
Abstract
The most common antiretroviral treatment (ART) received by individuals infected with HIV-1 in China is the combination therapy, comprised of nucleoside reverse transcriptase inhibitors (NRTIs) and nonnucleoside reverse transcriptase inhibitors (NNRTIs). To assess the prevalence of HIV-1 drug resistance and subtypes in Honghe of Yunnan, China, patient plasmas from ART-failed individuals were collected from January 2010 to December 2012. Genotyping was conducted using an in-house assay on patient plasmas. A total of 254 pol sequences were obtained. The prevalence of drug resistance was 47.2% in ART-failed individuals. Of these drug-resistant individuals, 51.7% harbored HIV strains dually resistant to NRTIs and NNRTIs or protease inhibitors (PIs) (34.2% for NNRTIs and 14.2% for NRTIs). Mutations such as M184V, A62V, T69Ins, K103N, Y181C, and G190A were common among the ART-failed individuals. The frequencies of M184V, A62V, and K103N were 20.5%, 11.0%, and 23.6%, respectively. The most common subtypes in Honghe were CRF08_BC (68.50%) and CRF07_BC (12.20%). The subtypes were almost consistent in different time points for one individual. When receiving ART for 6–12 months, the frequency of HIV-1 drug-resistant variants ranked first. This study shows that the high prevalence of HIV drug resistance observed among the ART-failed individuals should be of increasing concern (monitoring of resistance mutations) in ART regions and facilitate developing novel strategies for prevention and control of HIV infection in China.
Introduction
H
This might directly result in lower availability of drug substitution options in future ART iterations in China as there are only eight free antiretroviral drugs [including lamivudine (3TC), zidovudine (AZT), stavudine (d4T), didanosine (ddI), abacavir (ABC), tenofovir (TDF), nevirapine (NVP), efavirenz (EFV), and boosted lopinavir (LPV/r)] available from the initiation of free ART at the present time. Initially, the regimens of the first-line treatment were AZT/d4T+3TC/ddI+NVP/EFV. Because of the poor virological response and drug resistance of ddI, ddI was replaced with 3TC in 2005. In 2008, the second-line treatment became available through the national program, 5 with boosted LPV/r provided in combination with d4T, AZT, 3TC, or ddI. In 2010, TDF in combination with 3TC became available as the second-line treatment in combination with boosted LPV/r. 6 To maximize the long-term effectiveness of first-line ART and ensure the sustainability of ART programs, it is essential to minimize the further spread of HIV drug resistance.
Yunnan, a southwestern province of China that shares a border with the well-known heroin-producing region of Myanmar (Burma), was once considered the epicenter of the heroin trade and the HIV-1 epidemic in China. 7 Honghe is located in southern Yunnan bordering two provinces, one city, and six counties of Vietnam and two first-class national ports are located in this prefecture. The first HIV infection was reported in 1995; by 2012 the number of HIV-infected cases reached 18,928 in Honghe, and the frequency of HIV infections was 17.90%, which ranks first in Yunnan, including 205 foreign nationals. A recent study 8 shows that 45.1% (232/515) of the ART-failed individuals exhibited at least one drug-resistant mutation in Yunnan.
So far, a systematic drug resistance investigation was performed in Dehong and the results showed no optimistic HIV-1 drug resistance mutation. 9,10 Because of ART promotion, HIV-1 drug resistance is growing rapidly, and HIV-1-resistant mutations and genetic diversity in many areas in Yunnan are still unclear. To effectively check the spread of HIV and control the progression of AIDS in infected individuals, assessing the prevalence of HIV-1 drug resistance in regions is vital for implementing free ART in the future.
The primary aim of this study was to investigate the prevalence of HIV-1 drug resistance, with secondary aims including the examination of pol genotypes among HIV-1 ART failure individuals from 2010 to 2012 in Honghe and an evaluation of the timing of drug resistance that occurred in HIV-1 ART-failed individuals.
