
Abstract
The aim of this study was to assess whether hepatitis C virus (HCV) coinfection would affect the clinical and immunological outcome of HIV-infected patients following a simplification strategy. A prospective cohort of HIV-infected patients starting a ritonavir boosted darunavir monotherapy (mtDRV/rtv) was followed for 24 months. HCV infection was evaluated by HCV viremia and hepatic fibrosis. Immune activation was studied as HLA-DR CD38 coexpression on CD4+ and CD8+ T cells and also the quantification of plasma sCD14 levels. Microbial translocation was studied by the plasma levels of 16S rDNA and lipopolysaccharide (LPS). A total of 150 HIV-infected patients were enrolled in this study, including 46 individuals also infected with HCV (30.6%). HIV/HCV coinfection did not decrease mtDRV/rtv efficacy, since similar rates of HIV-1 intermittent viremia (HCV: 26.6% vs. no-HCV: 34.7%) and episodes of virological failure (HCV: 22.2% vs. no-HCV: 11.2%, p-value = 0.381) were found. No major differences were found between both groups at baseline, although higher HLA-DR+CD38+CD4+ T cell counts were found in the coinfected group (HCV: 6.65% vs. no-HCV: 4.55%, p-value = 0.032); this difference was maintained in the 24 months of follow-up. After the 24-month follow-up, both groups, HIV-monoinfected patients and HIV/HCV-coinfected patients, presented similar immune activation and microbial translocation profiles. In conclusion, the use of a simplified mtDRV/rtv strategy compromises neither HIV nor HCV viremic control in coinfected patients, although a higher immune activation of CD4+ T cells was found.
Introduction
P
Materials and Methods
A prospective cohort of HIV-1-infected adult patients who started a regimen of ritonavir boosted darunavir monotherapy (mtDRV/rtv, 800/100 mg once daily) at the University Hospital Virgen del Rocío, Sevilla, Spain, was followed for 24 months. 11 All enrolled patients were on HAART prior to the initiation of mtDRV/rtv and on viral suppression for at least the previous 6 months. This cohort was chosen because all recruited patients followed the same antiretroviral treatment, avoiding any potential interactions between anti-HIV-1 drugs and HCV infection. 12,13 HCV infection was defined as the presence of detectable HCV-RNA levels and anti-HCV antibodies. Enrolled patients must have been on viral suppression for at least the previous 6 months and must lack any protease gene mutations that would confer a decreased susceptibility to darunavir, according to the International AIDS Society guidelines. 14 Pregnancy, HBV infection, or concomitant use of drugs with potential major interactions with darunavir were considered as exclusion criteria. The study was designed and conducted according to the principles of the Declaration of Helsinki and was approved by the Spanish Agency of Medicines and Healthcare Products and the Coordinating Committee on Ethics in Biomedical Research of Andalucía. All patients gave informed consent.
Patients' assessments were performed at baseline, after the first month on treatment, and every 3 months thereafter, including biochemical and hematological profiles, CD4+ T cells counts, and plasma HIV-1-viremia (COBAS AmpliPrep/COBAS TaqMan HIV-1 Test, version 2.0, Roche Diagnostic, Basel, Switzerland). Virological failure was defined as two consecutive HIV-1 loads over 200 copies/ml. Blips were defined as transitory episodes of HIV-RNA loads over 50 copies/ml, preceded and followed by plasma viral loads <50 copies/ml, without changes in antiretroviral therapy, whereas intermittent viremia was defined as all viremic episodes of detectable plasma HIV-RNA load during follow-up not meeting blips or virological failure criteria. HCV genotypes and subtypes were determined using the Inno-Lipa HCV II test (Bayer, Barcelona, Spain), while plasma HCV-RNA levels were measured by the Cobas TaqMan qPCR assay (Roche Diagnostics, Basel, Switzerland).
