
Abstract
We previously reported mother-to-child transmission of HIV-1 in nine (6.7%) of 135 children on nevirapine prophylaxis in Vietnam. In the current study, we investigated the appearance and profile of antiretroviral drug (ARV) resistance mutations, the predicted coreceptor usage, and the genetic diversity of HIV-1 strains isolated from the eight pairs of HIV-1-infected mothers and their children, who were followed up to 12 months after birth. Portions of the pol and env C2V3 regions of the HIV-1 strains were analyzed genetically. HIV-1 CRF01_AE RNA was detected in four (50%) children at delivery. Y181C, a nevirapine resistance mutation, appeared in two (25%) children 1 and 3 months after birth, respectively. No ARV resistance mutation was detected in the mothers, though three mothers were on ARV prophylaxis. Five mothers and their children harbored CCR5-tropic (R5) viruses. Two mothers harbored both R5 and CXCR4-tropic (X4) viruses, but their children harbored only R5 viruses even though the X4 viruses were dominant in the mothers. In the remaining one mother, HIV-1 RNA was not amplified and her child harbored both R5 and X4 viruses at birth, but only X4 virus 12 months after delivery. The infants' viruses were more homogeneous than their mothers' viruses (mean distance: 0.5% vs. 1.1%, respectively). This is the first molecular epidemiological study of vertical HIV-1 infections in Vietnam. These findings may provide useful knowledge for the prevention of mother-to-child transmission of HIV-1 and the antiretroviral treatment of children in Vietnam.
Introduction
V
The chemokine receptors CCR5 and CXCR4 are the main coreceptors for HIV-1 entry into target cells. 7 Based on chemokine coreceptor usage, HIV-1 can be classified as a CCR5-tropic (R5), CXCR4-tropic (X4), or dual tropic (R5X4) virus. 8 A strong selection for viral variants using CCR5 as a coreceptor occurs during transmission, as most children are infected with R5 viruses. 9 –12
Prevention of mother-to-child transmission (PMTCT) of HIV-1 is one of the key components of the worldwide response to the pandemic and is based on the prophylactic use of antiretroviral drugs (ARVs). In developed countries, MTCT of HIV-1 has been reduced to less than 2% by combination antiretroviral therapy (ART), selective caesarian delivery, and avoidance of breastfeeding. 13,14 In developing countries, single-dose nevirapine given to mothers infected with HIV-1 and their children in the intrapartum and immediate postnatal period is the most common intervention to reduce the MTCT of HIV-1. Single-dose nevirapine can reduce the risk of MTCT of HIV-1, 15 but it may lead to the emergence of nevirapine-resistant HIV-1 variants in children who are infected with HIV-1 despite the prophylaxis. 16 One study of HIV-1-infected Ugandan women and their children who received single-dose nevirapine to prevent MTCT showed nevirapine resistance mutations in 11 of 24 (46%) children by 6–8 weeks of age. 16
In Vietnam, the first pregnant woman infected with HIV-1 was reported in 1993. The number of HIV-1-infected pregnant women increased from 4,000 in 2007 to almost 5,000 in 2012, and the number of children living with HIV-1 increased from 3,750 in 2007 to 5,700 in 2012. 17 –19 PMTCT was officially introduced in Vietnam in 2006. According to the guidelines of the Vietnamese government in 2005, all HIV-1-infected pregnant women and their children should receive single-dose nevirapine free of charge. 20 However, of the HIV-1-infected pregnant women in Vietnam, only 9.2% in 2006, 32.3% in 2009, and 44.0% in 2011 had access to the PMTCT program, and 27.9% received single-dose nevirapine in 2011. 21 Most of the women who had access to the PMTCT program resided in urban areas, such as Hanoi and Haiphong. 18,21 One study reported that 7.6% of the HIV-1-infected pregnant women were on combination ARVs, 51.9% on single-dose nevirapine, and the remaining 40.4% without ARVs; only 46.2% of their children received single-dose nevirapine for PMTCT in 2008. 18
MTCT of HIV-1 was observed in nine (6.7%) of the 135 children, who were all on single-dose nevirapine prophylaxis and were born to mothers with and without ARV prophylaxis between 2004 and 2006 in Northern Vietnam. 22 However, limited data are available on the factors associated with vertical transmission of HIV-1, such as the transmission of drug-resistant HIV-1 and selection based on coreceptor usage in Vietnam.