Materials and Methods
Study population and blood sample collection
A total of 366 individuals were included in this study between January 2010 and December 2012. Subjects were selected based on the following criteria: (1) they resided in Honghe, (2) they were aged 18 years and older, (3) when patient plasmas were collected, they were followed up since receiving ART, (4) the viral load (VL) was examined every 6 months, but some patients showed poor antiretroviral effects and the VL test would show deterioration, with the VL ≥1,000 copies/ml. Existing demographic information and clinical data as well as EDTA-3K-treated, anticoagulated whole blood samples were acquired for each subject. Samples were centrifuged at 3,000×g for 10 min and plasma was aliquoted and stored at −80°C. The VL of each study individual was determined by the Versant HIV RNA 3.0 Assay (bDNA;Siemens, IL) using the same plasma specimen used for the sequencing of RT, and was performed as recommended by the manufacturer. This study was approved by the Ethics Committee of the CPLA Kunming General Hospital and Yunnan Provincial Hospital of Infectious Disease.
RNA extraction, amplification, and sequencing of HIV-1 gene
A fragment of the HIV pol gene comprising the whole protease and 300 codons of the reverse transcriptase (RT) was bulk-sequenced from plasma HIV RNA using an in-house method developed in core laboratories that design tests for drug-resistant HIV strains in China. Viral RNA was extracted from 1 ml plasma using the Viral RNA Extraction Kit (QIAGEN, German) or the Abbott m2000s system (Canada) according to the manufacturer's instructions.
The target sequence was amplified with One Step Reverse Transcription PCR reagents procured from Takara (Dalian, China) using primers MAW26 (5′-TTGGAAATGTGGAAAGGAAGGAC-3′) and RT21 (5′-CTGTATTTCTG CTATTAAGTCTTTTGATGGG-3′) in a 25 μl reaction for 30 cycles. Cycling conditions were 50°C for 30 min, 94°C for 5 min, 94°C for 30 s, 55°C for 30 s, 72°C for 2.5 min, followed with an extension at 72°C for 10 min. The nested polymerase chain reaction (PCR) was performed using Taq PCR master mix (Tiangen, Beijing, China), using primers PRO-1 (5′-CAGAGCCAACAGCCCCACCA-3′) and RT20 (5′-CTGCCAGTTCTAGCTCTGCTTC-3′) in a 50 μl reaction for 30 cycles and the cycling conditions were 94°C for 5 min, 94°C for 30 s, 63°C for 30 s, 72°C 2.5 for min, followed with an extension at 72°C for 10 min. The resulting PCR product of 1,170 bp in length contained a full length protease (PR) gene of 99 amino acid codons and the first 254 amino acid codon segment of the RT gene. PCR products were visualized by 1% agarose gel electrophoresis. Amplified-positive samples were sequenced by Biomed Co. (Beijing, China). Each step was carried out with appropriate negative controls to detect PCR-related contamination during the experiments.
Sequence analysis
All of sequenced fragments were edited and assembled as described before.
11
Genotyping drug resistance analyses were carried out using the Stanford University's HIV Drug Resistance Database Program (
Statistical analysis
All data were analyzed using SPSS for Windows Version 19.0 (SPSS, Chicago, IL). Descriptive statistics were generated for each of the variables corresponding to specific questions in the survey. Chi-square tests were conducted to compare basic characteristics between the two groups. All statistical tests were two-sided with statistical significance defined as a value of p=0.05.
Results
Characteristics of ART-failed individuals
From 2010 to 2012, 366 ART-failed individuals were found among 6,099 ART individuals in Honghe. Two hundred and fifty-four sequences (69.4%) of the HIV-1 pol region were successfully amplified and sequenced including several repeated ART-failed individuals. Based on self-reported answers to a questionnaire, individual characteristics were obtained and are shown in Table 1 (without repeated information). The ratios of males to females in sequenced and drug resistance groups (range: 18–84 years) were 1:0.47 and 1:0.50, respectively. A total of 60.1% (139/231) were married or lived together with a spouse and the not married group was 28.6%. Heterosexual (48.5%) and intravenous drug injection (47.6%) transmission constituted the most frequent transmission routes.
VL, viral load.
