
Abstract
A recently diagnosed 22-year-old female with no history of transmission risk factors prompted a thorough investigation of possible alternative risk factors. As the patient had evidence of advanced disease and laboratory data compatible with long-standing infection, past events were reviewed. About 10 years ago the patient shared manicure utensils with an older cousin, later known to be HIV infected; this prompted the phylogenetic analysis of the HIV sequences of both patients. Phylogenetic analyses of partial HIV-1 polymerase and envelope sequences from both patients revealed highly related sequences, with an estimated common ancestor date (about 11 years ago) that coincided with the putative sharing of manicure instruments, during a time in which the cousin was not virally suppressed. Taken together, the information about the infection of this patient suggests the use of shared manicure instruments as an alternative route of fomite HIV-1 transmission.
T
A 22-year-old Brazilian woman, diagnosed with HIV infection after a first blood donation, was evaluated at the HIV/AIDS outpatient clinic, Santo Andre Infectious Diseases Ambulatory, Brazil. The patient (case) denied vaginal, anal, or oral sexual intercourse, blood transfusion, surgery, piercing, or tattooing. She had a boyfriend (seronegative by rapid check HIV test) for 2 years, but still had not engaged in sexual intercourse (a gynecological examination in August 2014 is compatible with the patient's statements). Her mother (seronegative by rapid check HIV test) confirmed that she was her biological mother and that the patient had never used blood products in childhood and had never suffered sexual violence. The patient reported no symptoms, but physical examination revealed oral candidiasis. She had an otherwise normal laboratory workup except for a low platelet count (115,000/ml), a low CD4 count (11 cells/mm3), and a viral load of 64,966 copies/ml (log 4,81).
Fluconazol and lamivudine/tenofovir/lopinavir/ritonavir were introduced. As the patient had no apparent transmission risk factor, a comprehensive review of all possible HIV acquisition routes was discussed independently by three attending physicians during subsequent visits. The only plausible mode of transmission was associated with events, about 10 years ago, when she remembered that at the age of 12 she used manicure instruments, including cuticle scissors, from an HIV-infected cousin. At that time the family did not know about the cousin' HIV infection. The cousin (putative index case, PIC) is a patient at the same clinic. She is a female manicurist, age 36 years, who was diagnosed 17 years ago during her third pregnancy. After she was diagnosed with HIV she used zidovudine and lamivudine until delivery, but was subsequently lost from follow-up. PIC remained without treatment for 5 years (1997–2003), a period that included the time of the putative transmission event. PIC did not remember any specific sharing event, but the case and her mother confirmed the occasional use of PIC's manicure instruments at home. Any other plausible risk, including any kind of relationship with a third party, as a common male partner, was denied. PIC was probably contaminated by the father of her third child, with whom she did not have a stable relationship. He did not partake of the family environment, making the possibility of sexual abuse unlikely, in agreement with the patient's and her mother's statements.
In 2003, PIC started zidovudine/lamivudine/nevirapine during her fourth pregnancy. Her first viral load, tested 10 days into treatment, was 7,530 copies/ml (log 3,88); it remained below the limit of detection until March 2008, when due to virological failure associated with irregular use of therapy, tenofovir/lamivudine/atazanavir/ritonavir was introduced. PIC has maintained undetectable viremia until her last evaluation in 2014.
Biological material was obtained after informed consent on separate occasions from both patients and processed and evaluated at the retrovirus laboratory, Adolfo Lutz Institute. Both patients had DNA from cell and RNA from plasma extracted and polymerase chain reaction (PCR) amplified in separate procedures, with the env and pol regions sequenced as previously described
3,4
(Supplementary Methods; Supplementary Data are available online at
Figure 1 depicts phylogenetic trees, constructed using BEAST v1.7.4, under the GTR+I+Γ model (Fig. 1a polymerase and Fig. 1b envelope). Four Markov Chain Monte Carlo (MCMC) runs were done independently; each MCMC run was 20,000,000 generations and was resampled every 2,000 generations. The runs were combined using LogCombiner after the consensus tree was obtained with TreeAnnotator. Trees were rooted with HIV-1 subtype C reference.