In the present study, we investigated the appearance and profile of drug resistance-associated mutations in infants under nevirapine prophylaxis, the predicted coreceptor usage, and the genetic diversity of HIV-1 strains in mothers and their infants in Hanoi and Haiphong, Northern Vietnam.
Materials and Methods
Study subjects
A total of 135 HIV-1-infected mothers and their children admitted to the Obstetrics and Gynecology hospitals in Hanoi and Haiphong, Northern Vietnam, were enrolled in our previous study. 22 Blood samples were collected from the mothers on the day of delivery and from their infants within 1–2 days after birth between 2004 and 2006. Blood samples were also collected from the infants 1, 3, 6, and/or 12 months after birth, although some mother-and-child pairs, especially those who lived far from the hospital, could not come to the hospital at all the sample collection times. Plasma was separated from the blood samples within 8 h of collection and stored at −80° C until analysis.
For the current study 38 mother-and-child pairs including one with a child vertically infected with HIV-1 were excluded for the lack of their mothers' plasma samples. Plasma samples from the remaining 97 pairs were still available and transferred to Kanazawa University for further analyses (Fig. 1). Of the 97 children samples eight were confirmed to be positive for HIV-1 RNA (Table 1). Of the eight HIV-1-infected children, one (HP25) was born to a mother given zidovudine/lamivudine/nelfinavir 1–3 weeks before delivery, two (HN51and HN88) were born to mothers given single-dose nevirapine at delivery, and five (HN23, HN46, HN47, HN60, and HP13) were born to mothers without any prophylaxis. After birth, all children were given single-dose nevirapine (2 mg of liquid nevirapine/kg body weight) within 48 h of delivery and fed formula, and one child (HP25) whose mother received combination ART before delivery was given liquid zidovudine for 7 days after birth according to the Vietnamese national guidelines. 20 All of the plasma samples collected from the eight HIV-1-infected children within 1–2 days after birth were available, but only a part of the samples collected from these children 1, 3, 6, and/or 12 months after birth were available as shown in Table 1. None of the children visited any other institutes or started ARV during the follow-up.
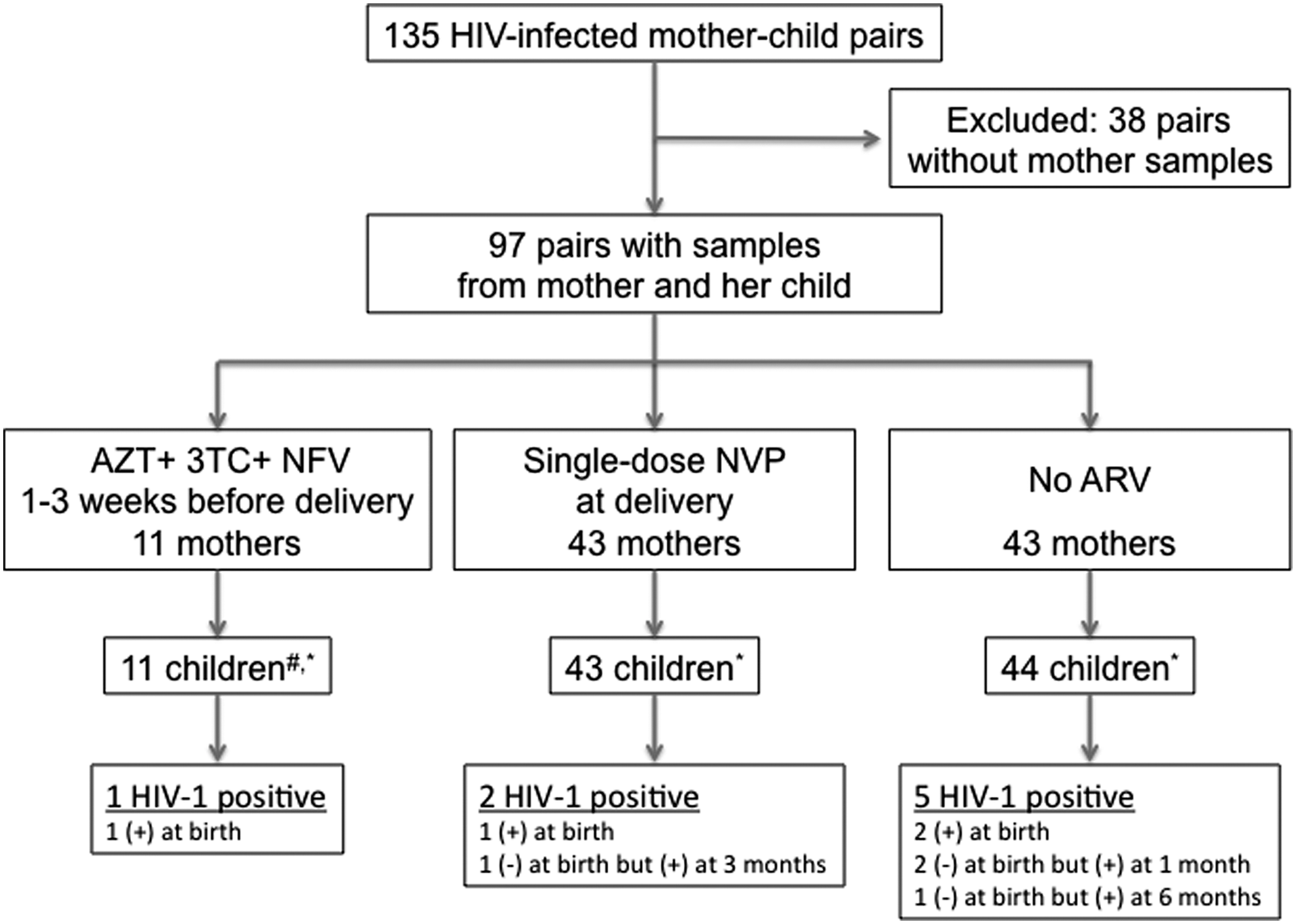
Mother-to-child transmission in the study group. AZT, zidovudine; 3TC, lamivudine; NFV, nelfinavir; NVP, nevirapine. #AZT liquid was administered for 7 days after birth. *All children were given single-dose liquid nevirapine within 48 h of birth and fed with formula.
M, mother; C, children; C-0, at delivery; C-1, 1 month; C-3, 3 months; C-6, 6 months; C-12, 12 months after birth; NRTI, nucleoside reverse transcriptase inhibitors; NNRTI, nonnucleoside reverse transcriptase inhibitors; PI, protease inhibitor; None, no resistance mutation was detected. Italics, minor mutations; Bold, major mutation; R5, CCR5; X4, CXCR4; Fail, PCR (+) but population sequencing was not successful; n/a, no PCR amplification. Distance is expressed as the percent nucleotides or amino acid.