To evaluate the relationship between VL and drug resistance, we divided the subjects into three groups according to VL level, and compared the difference between drug-resistant and susceptible individuals; no statistical difference was found among those groups. Among therapy regimens in ART-failed individuals, the most common regimens in Honghe were NVP/EFV+3TC+AZT, and the ART regimen frequencies were from 45.5%, 22.5% for the initial point to 35.8% and 22.5% when the blood samples were collected, respectively (Table 2).
NRTI, nucleoside reverse transcriptase inhibitor; NNRTI, nonnucleoside reverse transcriptase inhibitor; NVP, nevirapine; 3TC, lamivudine; AZT, zidovudine; d4T, stavudine; EFV, efavirenz; LPV/r, boosted lopinavir; TDF, tenofovir.
The subtype distribution in ART-failed individuals
The phylogenetic analyses based on the pol regions showed that of the 254 samples subtypes CRF08-BC (174/254, 68.50%) and CRF07-BC (31/254, 12.20%) were the most popular subtypes in Honghe. CRF01-AE (17/254, 6.69%), C (4/254, 1.57%), and B′ (2/254, 0.79%) were also identified in this prefecture. Eleven (4.33%) samples of other subtypes were found including novel B′/C and CRF01_AE/B′/C combinations. The subtypes in Honghe were similar to those found in the previous study in Yunnan. 8 In this study, 19 individuals had VL >1,000 copies/ml at more than one time point. Bootscanning and jphMM analysis were used to find the difference between the two or three pol genes in one person. Of 19 individuals, 13 had the same B′/C combination in the repeated pol gene analysis, and the jphMM results showed the position of the B′ segment appearing in subtype C with just several bases difference. One individual at two different time points exhibited a different backbone with the B′ and C subtype. The other five samples had different subtypes at different times. The C and B′/C subtypes alternated in the pol gene of four of five persons and the CRF01-AE and B′/C subtypes appeared in one person at different time points.
Prevalence of HIV drug resistance (HIVDR) in ART-failed individuals
To examine the presence of mutations in the HIV-1 pol region, the sequences were screened against the HIVDR Database from Stanford University to find known mutations related to drug resistance. The prevalence of drug resistance was 47.2% (120/254) in ART-failed individuals who exhibited at least one drug-resistant mutation. The HIVDR incidence frequencies in Honghe were 0.66%, 0.99%, and 0.92% from 2010 to 2012, respectively. Of the 120 individuals, 51.7% (62/120) were dually resistant to nucleoside reverse transcriptase inhibitors (NRTIs) and nonnucleoside reverse transcriptase inhibitors (NNRTIs) or protease inhibitors (PIs), 34.2% (41/120) to NNRTIs alone, and 14.2% (17/120) to NRTIs. The percentages of high-level resistance to 3TC, FTC, EFV, and NVP drugs were 22.4%, 22.4%, 26.4%, and 34.7%, respectively. The intermediate resistant ratios to ABC, ddI, TDF, EFV, and etravirine (ETR) drugs were 3.5%, 5.5%, 3.5%, 9.06%, and 8.66%, respectively. The low-level resistance was observed in ABC (11.8%), ddI (9.8%), and ETR (4.7%).
All the resistant scales are presented in Fig. 1. Comparing the resistance of several antiretroviral drugs between 2010 and 2012, higher resistance frequencies were found in 3TC, ddI, FTC, EFV, and NVP (Fig. 2). The rate of resistance was dramatically different between d4T and AZT in 2010. d4T has been recommended as the first-line antiretroviral therapy for treatment-naive HIV/AIDS patients in China since 2005. 15 Because of limited resources for anti-HIV infection, available antiretroviral drugs were rare in China, and the time of use of d4T was prolonged even with toxicity to individuals. 16 The mutations selected during d4T and AZT treatment were similar. Statistical differences were not found among 3 years.
