
Abstract
Simple and reproducible tools to assess antiretroviral adherence are needed. A level of tenofovir diphosphate (TFV-DP) in dried blood spots (DBS) <1,250 fmol/punch is predicted to identify imperfect adherence. Herein we evaluated TFV-DP in DBS as a measure of adherence among HIV-infected women. DBS and peripheral blood mononuclear cells (PBMCs) were collected twice (∼1 week apart) in 35 well-controlled HIV-infected women [median age 42 years, 14 African American/black (AA)] receiving daily coformulated tenofovir/emtricitabine and either atazanavir/ritonavir (n=20) or raltegravir (n=16). TFV-DP in DBS and PBMCs was quantified by LC-MS/MS. Six-month adherence was measured as average days between monthly pharmacy refills. Data were loge transformed for analysis and presented as median (range); the correlation between continuous variables was analyzed using the Pearson correlation coefficient. The average TFV-DP between the two visits (aTFV-DP) in DBS and PBMCs was 1,874 (706–3,776) fmol/punch and 125 (1–278) fmol/106 cells, respectively. AA women had lower levels of aTFV-DP in DBS compared to whites (1,660 vs. 1,970 fmol/punch; p=0.04), with a viremic patient having the lowest drug levels (706 fmol/punch). Days between pharmacy refills were 34 (30–54) vs. 30 (26–40) in women with TFV-DP in DBS <1,250 vs. ≥1,250 fmol/punch (p=0.006). TFV-DP in DBS was negatively correlated with an increasing number of days between refills (r=−0.56, p=0.002). TFV-DP DBS was a reliable and objective measure of adherence in HIV-infected women based on a strong inverse relationship with pharmacy refill adherence.
D
A wide variety of nonpharmacological methods to monitor drug adherence are currently used. 8 –10 However, most of them overestimate adherence (e.g., self-reporting and pill counts), 11,12 are subject to high variability (e.g., patient self-report, pharmacy refill adherence, and pill counts), 13,14 or may not be cost effective in all clinical settings (WisePill, MEMS). 15,16 Similarly, pharmacological measures of adherence have various limitations and have yielded inconsistent results. For example, plasma ARV levels, which generally exhibit short half-lives, can be confounded by “white coat” compliance (i.e., improved adherence preceding clinic visits) and lead to imprecise assumptions about long-term adherence. 17 Drug moieties with longer half-lives, such as hair levels of ARVs, have proven to be highly informative measures of drug exposure and adherence, 18,19 but hair collection has not been implemented into routine practice as yet. Developing reproducible and objective measures of long-term adherence that can be applied to multiple clinical settings continues to be a priority in HIV clinical care.
We have recently proposed the use of intracellular levels of tenofovir diphosphate (TFV-DP) in red blood cells (RBC) measured with dried blood spots (DBS) as an objective and quantitative assessment of long-term drug exposure and adherence. 20 Tenofovir (TFV), a nucleotide analog widely used for the treatment of HIV infection, is phosphorylated to TFV-DP and trapped inside RBC with a 17-day half-life and 25-fold accumulation to steady state. The expected TFV-DP DBS level at steady state is 1,560 fmol/punch with daily dosing and <1,250 fmol/punch with less than daily dosing in HIV-negative subjects. 20 To date, whether TFV-DP in DBS correlates with currently available adherence measures in HIV-1-infected individuals remains unknown. The objective of this study was to determine the relationship between TFV-DP in DBS and drug adherence in HIV-infected women.
HIV-infected women receiving daily coformulated tenofovir disoproxil fumarate/emtricitabine (TDF/FTC) and either atazanavir/ritonavir (ATV/r) or raltegravir (RAL) were enrolled in the study. Women were eligible to participate if they had received TDF/FTC/ATV/r or TDF/FTC/RAL for at least 6 months, had a CD4+ T cell count ≥300 cells/mm3, and had an HIV RNA viral load (VL) <48 copies/ml. Blood samples for TFV-DP quantification in DBS, peripheral blood mononuclear cells (PBMCs), and plasma were collected twice per participant over a 2-week period. CD4+ T cell counts and HIV-1 RNA VL were obtained once per participant (at the second visit) and were determined by flow cytometry and Roche COBAS TaqMan 96 HIV-1, respectively, according to standard methods in the University of Colorado Hospital Clinical Laboratory (Aurora, CO). Six-month data of monthly medication refill records for ARVs were directly obtained from the participant's pharmacy and measured as the average days between refills. Approval was obtained by the Colorado Multiple Institutional Review Board and informed consent was obtained from all participants.