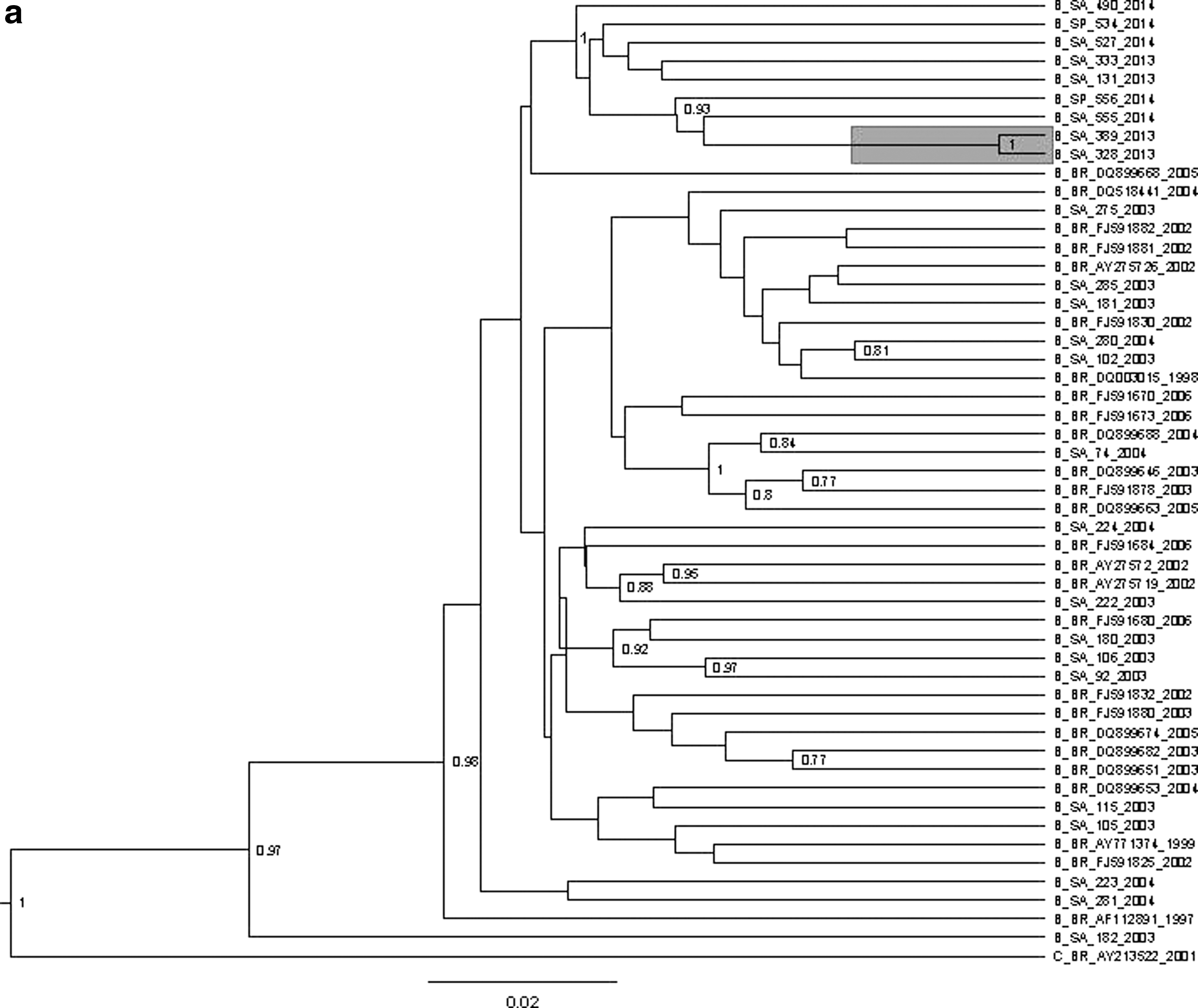
Phylogenetic trees of HIV-1 genome segments pol PR/RT (∼780 pb) and env c2-v3 (∼500 pb). B-Markov Chain Monte Carlo (MCMC) phylogenetic trees were constructed using the GTR+I+Γ model, based on four independent MCMC runs of four chains each, run for 20 million generations, combined using LogCombiner after the consensus tree was obtained with TreeAnnotator.