This study was approved by the ethical committees of the Hanoi National Hospital of Pediatrics, the National Institute of Hygiene and Epidemiology, the Obstetrics and Gynecology hospitals in Vietnam, and Kanazawa University in Japan.
RNA extraction, RT-PCR, cloning, and sequencing
RNA was extracted from 100 μl of plasma using the SMITEST EX-R&D nucleotide extraction kit (Genome Science Laboratories, Fukushima, Japan) according to the manufacturer's instructions. One-step reverse transcriptase polymerase chain reaction (RT-PCR) (SuperScript III One-step RT-PCR system with Platinum Taq DNA polymerase, Invitrogen, Carlsbad, CA) and nested PCR with AmpliTaq Gold (Applied Biosystems, Japan) or KOD FX (Toyobo, Osaka, Japan) were used to amplify HIV-1 pol and env.
The HIV-1 pol-PR region (coding amino acids 1 to 99) was amplified by nested RT-PCR with the primers DRPRO5/DRPRO2L in the first round and DRPRO1M/DRPRO6 in the second round. The HIV-1 pol-RT region (coding amino acids 1 to 220) was amplified using the primers DRRT1L/RTout in the first round and DRRT7L/DRRT6L in the second round. To amplify HIV-1 pol-RT, the primer pairs RT18/K104 and K101/K102 were used in the first and second round, respectively, when the PCR reaction with the previous primer pairs failed. 23 –25 RT-PCR was performed with one cycle at 55°C for 30 min and one cycle at 94°C for 2 min, then 40 cycles at 94°C for 15 s, 55°C (for DRPRO5/DRPRO2L and DRRT1L/RTout primer pairs) or 50°C (for the other primer sets) for 30 s, and 68°C for 1 min, with a final extension of 68°C for 5 min. 23 –25 Nested PCR for pol-PR was performed with one cycle at 95°C for 10 min, followed by 40 cycles at 95°C for 30 s, 55°C for 30 s, and 72°C for 1 min, with a final extension at 72°C for 10 min using Ampli Taq Gold. Nested PCR for pol-RT was performed with one cycle at 94°C for 1 min and 35 cycles at 98°C for 10 s, 55°C for 30 s (for DRRT7L/DRRT6L primer set) or 45°C for 30 s (for KT101/K102 primer set), and 68°C for 5 min using KOD FX. 23 –25
The HIV-1 env C2V3 region (366 bases) was amplified using the primers JA167mod/JA170mod in the first round and JA168mod/JA169mod in the second round. Amplification was performed with one cycle of 95°C for 2 min and 40 cycles of 95°C for 30 s, 55°C for 30 s, and 68°C for 1 min, with a final extension of 72°C for 10 min. 26
The amplified products were detected by staining the gel with ethidium bromide after electrophoresis. The amplified products of the PR and RT regions were sequenced directly with BigDye Terminator v1.1 on an ABI PRISM 310 Genetic Analyzer (Applied Biosystems). The amplified products of the env C2V3 region were cloned using the TOPO TA kit (Invitrogen) as described previously. 27 Eleven to 42 clones were sequenced for each sample using BigDye Terminator v1.1 on a 3500XL sequencer (Applied Biosystems).
