.5%) and PI-based (98.4%) ART regimens, the probability of an XDDI approximated nearly 100% after the addition of either SIM-containing HCV therapy.
We consolidated our analyses to focus on SIM+PR and SOF+PR because results for SIM+SOF+R and SOF+R would have identified the same patients. Prior to the addition of HCV therapy, interactions involving (1) two non-ART drugs, (2) an ART medication and non-ART medication, and (3) two ART medications were present in 16.1%, 6.0%, and 1.8% of patients, respectively. After the addition of SIM- and SOF-containing therapy, interactions involving ART medications occurred in 81.5% and 3.9% of patients, respectively. For XDDI between SIM- and SOF-containing therapy with non-ART medications, 14.0% and 2.7% of patients were affected, respectively.
The bivariate analyses assessing clinical covariates and the frequency of XDDI involving either SIM+PR or SOF+PR regimens are displayed in Table 1. The continuous variables for which significant CART-derived breakpoints were identified included duration of HIV infection, total number of medications, number of non-HIV medications, and number of comorbidities. Variables that were significantly associated with an increased frequency of XDDIs after the addition of SIM+PR were median CD4 count, median number of comorbidities, use of ≥7 non-HIV medications, ART treatment experience, receiving ART, ART regimen type, NRTI, lamivudine, emtricitabine, tenofovir, NNRTI, efavirenz, PI, atazanavir, lopinavir, and ritonavir.
CART-derived breakpoint.
CART-derived breakpoint associated with XDDI after the addition of SIM-containing therapy.
CART-derived breakpoint associated with XDDI after the addition of SOF-containing therapy.
All data are presented as n (%), mean±standard deviation or median (interquartile range), unless otherwise indicated.
XDDIs, contraindicated drug–drug interactions; HCV, hepatitic C virus; CART, classification and regression tree.
Variables that were significantly associated with XDDI after addition of SOF+PR were ≥9 comorbidities, chronic obstructive pulmonary disorder, depression, gastroesophageal reflux disease, posttraumatic stress disorder, use of ≥7 non-HIV medications, antipsychotics, antidepressants, calcium channel blockers, central nervous system depressants, and didanosine.
Predictors of contraindicated drug–drug interactions
Use of ≥7 non-HIV medications (prevalence ratio, PR: 6.78, 95% confidence interval, CI: 3.02–15.23, p<0.001) was the only variable to independently predict XDDI prior to adding HCV therapy. When replaced with the specific drug classes, the predictors were antipsychotics (PR: 3.97, 95% CI: 2.68–5.88, p<0.001), beta-2 agonists (PR: 2.09, 95% CI: 1.26–3.47, p=0.004), calcium channel blockers (PR: 1.69, 95% CI: 1.06–2.70, p=0.03) and corticosteroids (PR: 1.61, 95% CI: 1.05–2.46, p=0.03).
Variables that were independently associated with XDDIs after the addition of SIM+PR were use of an NNRTI regimen (PR: 1.62; 95% CI: 1.38–1.91, p<0.001), PI regimen (PR: 1.64; 95% CI: 1.40–1.93, p<0.001), and ≥7 non-HIV medications (PR: 1.06; 95% CI: 1.00–1.14, p=0.09). To add specificity to the model, medications in the PI and NNRTI classes were added to the model and a backward stepwise process was performed to identify the most parsimonious model with the individual agents. In addition to use of ≥7 non-HIV medications (PR: 1.10, 95% CI: 1.03–1.17, p=0.006), the specific NNRTI and PI agents to predict XDDI after the addition of SIM+PR were efavirenz (PR: 2.01, 95% CI: 1.65–2.45, p<0.001), nevirapine (PR: 1.92, 95% CI: 1.59–2.31, p<0.001), atazanavir (PR: 2.02, 95% CI: 1.65–2.47, p<0.001), darunavir (PR: 1.91, 95% CI: 1.54–2.36, p<0.001), fosamprenavir (PR: 2.08, 95% CI: 1.7 –2.55, p<0.001), lopinavir/ritonavir (PR: 1.92, 95% CI: 1.58–2.34, p<0.001), saquinavir (PR: 1.50, 95% CI: 1.09–2.06, p<0.001), indinavir (PR: 2.12, 95% CI: 1.73–2.59, p<0.001), and nelfinavir (PR: 1.62, 95% CI: 1.33–1.97, p<0.001).
For the multivariate analyses examining the variables independently associated with XDDIs after addition of SOF+PR to the patients' medication profiles, ≥7 non-HIV medications was the only variable to predict an XDDI outcome (PR: 4.80; 95% CI: 2.57–8.96, p<0.001). To further refine the predictors of XDDIs after the addition of SOF+PR, ≥7 non-HIV medications were removed from the model and the individual drug classes were replaced. The only variables to be independently associated with an XDDI after addition of SOF-containing therapy were use of antipsychotics (PR: 2.97, 95% CI: 2.08–4.25, p<0.001), antidepressants (PR: 1.53, 95% CI: 1.05–2.22, p<0.03), calcium channel blockers (PR: 2.03, 95% CI: 1.37–3.01, p<0.001), and corticosteroids (PR: 1.53, 95% CI: 1.02–2.29, p<0.04).