Blood samples were collected in Vacutainer cell preparation tubes (BD Biosciences, Madrid, Spain) at month 0 (m0), and 6, 12, 18, and 24 months after the initiation of mtDRV/rtv. Only patients with available samples in all these time points were enrolled in the study. IA profiles were measured as the coexpression of HLA-DR and CD38 in both CD4+ and CD8+ T cells, in addition to the naive, central memory, and effector memory subsets by flow cytometry, as previously described. 15
Microbial translocation (MT) was assessed by two different markers: lipopolysaccharide (LPS) and 16S rDNA. Plasma bacterial LPS was measured using the QCL-1000 Limulus Amebocyte Lysate kit (Lonza, Basel, Switzerland) following the manufacturer's instructions. Briefly, Plasma samples used for LPS determination were collected in EDTA vacutainer tubes, since this showed less of an inhibition profile than heparin, and stored in LPS-free glass tubes to prevent loss of endotoxin to plastic tube walls. All materials used for the assay were rendered LPS free. Plasma samples were diluted to 20% with endotoxin-free water and then heated to 70°C for 10 min to inactivate plasma proteins. Plasma 16S rDNA levels were measured by quantitative polymerase chain reaction (PCR), as previously described. 16 Additionally, plasma sCD14 levels were assessed as a surrogate marker of MT, showing the activation profile of monocytes-macrophages, using the Human sCD14 Quantikine ELISA kit (R&D Systems, Abingdon, UK) following the manufacturer's instructions.
Results were expressed as median and interquartile range (IQR) for continuous variables and number of cases and percentages for categorical variables. The Kruskal–Wallis H and ANOVA tests were performed to compare continuous variables and the χ2 and Fisher's exact tests were run to compare categorical variables. The differences were considered statistically significant for p-values <0.05. The statistical analyses were performed using SPSS software (v. 19.0, Chicago, IL).
Results
A total of 150 white patients were enrolled in this prospective cohort, with 46 individuals showing detectable HCV-RNA levels (30.6%). These HIV-infected patients exhibited a long history of HCV coinfection, with a median time of 207 months (157–240 months), with a median liver fibrosis of 5.2 kPa (4.8–6.7 kPa). No major differences in terms of viral control were found among monoinfected and coinfected patients, since similar rates of virological failure (HCV: 22.2% vs. no-HCV: 11.2%, p-value = 0.381) and intermittent viremia (HCV: 26.6% vs. no-HCV: 34.7%, p-value = 0.381) were found among them. All patients with virological failure reachieved viral suppression within the following 4 weeks either with the reinforcement of adherence or the addition of two nucleoside retrotranscriptase inhibitors to their current antiretroviral therapy.
Due to sampling limitation only 56 patients were enrolled for further analyses, including 12 HCV-coinfected patients with detectable HCV-RNA levels (21.4%). No major differences were found among both groups at baseline (Table 1). However, HIV/HCV-coinfected patients had higher levels of HLA-DR+CD38+CD4+ T cells (HCV: 6.65% vs. no-HCV: 4.55%, p-value = 0.032).
Results are expressed as median (M) and interquartile range (IQR) or number of cases (n) and percentages (%).
HCV, hepatitis C virus; HAART, highly active antiretroviral treatment; LPS, lipopolysaccharide; HDL, high-density lipoprotein; LDL, low-density lipoprotein.
HIV/HCV-coinfected patients presented lower CD4+ T cell counts in the 24 months of follow-up (Fig. 1A) and, consequently, a lower CD4:CD8 ratio (Fig. 1B). Indeed, coinfected patients showed higher levels of central memory CD4+ T cells (HCV vs. no-HCV: m0 = 20.1% vs. 19.4%; m6 = 22.6% vs. 14.7%; m12 = 18.8% vs. 17.4%; m18 = 32.4% vs. 21.0%; m24 = 34.3% vs. 26.3%; p-value = 0.075), but lower levels of naive CD4+ T cells compared to HIV-monoinfected patients (HCV vs. no-HCV: m0 = 38.5% vs. 42%; m6 = 34.7% vs. 45.4%; m12 = 37.0% vs. 42.3%; m18 = 37.8% vs. 45.7%; m24 = 28.7% vs. 41.1%; p-value = 0.036). When the IA profile was studied, HIV/HCV-coinfected patients showed significantly higher levels of HLA-DR+CD38+CD4+ T cells, which did occur for the CD8+ T cell subset (Fig. 1C and D, respectively).

Evolution along the 24 months of follow-up of CD4+ T cells counts
Furthermore, MT was assessed throughout the 24 months of follow-up, showing similar levels of plasma LPS and 16S rDNA between HIV/HCV-coinfected and HIV-monoinfected patients (Fig. 1E and F, respectively). Similar behavior was observed when plasma sCD14 levels were analyzed, since no significant differences were found between both groups of patients during the 24 months of follow-up (HCV vs. no-HCV: m0 = 12.73 vs. 10.31 ng/ml; m6 = 13.17 vs. 10.45 ng/ml; m12 = 12.56 vs. 10.71 ng/ml; m18 = 9.85 vs. 10.63 ng/ml; m24 = 10.66 vs. 9.93 ng/ml; p-value = 0.306).