Drug resistance
HIV-1 pol PR and RT sequences were analyzed for drug resistance mutations using the Stanford University HIVdb sequence analysis program (
Coreceptor usage
HIV coreceptor usage was predicted based on the net charge of amino acids in the env V3 region, which was calculated by subtracting the number of acidic amino acids [aspartate (D) and glutamate (E)] from the number of basic amino acids [lysine (K) and arginine (R)]. A net charge less than +5 in the V3 region has been shown to predict CCR5 usage (R5 virus), whereas a net charge of more than +5 has been shown to predict CXCR4 usage (X4 virus), and a net charge equal to +5 indicates R5 variants unless accompanied by an arginine or lysine residue at position 11 or 25 of the V3 amino acid sequences. 30
Phylogenetic analysis
A phylogenetic tree was constructed based on the HIV-1 env C2V3 region to elucidate the genetic variations between the mothers' and their children's viruses using Clustal W (version 1.83) with the neighbor-joining method, and its reliability was estimated by 1,000 bootstrap replications. The distance of the env C2V3 region at each time point in each subject and between mother and infant pairs was analyzed by Mega5. 31
Results
HIV-1 vertical transmission and drug resistance mutations
Of the eight HIV-1-infected children, four were positive for HIV-1 RNA at birth and the remaining four were negative at birth and became positive for HIV-1 RNA 1 (HN47 and HN60), 3 (HN88), or 6 (HN23) months after birth (Figs. 1 and 2 and Tables 1 and 2). All HIV-1 strains detected in the mothers and their infants were CRF01_AE (data not shown), although HIV-1 RNA was not amplified in the sample from one mother (HN46). In the HIV-1 strains detected in the mothers, no reverse transcriptase inhibitor (RTI) or protease inhibitor (PI) resistance mutations were found. No ARV resistance mutations were detected in the children at birth, but Y181C, a nonnucleoside reverse transcriptase inhibitor (NNRTI) resistance mutation, appeared in two (25%) children 1 (HN51) and 3 (HP25) months after birth, respectively. No NRTI or PI resistance mutations were found in these children during the follow-up period (Table 1).

Phylogenetic trees : mother's virus, X4 variant; ▲: child's virus at birth, R5 variant;  : child's virus at birth, X4 variant; ■: child's virus 1 month after birth, R5 variant; ♦: child's virus 3 months after birth, R5 variant;
: child's virus at birth, X4 variant; ■: child's virus 1 month after birth, R5 variant; ♦: child's virus 3 months after birth, R5 variant;  : child's virus 6 months after birth, R5 variant;
: child's virus 6 months after birth, R5 variant;  : child's virus 12 months after birth, X4 variant.
: child's virus 12 months after birth, X4 variant.

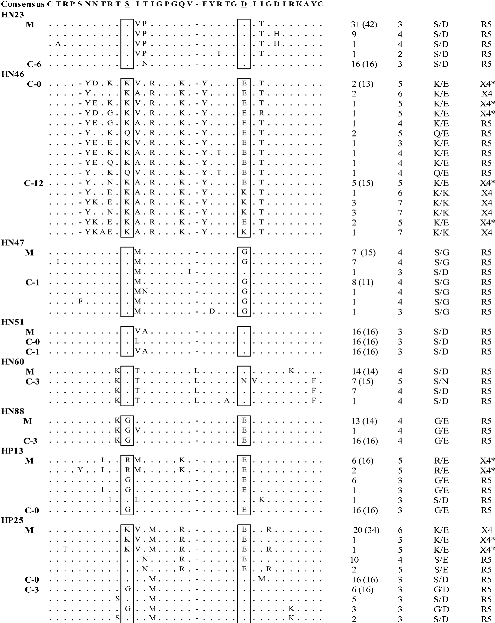
A net charge of less than and more than +5 in the V3 region indicated CCR5-using (R5) and CXCR4-using (X4) variants, respectively, and a net charge of +5 indicated R5 variants * unless accompanied by an arginine (R) or lysine (K) residue at position 11 or 25 of the V3 amino acid sequence.
