
Abstract
Antiretroviral therapy-related dyslipidemia increases the risk of cardiovascular disease (CVD) and is less frequently observed with nevirapine. Whether substituting rilpivirine for nevirapine has dyslipidemic consequences and alters CVD risk is unknown. The aim of this prospective open-label clinical trial was to evaluate serum lipids, cardiovascular risks, and lipid treatment goals over 48 weeks after switching from nevirapine to rilpivirine. Fifty HIV-1-suppressed patients on stable once-daily nevirapine plus emtricitabine/tenofovir-DF were switched to single-tablet rilpivirine/emtricitabine/tenofovir-DF. Lifestyle, weight, systolic blood pressure (SBP), ≥6 h overnight fasting lipids, 10-year Framingham risk scores (FRS), and Adult Treatment Panel III (ATP-III) lipid goals were evaluated over 48 weeks. Patients were 82% males, were a median of 45 years of age, and were on nevirapine for a median of 66 months. Diets, exercise levels, body mass index, and smoking status did not change during follow-up. At week 24, significant changes (p<0.001) were seen in mean [95% confidence interval (CI)] total cholesterol (−0.67 mmol/liter, CI: −0.50 to −0.83), low-density lipoprotein cholesterol (−0.36, CI: −0.21 to −0.51), and high-density lipoprotein cholesterol (−0.28, CI: −0.20 to −0.35). The total cholesterol/high-density lipoprotein cholesterol ratio increased 0.20 (CI: 0.02 to 0.37; p=0.029). Triglycerides did not change and the SBP decreased 6 mmHg (CI: −1.7 to −10.3; p=0.007). Week 48 lipid profiles and SBP were similar to week 24. The median FRS did not change during follow-up (−0.7%, p=0.119). More patients achieved ATP-III low-density lipoprotein cholesterol (+14.9%; p=0.016) and total cholesterol goals (+25.5%; p<0.001). The lipid profile changes after substituting rilpivirine for nevirapine did not significantly influence FRS, although SBP and the ATP-III low-density lipoprotein and total cholesterol goals improved.
HIV-1-
ART-induced dyslipidemia varies with the drugs used. The use of nevirapine in the 2NN, ARTEN, and OCTANE trials 6 –8 and rilpivirine in the ECHO, THRIVE, and SPIRIT trials 9 –12 has been associated with more favorable lipid profiles compared to efavirenz and protease inhibitors. In these large randomized clinical studies, rilpivirine and nevirapine had different effects on serum lipids. Rilpivirine had neutral effects on low-density lipoprotein cholesterol (LDL-C), total cholesterol (TC), and high-density lipoprotein cholesterol (HDL-C). The use of nevirapine resulted in a favorable HDL-C increase, although LDL-C and TC also increased.
Based on these results, nevirapine has been commonly used in HIV-1 patients at risk for CVD. Nonetheless, nevirapine is not recommended in first-line ART, 13 has significant toxicity, 14 and should not be used at higher CD4 counts. Nevirapine induces cytochrome P450 (CYP) 3A4, which causes drug–drug interactions and could lower the antilipid effects of statins. 15 In contrast to nevirapine, rilpivirine is recommended in first-line ART, is better tolerated, and does not significantly influence CYP3A4. Rilpivirine could therefore be preferred over nevirapine as a nonnucleoside reverse transcriptase inhibitor in antiretroviral regimens.
However, whether the substitution of rilpivirine for nevirapine has dyslipidemic consequences and alters the risk of CVD is unknown. This trial evaluates changes in serum lipids, cardiovascular risks, and lipid treatment goals over 48 weeks after switching from nevirapine to rilpivirine in HIV-1 patients.
In this prospective, open-label clinical trial, HIV-1 patients were switched from once daily nevirapine plus emtricitabine/tenofovir-DF to once daily coformulated rilpivirine/emtricitabine/tenofovir-DF. Participants were HIV-1-infected patients, 18 years or older, using nevirapine plus emtricitabine/tenofovir-DF for over 9 months with plasma HIV-1 RNA levels <50 copies/ml for at least 6 months. Patients with historically documented virological failure, baseline resistance, an estimated glomerular filtration rate <60 ml/min, the inability to use rilpivirine with a meal of at least 500 kcal, pregnancy, or concomitant proton-pump inhibitor use were excluded. We collected demographical data and medical history at baseline. Patients visited the outpatient clinic and we assessed (changes in) diet, recommended exercise levels (30 min of moderate exercise minimal 5 days/week), 16 comedication, smoking status, self-reported adherence with pill counts, weight, body-mass index (BMI), and automatic blood pressure measurements at baseline, week 4, week 12, week 24, and week 48. Overnight fasting (≥6 h) TC, LDL-C, HDL-C, triglycerides (TG), TC/HDL-C ratios, and glucoses were measured at all time points.