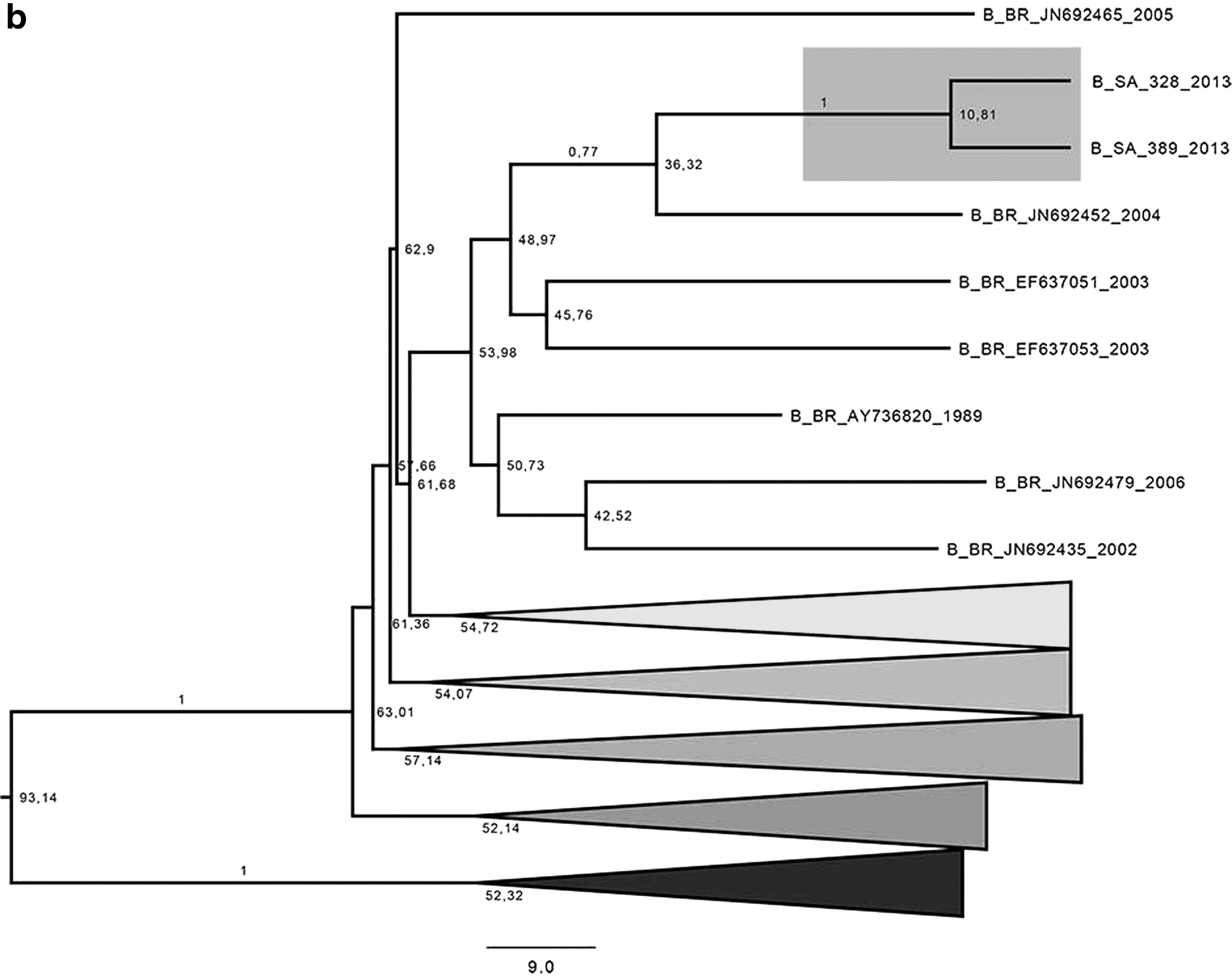
A representative pol phylogenetic tree was built using study cases and available sequences from naive and treated HIV-infected individuals followed at the same clinic, along with sequences from other areas of São Paulo and GenBank references (Fig. 1a). To trace the lineage of patients' sequences back in time, we evaluated env sequences with B-MCMC, 5 along with available subtype B envelope sequences from Brazil at GenBank covering position 6,800 to 7,500, excluding clones. Available HIV sequences obtained from other patients at the same clinic were also included, along with two subtype C references to root the tree (Fig. 1b). The estimated common ancestor date (about 11 years ago) corresponds to the period of the referred sharing of manicure instruments, a time when PIC was not virally suppressed. Sequences are available at GenBank with accession numbers KM360099 to KM360119 and KM489108 to KM489123.
With the phylogenetic data on hand, the case and PIC were further interviewed and the epidemiological data were confirmed. Although it is very difficult to determine the course of events occurring a decade ago and to guarantee that the use of the cosmetic paraphernalia was actually the mode of transmission, the HIV envelope and polymerase regions from both women are strongly related by phylogenetic parameters, and no alternative mode of transmission was identified. In a recent case of transmission among women, the CDC lists, along classical transmission routes, potential alternative sources that must be ruled out, such as tattooing, acupuncture, piercing, the use of shared sex toys between the partners and other persons, and exposure to body fluids, 6 but does not include manicure instruments. Our case raises the potential role of an additional fomite-related route of transmission of HIV-1.
Footnotes
Acknowledgment
Supported by FAPESP 2011/21958-2.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.