Genetic diversity of HIV-1 in the mother–children pairs
Clonal sequencing of the HIV-1 env C2V3 region was performed and the genetic distance of the clones within each subject was calculated (Table 1). The mean genetic distance of the nucleotide sequences in the mothers ranged from 0.00% to 2.82% (median value: 1.09%) and from 0.06% to 2.05% (median value: 0.50%) in the children. In five pairs, the children's sequences had less diversity than their mother's sequences. In two pairs, the children's sequences had higher diversity than their mother's sequences (0.17% at birth and 0.14% 1 month after birth vs. 0.07% in HN51 and 0.52% vs. 0.00% in HN60). Thus, the children's sequences were generally more homogeneous than their mothers' sequences.
In the child HP25, the viral genetic diversity increased from 0.06% at birth to 0.89% 3 months after birth, whereas in the child HN51 it decreased slightly from 0.17% at birth to 0.14% 1 month after birth.
Predicted HIV-1 coreceptor usage
The multiple alignments of the amino acid sequences of the HIV-1 env V3 region and the predicted coreceptor usage of HIV-1 strains isolated from the eight mother-and-child pairs are shown in Table 2. Five mothers and their children (HN23, HN47, HN51, HN60, and HN88) harbored R5 viruses. Two mothers (HP13 and HP25) harbored both R5 and X4 viruses, whereas their children harbored only R5 viruses. In the remaining one mother (HN46), HIV-1 RNA could not be amplified and her child harbored both R5 and X4 viruses at birth, but only X4 virus 12 months after delivery.
Phylogenetic analysis of HIV-1 env C2V3 regions
To examine the viral genetic relationship between each mother and her child, we performed phylogenetic analyses based on the HIV-1 env C2V3 nucleotide sequences (Fig. 2). In five mother–child pairs (HN23, HN47, HN88, HP13, and HP25), the HIV-1 strains of the children formed more homogeneous clusters than the strains of the mothers (Fig. 2A, C, and F–H), whereas in the HN51 and HN60 pairs the mothers' viruses formed more homogeneous clusters than the children's viruses (Fig. 2D and E). In the HP25 child, the viral population was very homogeneous at birth, but its diversity spread significantly 3 months after birth (Fig. 2H). In the HN51 pair, the child's viruses formed two independent clusters, at birth and 1 month after birth. Interestingly, the child's virus population 1 month after birth was much closer to the mother's virus population than the child's virus population at birth (Fig. 2D). In the HP13 and HP25 pairs, the mothers' virus populations consisted of both R5 and X4 viruses, whereas their children's consisted of only R5 viruses, even though X4 viruses were dominant in their mothers (Fig. 2G and H). In the remaining pair, HN46, in which maternal HIV-1 RNA was not amplified, the child's viruses exhibited high diversity at birth as well as 12 months after birth, and the virus population at birth consisted of both R5 and X4 viruses (Fig. 2B).
Discussion
In the current study, we investigated the appearance and profile of ARV resistance mutations, the predicted coreceptor usage, and the genetic diversity of the HIV-1 strains isolated from eight pairs of HIV-1-infected mothers and their children in Northern Vietnam. All of the children were given single-dose nevirapine at birth and followed for up to 12 months. This is the first molecular epidemiological study of vertical HIV-1 infection in Vietnam.
Of the eight HIV-1-infected children, four were positive for HIV-1 RNA at birth, suggesting in utero transmission of HIV-1, and four children became positive 1, 3, and 6 months after birth, suggesting intrapartum transmission of HIV-1. All of the children were fed formula. Therefore, most of the children who failed PMTCT of HIV-1, even with single-dose nevirapine within 48 h after birth, might be infected with HIV-1 in utero and intrapartum.