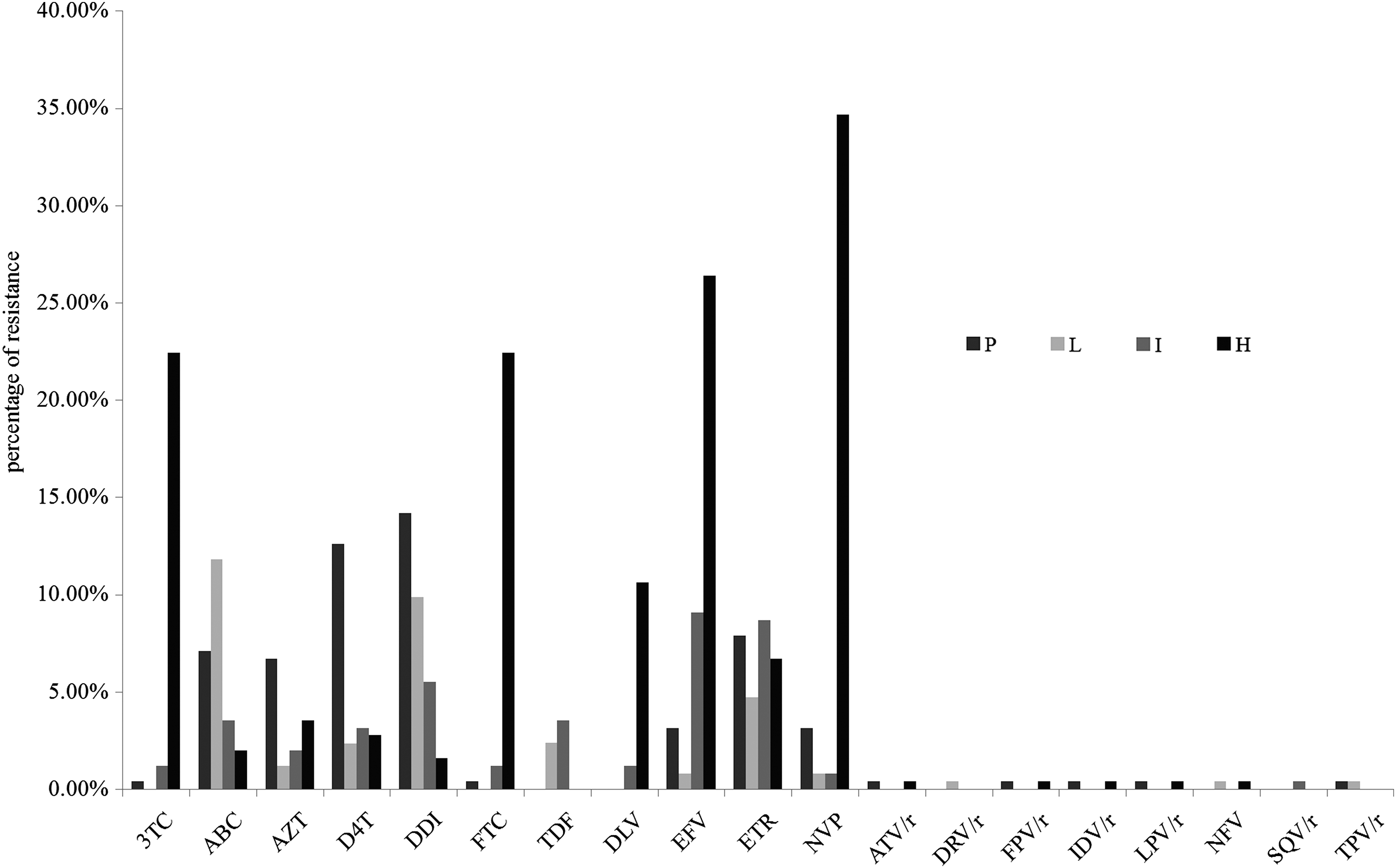
The resistant scales of antiretroviral drugs from 2010 to 2012 (P, potential low-level resistance; L, low-level resistance; I, intermediate resistance; H, high-level resistance).

The antiretroviral drug resistance comparison for 3 years (from 2010 to 2012).