We evaluated the changes in TC, LDL-C, HDL-C, TG, TC/HDL-C ratio, glucose, blood pressure, and BMI during 48 weeks of follow-up. The 10-year risk on CVD was estimated by using the Framingham risk score (FRS) of the Copenhagen HIV Program. 17,18 The Adult Treatment Panel III (ATP-III) criteria of the National Education Cholesterol Program were used to categorize TC, LDL-C, HDL-C, and TG. 19 In short, the FRS stratifies patients into low (<10.0%), intermediate (10.0% to 19.9%), or high (≥20.0%) risk groups on CVD. The ATP-III categories are CVD or FRS >20.0% (high risk), ≥2 risk factors on CVD with FRS <20.0% (intermediate risk), and <2 risk factors (low risk). Smoking, hypertension, unfavorable HDL-C, familial premature CVD, and age each counts as one risk factor.
The ATP-III LDL-C levels (mg/dl×0.0259 equals mmol/liter) are categorized into <2.59 mmol/liter (optimal), 2.59 to 3.36 mmol/liter (near optimal), 3.37 to 4.13 mmol/liter (borderline), 4.14 to 4.91 mmol/liter (high), and ≥4.92 mmol/liter (very high). Depending on the ATP-III risk category, the LDL-C treatment goals are <2.59 mmol/liter for patients at high risk, <3.37 mmol/liter for patients at intermediate risk, <4.14 mmol/liter for patients at low risk, and <4.92 mmol/liter for patients without risk factors on CVD. TC is classified in ATP-III as desirable (<5.18 mmol/liter), borderline (5.18 to 6.19 mmol/liter), and high (>6.19 mmol/liter). An HDL-C above 1.04 mmol/liter is favorable and TG below 3.89 mmol/liter is considered normal according to ATP-III.
The data are described as means with 95% confidence intervals (95% CI) or standard errors of mean, medians with interquartile ranges (IQR), or numbers with percentages, when appropriate. Paired t-tests were used to analyze the changes in serum lipids, glucose, BMI, and blood pressure between baseline and week 24 and between week 24 and week 48. The Wilcoxon signed-rank test was used to evaluate the change in median FRS. McNemar's test was used to compare changes in FRS categories and ATP-III treatment goals between baseline and week 24. A two-sided p value was prespecified at 0.05. Analyses were done with SPSS 21.0 and Graphpad Prism 5.0.
All included patients provided written informed consent after at least 7 days of consideration. The study was approved by the institutional ethics review board and was done in accordance with good clinical practice and the Helsinki Declaration. The trial was registered at
Table 1 shows the baseline demographic data, anthropometrics, and metabolic parameters of the 50 included participants. Patients were mostly white men having sex with men in the fourth decades of their lives. They used nevirapine for a median of 66 months and had a median CD4 count of 565 (IQR: 470–730) cells/mm3. Nevirapine was used as first-line cART in 26 patients; 24 patients had switched to nevirapine from efavirenz (N=14) or protease inhibitors (N=10) because of side effects or for convenience reasons. Thirty patients (60%) were smokers or former smokers, nine (18%) were on antihypertensive treatments or had a history of hypertension, and one patient had well-controlled diabetes type-II. One patient had previous CVD. Two patients used statins for over 6 months prior to study entry. Their statin dosages remained unchanged on follow-up. Nine patients achieved the recommended exercise levels. No changes in diets, physical exercise levels, or smoking status were reported by the patients over 48 weeks and no additional lipid-lowering therapies were initiated. Three patients discontinued the study because of the side effects of rilpivirine or because of study noncompliance. Forty-seven patients (94%) completed the study and were included in the analysis. None of the 47 patients experienced virological failure during 48 weeks of follow-up.
Categorical variables are numbers (%) and continuous data are medians (IQR).
BMI, body mass index; BP, blood pressure; HDL-C, high-density lipoprotein cholesterol; IQR, interquartile range; LDL-C, low-density lipoprotein cholesterol; MSM, men having sex with men; NVP, nevirapine; TC, total cholesterol; TG, triglycerides.