Intracellular TFV-DP in DBS was quantified using previously validated methods. 20,21 Briefly, 30 μl of blood from EDTA tubes was spotted onto 903 Protein Saver Cards (Whatman/GE Healthcare, Piscataway, NJ), allowed to dry for at least 2 h, and placed in plastic bags with humidity indicators, which were stored in a sample box with desiccant at −20°C. At the time of extraction, a 3-mm-diameter disc was punched from the DBS using a micropuncher, extracted with 500 μl of 70:30 methanol-H2O with sonication, and stored at −80°C until analysis. PBMCs were isolated with an RBC lysis step and counted with an automatic cell counter (Countess; Invitrogen, Carlsbad, CA). Cells were lysed with 500 μl of 70:30 methanol-H2O and stored at −80°C. Supernatants derived from DBS and PBMCs were analyzed using LC-MS/MS as previously described. 21 Plasma levels of TFV were measured using a validated LC-MS/MS method, as previously described. 22
Statistical analysis was conducted using GraphPad Prism version 6.00 for Windows (GraphPad Software, La Jolla, CA,
A total of 36 women (14 African American/black, 10 Hispanic) were enrolled in the study. The median (range) age of the study population was 42 (28–75) years, with an average time between visits of 9 days. The third component of the ARV regimen was ATV/r in 20 (56%) and RAL in 16 (44%) participants, with a median (range) duration of current regimen of 3 (0.5–10) years. CD4+ T cell and Hct data were available for 34 subjects with a median (range) of 654 (269–1,615) cells/mm3 and 41 (33–48)%, respectively. HIV-1 VL was also available in 34 participants and was <20 copies/ml in 31 participants, <200 copies/ml in two participants, and 20,600 copies/ml in one participant. The median (range) sCr was 0.8 (0.58–1.31) mg/dl.
TFV-DP quantification in DBS and PBMCs and TFV in plasma was available for 35 women (34 women in both visits, one woman in only one visit). The median (range) aTFV-DP in DBS and PBMCs was 1,874 (706–3,776) fmol/punch and 125 (1–278) fmol/106 cells, respectively, with a significant correlation between DBS and PBMCs, r=0.63, 95% CI (0.37–0.79), p<0.0001. The median aTFV in plasma was 88 (5–299) ng/ml, and was correlated with aTFV-DP in DBS, r=0.43, 95% CI (0.11–0.67), p=0.01. This correlation was influenced by a single point for which the plasma aTFV was below the LLOQ (described further below), and significance was lost when the point was removed from the analysis (p=0.15). TFV-DP in DBS had significantly lower between-visit percent differences and coefficient of variation (CV) compared to TFV-DP in PBMCs and TFV in plasma. The median (range) differences between visits were 8.5 (0.4–29.8)% vs. 21.9 (2.4–93.2)% and 27.3 (2.2–86.7)%, p<0.0001, respectively. The CVs, which account for interindividual (biological), analytical, and adherence variability, were 39% vs. 49% vs. 69%, respectively, demonstrating lower variability in DBS due to the long half-life of TFV-DP and to the standardized number of RBCs contained in a 3-mm DBS punch.