The most common mutations associated with drug resistance in NRTIs were M184V (20.5%), A62V (11.0%), T69Ins (7.1%), and TAMs (thymidine analogue-associated mutations) including M41L, D67N, and K70R (Fig. 3). M184V could cause high-level resistance to 3TC and FTC and low-level resistance to ddI and ABC. TAMs were selected by AZT and d4T. TAMs-1 (M41L) could cause more serious cross-resistance than TAMs-2 (D67N and K70R). T69ins are unusual NRTI-selected mutations. According to the Stanford HIVDB, a T69 insertion alone would cause low-level resistance to all NRTIs. Together with TAMs, they confer high-level resistance to AZT, d4T, ddI, ABC, and TDF and intermediate/high-level resistance to 3TC and FTC.
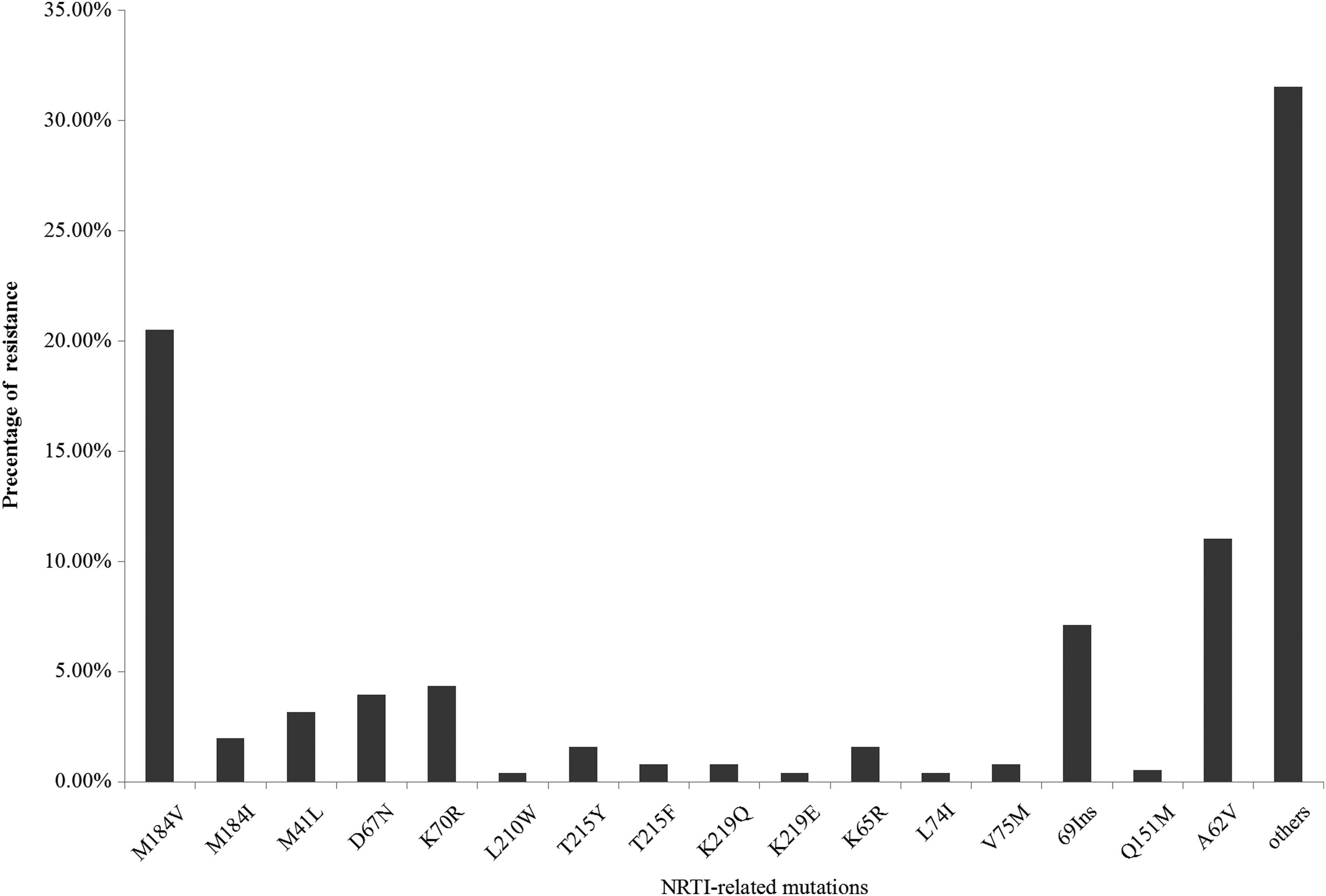
The resistant mutations associated with nucleoside reverse transcriptase inhibitors (NRTIs) in Honghe.