The mean lipid changes from baseline to week 48 are shown in Fig. 1. By week 24, the mean (95% CI) TC decrease was −0.67 (−0.50 to −0.83; p<0.001). The HDL-C decreased −0.28 (−0.20 to −0.35; p<0.001) and the LDL-C decreased −0.36 (−0.21 to −0.51; p<0.001). The TC/HDL-C ratio increased significantly by+0.20 (0.02 to 0.37; p=0.029) and TG decreased nonsignificantly by −0.14 (−0.29 to 0.01; p=0.074). Glucoses were similar at baseline and week 24 (p=0.786). The systolic blood pressure decreased a mean of −6.0 mmHg (95% CI: −1.7 to −10.3; p=0.007). The diastolic blood pressure (−0.6 mmHg, 95% CI: −3.1 to 1.9; p=0.613) and BMI (+0.2 kg/m2, 95% CI: −0.1 to 0.5; p=0.113) did not change over 24 weeks. Excluding the two patients on statins did not influence the changes in TC (−0.66), HDL-C (−0.28), LDL-C (−0.35), ratio (+0.21), or TG (−0.13) over 24 weeks. The changes in LDL-C or systolic blood pressure were not observed in the included African patients. Week 48 lipids, glucose, blood pressure, and BMI did not change significantly compared to week 24 (p=0.228 or higher for all).

The mean changes (SEM) in fasting serum lipids (in mmol/liter) and TC/HDL-C ratio over 48 weeks in HIV-1-infected patients after a nevirapine to rilpivirine switch. HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; SEM, standard error of mean; TC, total cholesterol; TG, triglycerides.
The median FRS decreased nonsignificantly (p=0.119) from 8.4% (IQR: 2.8 to 20.3) at baseline to 7.7% (IQR: 2.2 to 16.9) at week 24 (Fig. 2). The distribution of patients between the FRS categories did not change significantly between baseline and week 24 (p=0.5); four patients decreased and one patient increased in FRS category from baseline to week 24. The patients' baseline and week 24 systolic blood pressures were used to calculate their FRS at these respective time points.

Framingham risk scores at baseline on nevirapine and at week 24 on rilpivirine. Patients have low (<10%, dots), intermediate (10–20%, triangles), or high (>20%, squares) 10-year risk of cardiovascular disease. The solid lines are the median Framingham risk scores. Each symbol represents the Framingham risk score category of an individual patient. The symbols for each patient at week 24 represent the patient's baseline Framingham risk score categories.
Figure 3 shows ATP-III lipid treatment goals at baseline and week 24. At week 24, 76.6% (36/47) of patients had desirable TC levels according to ATP-III treatment goals compared to 51.1% (24/47) at baseline (difference: 25.5%; p<0.001). For LDL-C, 22/47 (46.8%) patients did not achieve the desired LDL-C levels according to their ATP III risk categories at baseline. These 22 patients included all 12 high-risk patients with FRS >20%. According to ATP III guidelines, lifestyle or (non)medical LDL-C lowering interventions were indicated in these patients. By week 24 on rilpivirine, 15/47 patients (31.9%) did not fulfill LDL-C treatment goals (difference: 14.9%; p=0.016). Two of the 12 patients with FRS >20% at baseline achieved the desired LDL-C level according to their ATP-III risk category on rilpivirine at week 24. HDL-C levels were below 1.04 mmol/liter in 5/47 patients (10.6%) at baseline and 14/47 patients (29.8%) at week 24 (difference: 19.2%; p=0.004). All patients had normal TG according to their ATP-III classification at baseline and week 24.