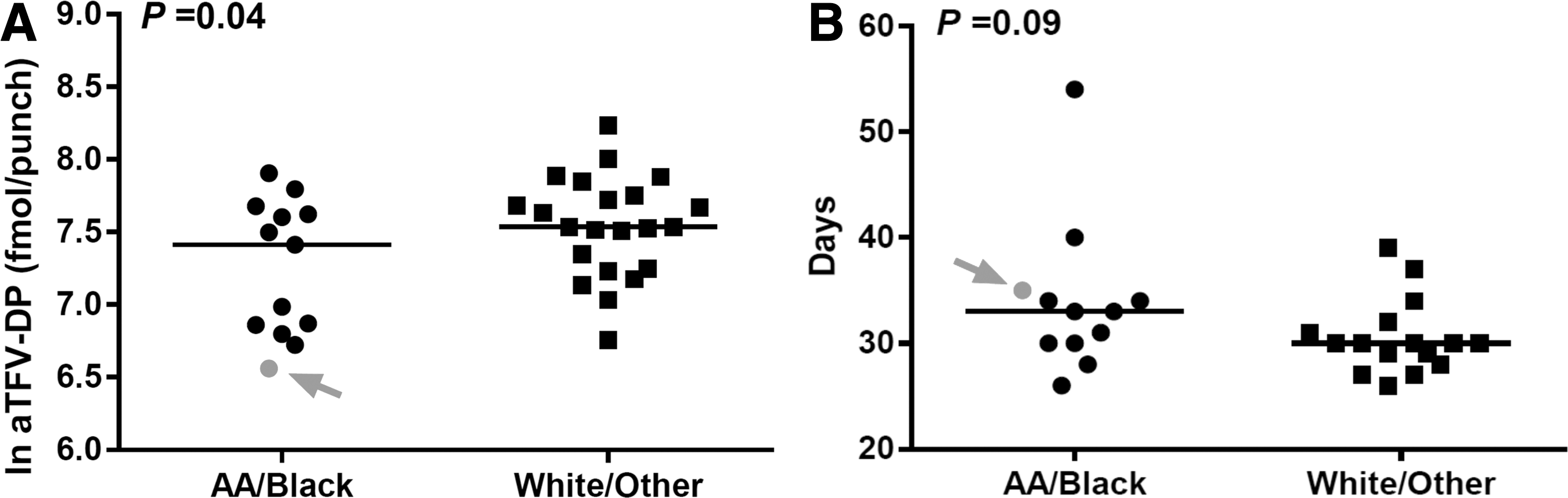
The aTFV-DP in DBS and PBMCs differed by race, with significantly lower median (range) levels in African American/black women compared to white women, 1,660 (706–2,717) vs. 1,970 (860–3,776) fmol/punch, p=0.04 in DBS (Fig. 1) and 100 (1–160) vs. 129 (54–278) fmol/106 cells, p=0.04 in PBMCs. No significant correlation between aTFV-DP in DBS with age, duration of ARV therapy, or sCr was identified (p>0.15). Furthermore, there was no influence of Hct on the aTFV-DP in DBS (p=0.56), which is consistent with our previous observations that Hct and RBC/μl encompassing the normal range did not significantly impact TFV-DP concentrations in DBS. 23 Lastly, the aTFV-DP concentration in DBS was not significantly different when compared by a third ARV component (ATV/r vs. RAL, p=0.68).
aTFV-DP (ln) in DBS
Six-month pharmacy refill data were available for 28 participants (12 African American/black), with a median (range) of 30 (26–54) days between pharmacy refills. African American/back women had longer average days between pharmacy refills when compared to white women, median (range) 33 (26–54) vs. 30 (26–39) days, although this difference was not statistically significant (Fig. 1). There was a significant inverse correlation between the average days between pharmacy refills and the aTFV-DP in DBS, r=−0.56, 95% CI (−0.78 to −0.24), p=0.002 (Fig. 2), but not with aTFV-DP in PBMCs (p=0.10) or aTFV in plasma (p=0.54). No differences in these results were observed when the average days between pharmacy refills below 30 days were set to exactly 30 days (given the low likelihood of achieving >100% adherence).