Along with the advancement of ART, HIV-1-resistant mutations were accumulating and multiresistant variants were increasing. Thus, those variants showed an increasing T69 mutation induced by NRTIs. K103N, Y181C, and G190A were the most prevalent mutations associated with NNRTI resistance and the frequencies were 23.6%, 7.5%, and 7.9%, respectively (Fig. 4). K103N causes high-level resistance to NVP and EFV. Y181C and G190A cause high-level resistance to NVP and intermediate resistance to EFV. Importantly, Y181C forms the foundation for intermediate ETR and rilpivirine (RPV) resistance as an addition to some single mutations and many double mutations, causing high-level resistance to these drugs. Four PI-associated mutations were observed in two individuals in this study.
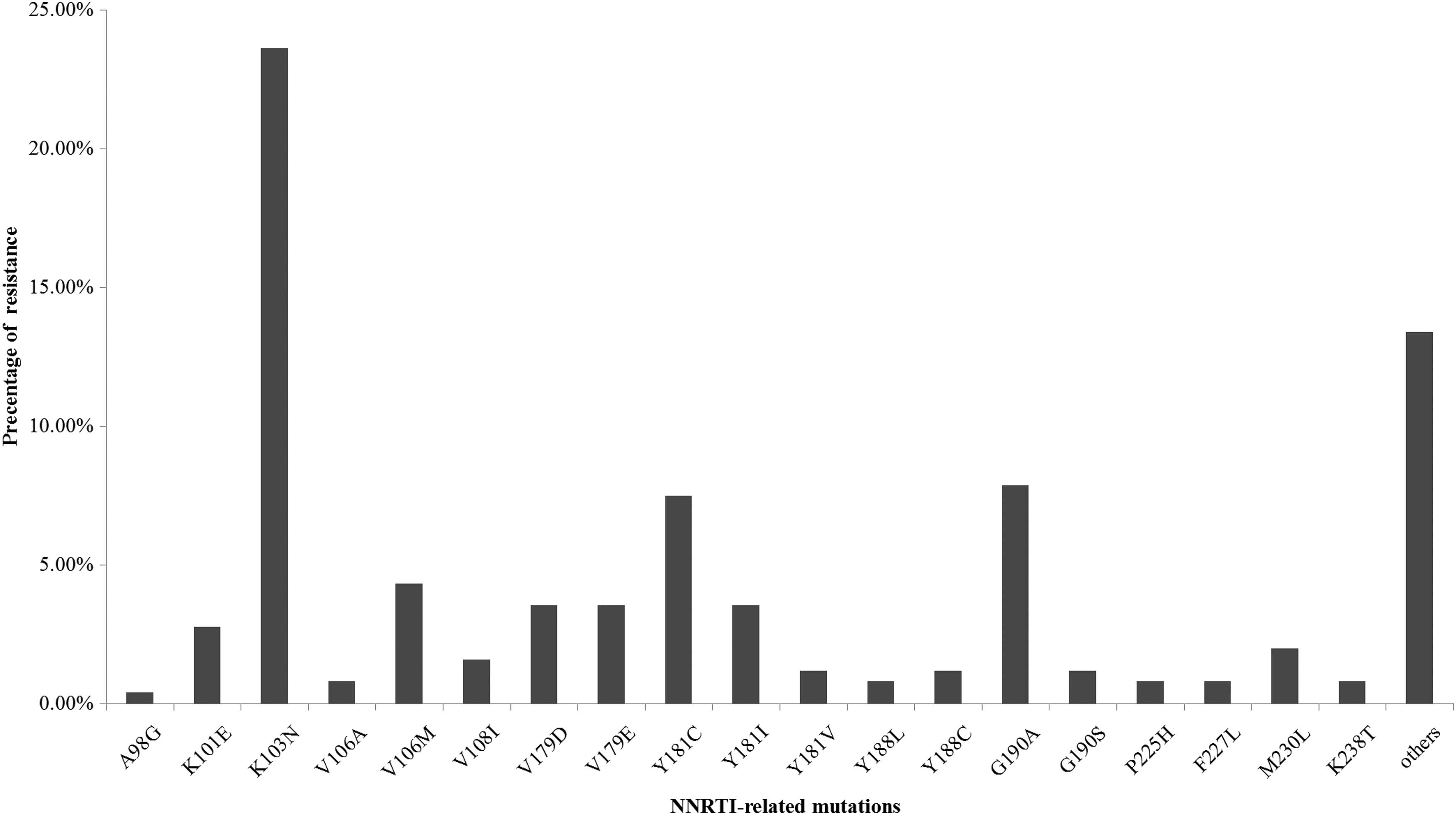
The resistant mutations associated with nonnucleoside reverse transcriptase inhibitors (NNRTIs) in Honghe prefecture.