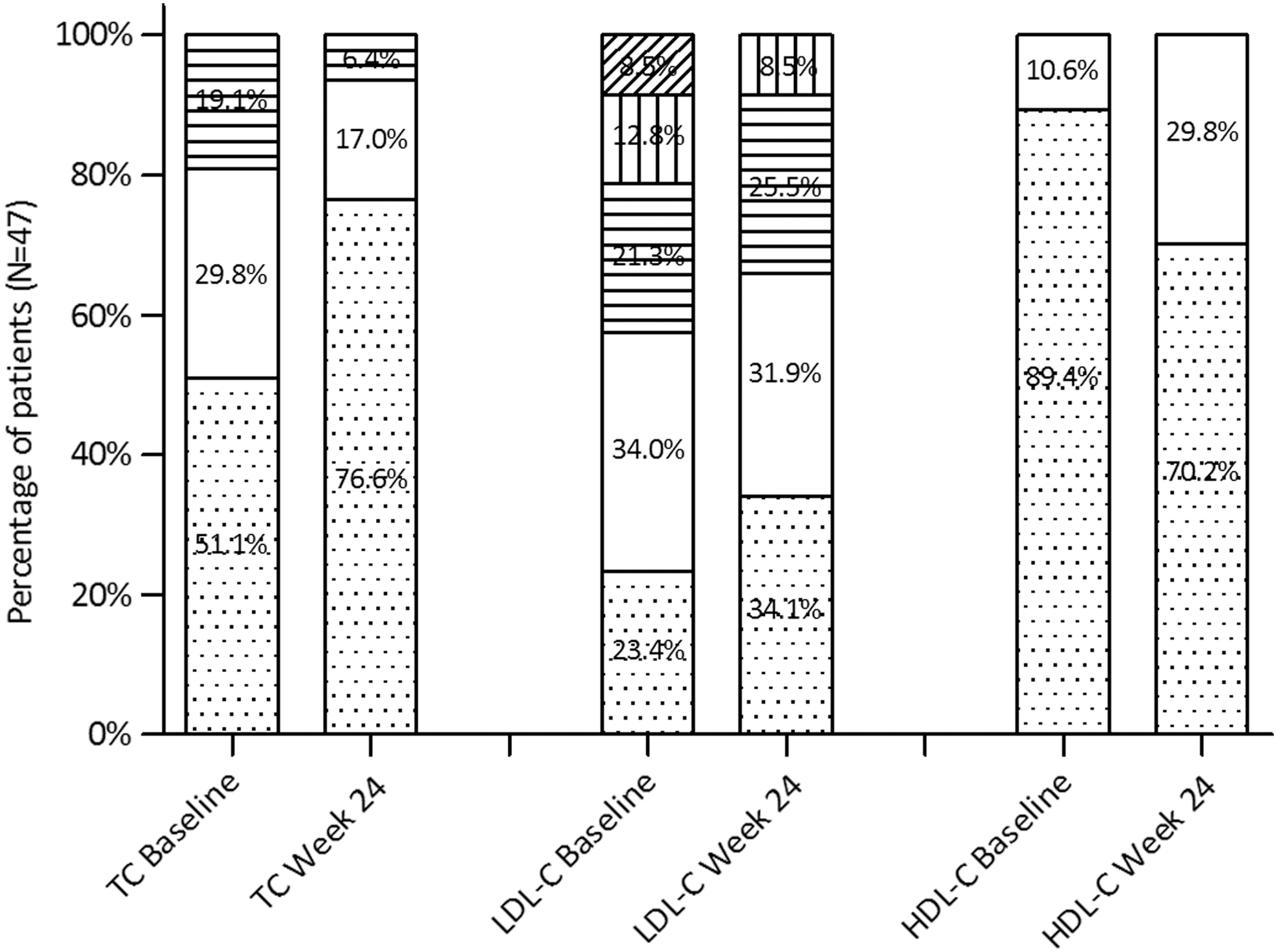
Distribution of Adult Treatment Panel-III recommended TC, LDL-C, and HDL-C levels at baseline on nevirapine and at week 24 on rilpivirine. Treatment categories from optimal to unfavorable for TC are <5.18 (dots), 5.18 to 6.19 (blank), or >6.19 mmol/liter (lines). Categories for LDL-C are <2.59 (dots), 2.59 to 3.36 (blank), 3.37 to 4.13 (horizontal lines), 4.14 to 4.91 (vertical lines), or ≥4.92 mmol/liter (diagonal lines), and categories for HDL-C are ≥1.04 (dots) or <1.04 mmol/liter (blank). HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; TC, total cholesterol.
In this study we show that after substituting rilpivirine for nevirapine in virologically suppressed HIV-1-infected patients the lipid profile changes did not result in significant alterations of the FRS on 10-year CVD. The systolic blood pressure decreased and significantly more patients achieved TC and LDL-C treatment goals after switching ART to rilpivirine. The results indicate that in patients at risk for CVD or with ART-related dyslipidemia, rilpivirine may be a good alternative for nevirapine. Patients who have to replace nevirapine for toxicity, for drug–drug interactions, or because a single tablet regimen is desired may switch to rilpivirine without a negative impact on their cardiovascular risk profiles.