Discussion
This study compares the frequency of XDDIs if various HCV treatment regimens were to be initiated in patients with chronic HIV/HCV coinfection. In so doing, we suggest the types of ART that could potentially be coadministered and identify clinical risk factors for XDDIs upon initiation of different types of HCV therapy. Given the pharmacokinetic properties, it would seem intuitive that the contribution of pegylated interferon to XDDI frequency was likely to be negligible. However, we did not want to make any a priori assumptions that would result in consolidating treatments without ensuring that it was appropriate to do so. In our study, the XDDIs that occurred upon addition of SOF+PR were also present in the same patients after the addition of SOF+R to the patients' medication profiles. Similarly, XDDIs that occurred with SIM+PR were also present in the same patients when SOF+SIM+R was included in their medication profiles. Thus, we consolidated the presentation of our findings to describe the risk of XDDIs among SOF+PR and SIM+PR as they would be identical for SOF+R and SOF+SIM+R, respectively.
A major finding was the much greater probability of an XDDI after adding SIM+PR compared to SOF+PR. A 5- to 10-fold increase in the likelihood of XDDI after the addition of SIM+PR was noted for all types of ART, but SOF+PR was not associated with a significantly increased risk of XDDI for any of the ART regimens. It is important to note that SIM is a substrate for CYP3A in the liver and acts as an inhibitor of CYP3A in the intestines. 1 The effect of these XDDIs after the addition of SIM-containing therapy is likely to lead to altered concentrations of SIM in the presence of other interacting drugs that are either inducers or inhibitors or CYP3A. Alternatively, SOF is metabolized by P-glycoprotein (P-gp) and inducers/inhibitors of P-gp are likely to alter SOF exposure. 2 As expected, the use of multiple medications, polypharmacy, appeared to be an important risk factor for all HCV regimens.
Prior to the addition of DAA therapy to medication profiles, predictors of XDDIs were antipsychotics, beta-2 agonists, calcium channel blockers, and corticosteroids. Predictors of XDDI for SIM+PR were the use of various ART medications and ≥7 non-HIV medications. Predictors of XDDI for SOF+PR were antipsychotics, antidepressants, calcium channel blockers, and corticosteroids and were largely consistent with the predictors of XDDI prior to the addition of any HCV therapy.
Collectively, these findings demonstrate that great vigilance is warranted when initiating SIM+PR among HIV/HCV-coinfected patients who are either on ≥7 non-HIV medications or receiving ART. Given that either of these predictors is present in the majority of patients with HIV/HCV coinfection, pharmacotherapeutic intervention is highly likely. One of these interventions may be to switch a patient's ART regimen. This may be associated with other challenges and the focus should be on empowering the patient to achieve optimal drug adherence and maintaining virologic suppression. For SOF+PR, the use of ART did not appear to predict XDDIs. However, pharmacovigilance is still necessary, particularly for patients using ≥7 non-HIV medications.
While this study compares the frequency of XDDI between SIM- and SOF-containing regimens, some limitations may affect the interpretation of these data. First, there are inherent limitations to cross-sectional studies and they primarily are temporal ambiguity and length-bias sampling. The baseline frequency of XDDIs was 20% and seems to be high. Considering this was a cross-sectional study the medication lists represent only a snapshot in time. It is important to note that many XDDIs do not result in immediate consequences (e.g., virologic failure, toxicity) and that cumulative exposure is a factor that must be considered. For the patients in this study, it is unclear how long these patients had XDDIs within their medication profiles, how quickly, if ever, they were resolved, and if any clinical sequelae occurred.
Second, some of the variables independently associated with XDDI after the addition of DAA therapy are not drug classes that are contraindicated in the prescribing information. 2 Thus, some of the predictors of XDDIs after the addition of DAA therapy may not be applicable to populations with differing medication use patterns. These variables may have been predictors of XDDI with the patients' underlying medication profile prior to the addition of DAA therapy or surrogates for disease severity that were not captured by data collection. Future studies should attempt to differentiate these factors.
Third, the armamentarium of HCV medications is evolving rapidly and a number of medications are still being developed to treat chronic HCV infection. While these data are currently contemporary, this type of study will most likely need to be replicated if new medications replace simeprevir and sofosbuvir as the standard of care.
Fourth, the study population was derived from two sources. Medication use patterns among Veterans' Affairs patients are largely driven by formulary management whereas for patients receiving care at the Upstate Medical University Hospital, decisions about medication use are driven by specific providers. As a result, the underlying distribution of specific medications being utilized may not be truly representative of all HIV/HCV-coinfected patients.
Fifth, the number of patients in the study population limited our ability to assess differences in XDDI frequency within ART drug classes. For instance, among patients receiving INSTIs, there were zero patients receiving dolutegravir, two patients on elvitegravir, and 37 on raltegravir.
Finally, we relied on an automated software program to determine the severity of drug–drug interactions. Other programs may not rank specific interactions the same way and future studies should delineate if the choice of software program truly matters when identifying XDDI.
In conclusion, the addition of SIM-containing treatment to our patients' medication profiles was associated with a significantly increased frequency of XDDIs compared to SOF-containing regimens among patients with HIV/HCV coinfection. Polypharmacy and/or the use of various antiretrovirals predicted the XDDIs. While our findings are strictly theoretical due to the nature of our study design, caution is clearly warranted when considering SIM-containing over SOF-containing treatment given the clear difference in the prevalence of XDDIs. While factors such as effectiveness, tolerability, and adherence need to be assessed when selecting an HCV treatment regimen, drug interactions also play an important role in distinguishing potential safety risks.
Footnotes
Acknowledgments
This material is based upon work partially supported by the Office of Research and Development, Department of Veterans Affairs. This article has greatly benefited from the thoughtful editing of Allison Krug.
Author Disclosure Statement
NP has purchased 5 shares of stock in Gilead Sciences (valued at $484.45 USD). All other authors have no pertinent disclosures.