When blood samples were first collected, all subjects were at the first event of ART failure. The duration of ART for drug resistance in ART-failed individuals was evaluated by calculating the difference in value from initiation of ART to ART failure. The best possible timing of drug resistance occurred 6 to 12 months after receiving ART, followed by 18 to 24 months (Fig. 5).
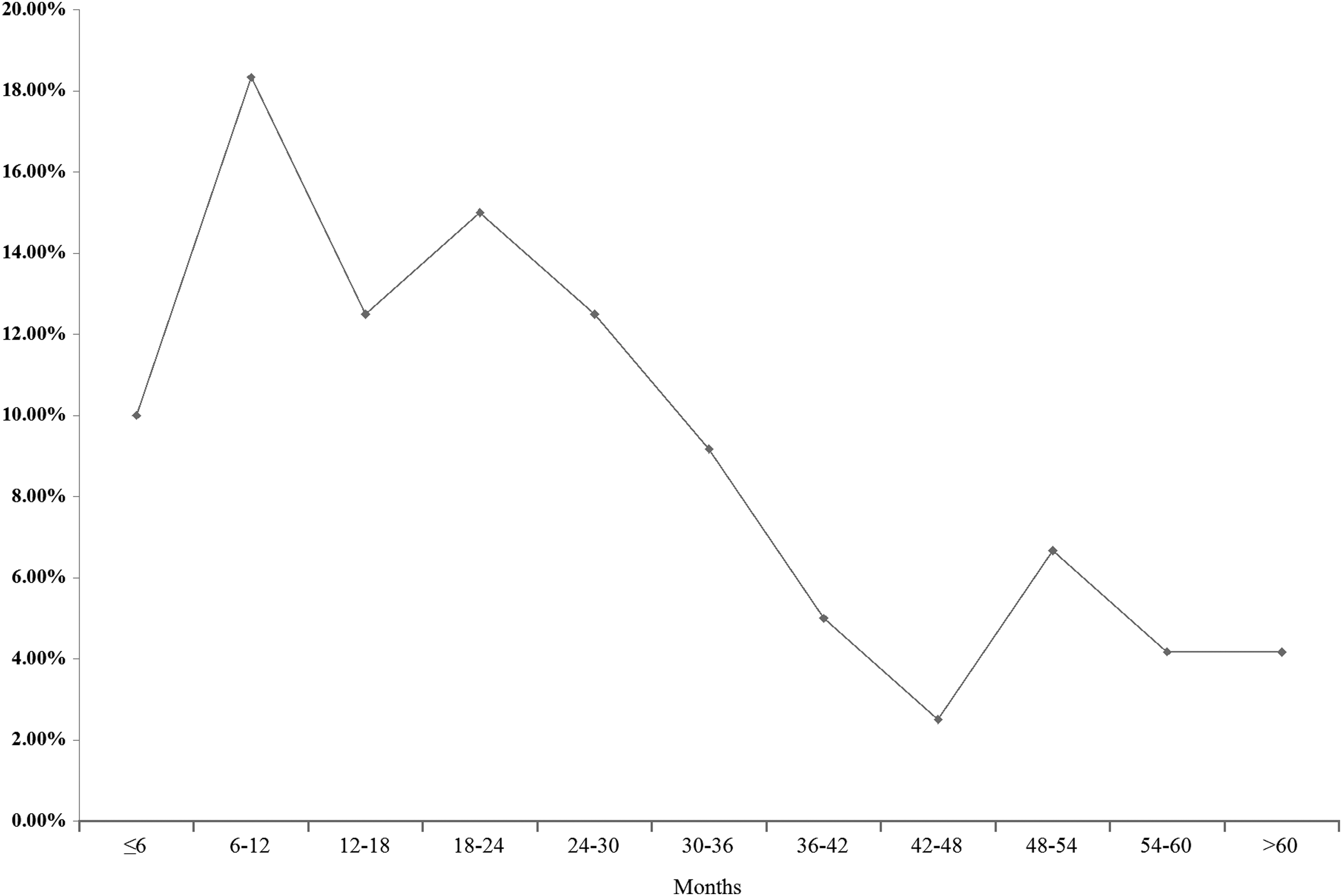
The timing (months) of drug resistance occurred among antiretroviral treatment (ART) in Honghe prefecture.
Discussion
Antiretroviral therapy has resulted in marked improvements in morbidity and mortality from HIV-1 infection. 17 –19 Adherence, drug interactions, and other associated risk factors could cause ART failure. In addition, the large variation and replication of HIV influence the effect of ART. 20,21 Because of limited therapy options and the increasing risk of treatment failure in China, the prevalence of HIV-1-resistant variants in treatment-experienced individuals has important implications for the successful management of ART, especially for the option of second-line ART.
Yunnan, the golden triangle border of the drug trade due to its complicated geographic environment, has become the region with the highest prevalence of HIV/AIDS in China, with sexual contact becoming the leading transmission route due to the influx of a large number of sex workers across the borders. 22,23 In this study, we carried out a survey of drug resistance in 254 ART-failed individuals residing in Honghe since the beginning of ART in 2004. The prevalence of drug resistance was 2.0% (120/6099) and 47.2% in ART-treated and ART-failed individuals, respectively.