This is the first study to evaluate the potential dyslipidemic consequences and CVD risk alterations after switching from nevirapine to rilpivirine in HIV-1 patients. Nevirapine is commonly regarded as the least atherogenic antiretroviral drug based on results from previous clinical trials. 20 HIV-1 patients using nevirapine had a higher mean HDL-C compared to patients on efavirenz, boosted atazanavir, or boosted lopinavir. 6 –8 The association between nevirapine and higher HDL-C was also observed in our study. An increased production of apolipoprotein A1, HDL-C's major apolipoprotein, in patients using nevirapine could be a possible explanation. 6,21
Whether a nevirapine-induced HDL-C increase results in antiatherogenic effects and prevents CVD has not yet been demonstrated. However, HIV-1 patients using nevirapine also had increases in LDL-C and TC levels. These LDL-C and TC alterations in patients using nevirapine were lower compared to efavirenz or boosted lopinavir but higher compared to boosted atazanavir. No LDL-C or TC increases were observed in patients using rilpivirine with emtricitabine/tenofovir-DF in contrast to patients using efavirenz, 9 –11 and LDL-C and TC levels were lower in patients using rilpivirine compared to boosted protease inhibitors. 12 The use of rilpivirine was not associated with major changes in HDL-C in these trials. Although a lower HDL-C is a risk factor for CVD, the LDL-C remains the primary target of cholesterol-lowering therapy according to ATP-III. The results of our study indicate that the use of rilpivirine might aid in achieving LDL-C treatment goals. The LDL-C lowering effects of statins metabolized by CYP3A4 might be more pronounced by the use of rilpivirine instead of nevirapine, although this hypothesis needs additional confirmation.
This study has limitations. First, no control group of patients on nevirapine was included for comparison of lipid profiles and CVD risks as the participants were their own controls. This study's conclusions would be strengthened if the study outcomes were observed in patients randomly assigned to continue nevirapine or to initiate rilpivirine. A more detailed diet and exercise registration would aid the interpretation. Selection bias of motivated patients could have positively influenced the results. The generalizability of these results to less frequently monitored patients, or to patients from various ethnicities, remains to be elucidated.
The follow-up of 48 weeks was sufficient to observe the initial changes and plateauing of metabolic parameters but was too short to evaluate the effects on lipids and CVD risk alterations on morbidity and mortality. Furthermore, lipids and medical cardiovascular risk management should be considered in addition to maintaining a healthy lifestyle and smoking cessation. Finally, unexpected findings without direct plausible biological mechanisms, such as the blood pressure changes, should be interpreted with caution and confirmed in future studies. The Hawthorne effect (change in behavior due to the study participation) could explain the observed blood pressure changes. However, an increased systolic blood pressure on nevirapine has been observed previously in the randomized OCTANE trial. 8 Despite the study limitations, the observed lipid and blood pressure changes were highly significant. It is therefore unlikely that larger studies would find completely different results, which would indicate that our observations occurred solely due to chance.
In conclusion, we did not observe relevant alterations in FRS as a consequence of changed fasting lipid profiles after substituting rilpivirine for nevirapine, although significantly more patients achieved LDL-C and TC ATP-III treatment goals and the systolic blood pressure improved on rilpivirine. Our study results indicate that rilpivirine could be used as an alternative for nevirapine as a treatment option for HIV-1 patients at risk for CVD.
Footnotes
Acknowledgments
We thank the patients who made this study possible and Rosa Meijer for key statistical input.
C.R., A.V., and B.R. designed the study and collected and analyzed the data. C.R. and B.R. wrote the first drafts of the manuscript. A.V. reviewed the manuscript for important intellectual content. The final manuscript was seen and approved by all authors.
This investigator initiated trial was supported by Gilead Sciences who had no influence in the conduct or analysis of the trial.
Clinical trials registration number: NTR3368,
Author Disclosure Statement
Casper Rokx reports lecture payment, travel expenses from ViiV Healthcare/MSD/Gilead outside the context of the submitted work. Bart J.A. Rijnders discloses research grants, board memberships, consultancy, lecture payment, travel expenses from Gilead/MSD/BMS/Janssen-Cilag. Annelies Verbon reports a research grant from Gilead outside the context of the submitted work.