Finally, good correlations were found between the CD4:CD8 ratio and the percentage of HLA-DR+CD38 CD4+ T cells (ρ = –0.237, p-value = 0.0003, Fig. 2A), plasma sCD14 levels and the percentage of HLA-DR+CD38+ CD8+ T cells (ρ = 0.139, p-value = 0.036, Fig. 2B), and sCD14 and 16S rDNA levels (ρ = −0.463, p-value <0.0001, Fig. 2C). On a subanalysis of the HCV population, it was observed that those correlations more often held true among HIV/HCV-coinfected patients (ρ = −0.354, p-value = 0.009, Fig. 2D; ρ = 0.334, p-value = 0.014, Fig. 2E; ρ = −0.608, p-value <0.0001, Fig. 2F, respectively). Interestingly, a good correlation was found between liver fibrosis and HLA-DR+CD38+CD4+ T cells counts (ρ = 0.417, p-value = 0.043).
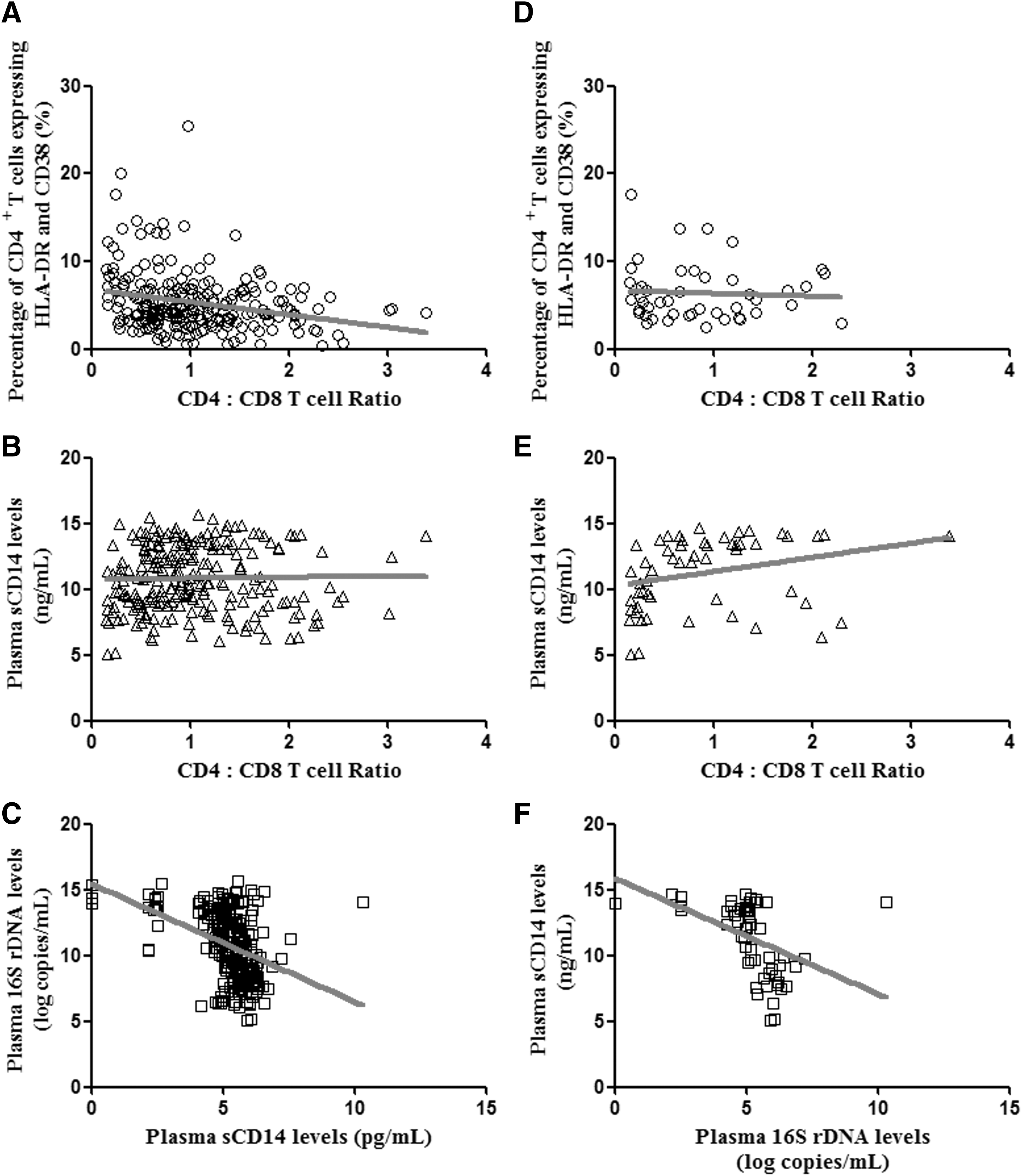
Correlations between immune activation and microbial translocation parameters along the 24 months of ritonavir boosted darunavir monotherapy (mtDRV/rtv) in the complete cohort
Discussion
About 15–30% of patients infected with HIV-1 are also infected with HCV, 17,18 experiencing higher values of HIV viremia and augmented rates of both disease progression and mortality. 19,20 HIV/HCV-coinfected subjects have increased levels of activated CD4+ T cells compared to HIV-monoinfected subjects. 21 –23 These higher levels could be explained by the increased number of antigens, a fact that would also explain the differences in naive and central memory counts between HIV-monoinfected and HIV/HCV-coinfected patients. Indeed, CD4+ T cell activation showed a good correlation with liver fibrosis, suggesting a direct interaction between the levels of fibrosis and IA. However, in our study the levels of activated CD8+ T cells, evaluated as the simultaneous expression of HLA-DR and CD38, were similar in coinfected and monoinfected subjects, with significant differences found only in the CD4+ T cell subset. 24 Indeed, these higher levels of HLA-DR+CD38+CD4+ T cells among coinfected patients were closely correlated with lower CD4+ T cell counts and, thus, with the CD4:CD8 ratio. Moreover, the correlation between the levels of HLA-DR+CD38+CD8+ T cells and sCD14 suggests a link between innate and adaptive immune activation among HIV/HCV-coinfected individuals.
It is worth noting that we did not observe changes in the IA profile throughout the 24 months of follow-up of these patients, either in HIV-monoinfected or HIV/HCV-coinfected patients, in agreement with previous studies. 25 These differences in the IA profile are not influenced by the number of HIV viremic patients in each group, since both groups showed a similar proportion of patients with intermittent viremia and virological failure (approximately 30%). Obviously the emergence of episodes of virological failure was intimately linked to increases in the IA profiles of both CD4+ and CD8+ T cells, as previously reported. 15