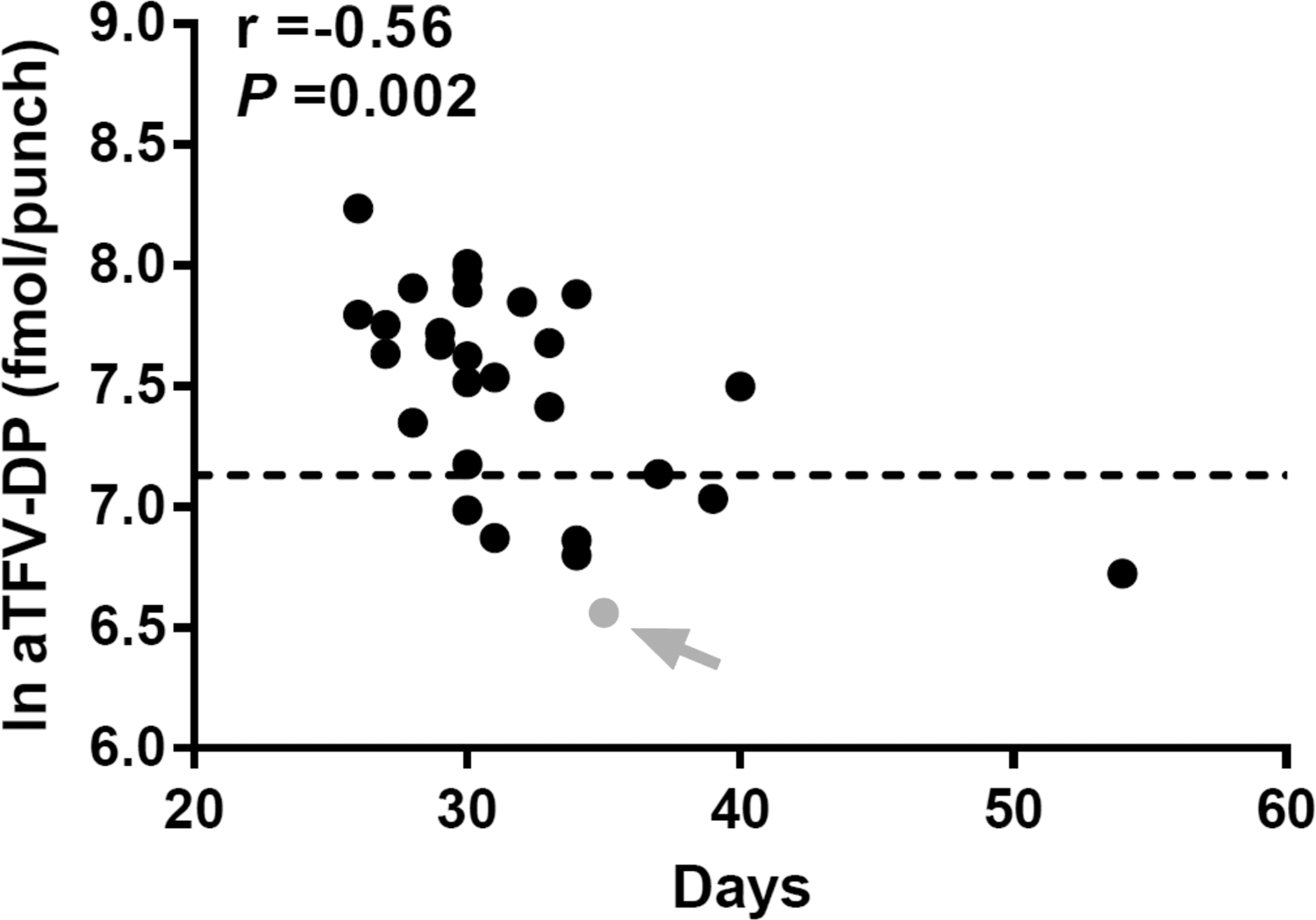
Correlation of aTFV-DP (ln) in DBS with days between pharmacy refills. The gray arrow indicates a woman with HIV VL >20,000 copies/ml. The dotted line indicates the threshold for daily dosing (1,250 fmol/punch). Pharmacy refill data were available for n=28 participants (n=7 with aTFV-DP level <1,250 fmol/punch). aTFV-DP, average tenofovir-diphosphate; DBS, dried blood spots. HIV VL, human immunodeficiency virus viral load.