The HIV-1 strains harboring a major nevirapine resistance mutation, Y181C, appeared in two (25%) of the eight children 1 and 3 months after birth. This finding is consistent with a previous study in Ethiopia that reported a prevalence of 26% for the drug resistance mutation in children who received single-dose nevirapine from 2001 to 2007, and that Y181C was the most dominant mutation in the children. 32 Other studies have reported nevirapine resistance mutations among 33–38% of HIV-infected children when both the children and their mothers were exposed to single-dose nevirapine. 33 –36
In the current study, the nevirapine resistance mutation was not detected in the children at birth, and no ARV resistance mutations were detected in their mothers, suggesting that the drug resistance mutation developed in the children independently after nevirapine administration. These findings completely agree with previous reports that most resistance mutations to nevirapine in children are selected de novo when the virus is exposed to nevirapine rather than being transmitted from their mothers. 16 Our findings together with previous results strongly suggest that longer treatment with ARV, such as 4–6 weeks of once-daily nevirapine or twice-daily zidovudine, which is recommended in the WHO ART guidelines 2013, 37 should be considered as a PMTCT of HIV-1 in the children, instead of single-dose nevirapine. It is also suggested that ARV resistance testing is necessary for the children who failed PMTCT of HIV-1 before starting antiretroviral therapy. To the best of our knowledge, this is the first report of the appearance and profile of ARV-resistant HIV-1 in children given single-dose nevirapine at birth for PMTCT in Vietnam.
In the present study, two children (HP13 and HP25) born to mothers who had both R5 and X4 viruses harbored only R5 viruses at birth, despite the X4 viruses being dominant in the mothers, demonstrating selected transmission of R5 virus from mother to child. These findings are consistent with previous studies in which the R5 phenotype was predominantly transmitted from mother to child. 38,39 In contrast, one child (HN46) harbored both R5 and X4 viruses at birth with relatively high diversity, suggesting that multiple HIV-1 strain transmission occurred in utero and evolved to some extent by delivery. However, whether HIV infection was initiated with both R5 and X4 viruses or only R5 virus(es) that evolved in utero to produce X4 virus populations in this child cannot be determined because no data were available on the mother's virus and X4 and R5/X4 viruses can be transmitted from mother to child before, during, or shortly after delivery. 40
In the current study, we found that the viral populations of the children were more homogeneous than those of their mothers at delivery, suggesting “bottleneck transmission” of HIV-1 variants from mother to child. 31 However, in the two mother–child pairs, the children's viral populations at birth and 1 month (HN51) and 3 months (HN60) after birth exhibited higher genetic diversity than their mothers' viral populations, suggesting recent infection of the mothers with HIV-1 and rapid viral replication and evolution in these children after birth. This is in agreement with a study from Sweden in which the children's viral populations were more heterogeneous than the mothers' viral populations. 31
Phylogenetic analyses showed that single-strain infection occurred in five of the eight mother–child pairs, few-strain infection in two, and multiple-strain infection in one during vertical transmission. This finding is consistent with previous studies on MTCT of HIV-1 showing that either single or multiple variants can be transmitted vertically, 42 –44 but multiple-strain infection during vertical transmission seems to be less frequent than infection initiated by a single or a few closely related maternal variants. 41 –47 Phylogenetic analyses also showed relatively longer genetic distances between the viral populations of mothers and their children in all pairs, except for HP13, which could be due to the transmission of a minor variant from the mother to her child. 48
In the current study, evolution of HIV-1 strains (HP25), viral population shifts (HN46 and HN51), and switch of coreceptor usage from R5 to X4 (HN46) were also observed in the children. However, the small number of HIV-1-infected mother–child pairs and incomplete sample collection from the children during the follow-up are acknowledged limitations in this study. Multicentric cohort studies are necessary to confirm these findings and to investigate the mechanism and risk factors associated with HIV-1 vertical transmission in Vietnam.
Sequence Data
The sequences obtained in this study were deposited in GenBank under accession numbers KP006809 to KP007125 for env and KP007126 to KP007143 for pol.
Footnotes
Acknowledgments
This study was supported by the Ministry of Education in Vietnam (the 322 scholarship program). We are grateful to all participants enrolled in this study at Hanoi and Haiphong Hospitals. We thank our colleagues: Dr. Ha, Ms. Ngoc (National Institute of Hygiene and Epidemiology, Hanoi, Vietnam), Ms. Thuy (National Hospital of Pediatrics, Hanoi, Vietnam), and the members of the Viral Infection and International Health Department of the Graduate School of Medical Science, Kanazawa University, Kanazawa, Japan.
Author Disclosure Statement
No competing financial interests exist.