Previous studies have suggested that gut translocation is poorly controlled in HIV/HCV-coinfected patients. 26 This suggestion relies on the impaired liver function and thus impaired microbial clearance caused by HCV infection. However, we, as others, 25 have not observed this fact, since no significant differences among the 24 months of follow-up were found in LPS, 16S rDNA, or sCD14 levels. However, this observation should be corroborated by larger longitudinal studies. The main limitation of the study is the small number of patients with HIV/HCV coinfection with available samples, although the inclusion criteria were quite restricted since patients were selected from a cohort of mtDRV/rtv in order to avoid potential inhibition between antiretroviral drugs and HCV infection. 12,13
The observation that chronic HCV viremia is associated with lower CD4+ T cell counts and elevated levels of IA among this CD4+ subset strongly suggests that the mechanism that guides both phenomenon is tightly linked. 21,25 Thus, although in the absence of significantly higher levels of MT and IA, at least among CD8+ T cells, the significant differences found in CD4+ counts and IA suggest that the introduction of anti-HCV therapy might improve both facts, potentially avoiding higher levels of IA and subsequently a major risk for other clinical complications.
In summary, HIV/HCV-coinfected patients presented higher counts and higher IA in the CD4+ T cell subset, although no major changes were observed in CD8+ T cells and MT compared to HIV-monoinfected patients. Moreover, it is important to note that the use of a simplification monodrug therapy against HIV is not detrimental among HCV-coinfected patients, since similar viral control was found among HIV-monoinfected and HIV/HCV-coinfected patients.
Footnotes
Acknowledgments
The authors are indebted to their patients for their involvement in this study and M. Rodríguez, F. Cano, and R. Martin for their help with specimen processing. This work was partially presented in the 20th International AIDS Conference at Melbourne, Australia, July 20–25, 2014 (WEPE089).
This work was supported by a grant from Consejería de Salud y Bienestar Social, Junta de Andalucía (exp. P0077-2012).
Author Disclosure Statement
L.F.LC. and P.V. have received unrestricted research funding, consultancy fees, and lecture fees from and have served on the advisory boards of Abbott, Bristol-Myers Squibb, Gilead Sciences, Janssen-Cilag, Merck Sharp & Dohme, Roche España, and ViiV Healthcare.