When the daily dosing cutoff value of TFV-DP (<1,250 fmol/punch) was used, 20,24 23% (8/35) of women had less than daily adherence. Of these eight women, 75% were African American/black and 75% had undetectable VL (HIV VL unavailable in one woman). The median (range) average days between pharmacy refills were significantly longer in participants with an aTFV-DP <1,250 fmol/punch vs. ≥1,250 fmol/punch, 34 (30–54) vs. 30 (26–40) days, p=0.006. The median (range) aTFV-DP in the women with less than perfect adherence (based on DBS level <1,250 fmol/punch) was 926 (706–1,133) fmol/punch in DBS, which is predicted to be associated with four to five doses per week (57–71% adherence), 20 and 64 (1–160) fmol/106 cells in PBMCs. The viremic participant with an HIV VL >20,000 copies/ml had the lowest TFV-DP levels in DBS and PBMCs and was below the LLOQ for TFV in plasma at both visits, indicative of recent regimen discontinuation (for the two visits, 7 days apart: 830 and 583 fmol/punch for DBS; 2 fmol/106 cells and below LLOQ for PBMCs, respectively).
In this study we identified a strong relationship between TFV-DP in DBS, a novel pharmacological measure of cumulative drug exposure, and pharmacy refill data, which is frequently used to monitor adherence in HIV-infected individuals. Additionally, we demonstrated the strong reproducibility of TFV-DP in this matrix and robust correlation with PBMCs. Since the accumulation of TFV-DP in DBS is directly dependent on a continuous drug intake over a long period of time (i.e., weeks to months), this measure is not influenced by “white-coat” compliance, which is a major limitation of plasma drug levels with short half-lives. 17 In this way, DBS monitoring is analogous to ARV levels in hair, with the additional benefit that blood collection is part of routine clinical care and has the potential for at-home self-collection via fingerstick. Further studies are needed to compare DBS and hair in terms of convenience, patient acceptance, and biological and analytical variability.
While we identified suboptimal drug adherence in African American/black women according to their average days between pharmacy refills, this measure was not statistically significant. However, our cohort did demonstrate significant racial differences in aTFV-DP in DBS, with lower levels in African American/black women. This disagreement suggests that TFV-DP in DBS could be a more sensitive method to detect suboptimal adherence and that it may outperform currently available adherence measures. Alternatively, racial differences in TFV-DP levels in DBS could also be a potential explanation for this observation. Although previous studies have not identified an influence of race or sex on the pharmacokinetics of TFV-DP in RBCs, 25 larger studies are required to confirm this finding.
According to the aTFV-DP in DBS of <1,250 fmol/punch, almost 25% of our population showed less than daily dosing, which is consistent with previous observations. 2,26,27 Of note, the majority of these women had an HIV VL <20 copies/ml, which is of particular relevance because HIV VL is the main surrogate marker for ARV adherence used in clinical practice. Thus, TFV-DP in DBS may be able to identify a significant proportion of patients in whom suboptimal adherence would have otherwise been missed. Such patients may be on the cusp of clinically significant nonadherence and/or impending treatment failure. The TFV-DP level in the participant with viremia corresponded to an average drug intake of three doses per week. 20 The presence of viremia in this participant suggests that the thresholds for less than daily dosing and “nonsuppressive” adherence may be different. Further studies to identify these differences are required.
Our findings are consistent with current estimates for suppressive adherence thresholds of 70–80% with newer, more potent ARVs. 2,4,26,27 Even with this adherence “forgiveness,” several studies have demonstrated a multifactorial progressive decline in adherence over time, 28,29 which could ultimately lead to treatment failure, development of drug resistance, and increased HIV transmission. Thus, identifying nonadherence via an objective marker such as TFV-DP in DBS before any of these negative outcomes arise would have major clinical implications and should be further studied. We are currently evaluating DBS longitudinally to address this question.
In conclusion, measuring TFV-DP in DBS is a simple and reproducible method to quantify drug exposure and drug adherence in HIV-infected women on chronic TDF-based therapy. The ease in collection and processing of DBS enhances it applicability in various clinical settings and provides the potential to significantly increase the outreach of ARV adherence monitoring in HIV therapy.
Footnotes
Acknowledgments
This work was supported by grants from the National Institutes of Health, K23 AI104315 (J.C-M), U01 AI84735 (P.L.A.), and UL1 RR025780 (University of Colorado Clinical and Translational Sciences Institute) and by an investigator initiated grant from Merck #39423 (A.L.M.). We wish to express our gratitude to the women who participated in this study.
Author Disclosure Statement
Dr. Anderson reports the donation of the study drug and contract work with Gilead Sciences. Dr. Meditz received grant funding from Merck paid via the University of Colorado.