The previous study conducted in 2008 showed that the DR rates of ART failure were 84% and 79% in Dehong and Kunming. 24 The research conducted in Yunnan from 2010 to 2011 revealed 45.1% HIV-1 drug resistance in ART-failed patients, which is almost consistent with our results. 8 Due to the continuous improvement of ART in Yunnan, the DR incidence was lower because of better adherence and education in ART individuals. As of 2009, a change occurred in the HIV epidemic in China as sexual contact became the leading transmission route, replacing intravenous drug injections (IDUs), aggravating the difficulty of HIV/AIDS prevention due to the migratory nature of sex workers and their multiple sexual partners. The main transmission routes in Honghe were heterosexual contact (48.5%) and IDUs (47.6%), which had no significantly statistical difference (P<0.01). The individuals resistant to NRTIs (11/6), NNRTIs (19/20), and NRTIs+NNRTIs (19/30) in the two transmissions also showed no statistical difference (P<0.01). In defective viruses, the replication capacity of HIV drug-resistant strains would be decreased during the course of viral RNA synthesis in contrast to the wild-type HIV virus, which has been proven in published papers. 25 –28
We evaluated the VL difference in NRTIs, NNRTIs, dually resistant, and susceptible groups in ART-failed individuals to demonstrate the correlation between VL and drug resistance. The results show no correlation between the VL levels and resistant incidence, similarly to a previous study. 8
CRF07_BC and CRF08_BC were first detected from IDUs in Xinjiang and Guangxi in 1997, respectively. 14,29 However, it is believed that these two CRFs were initially found in Yunnan 30 and spread through two different overland heroin trafficking routes. CRF07_BC spread northwestward to Xinjiang; and CRF08_BC eastward to Guangxi. As reported previously, these two CRFs were not identified in western Yunnan until 2002 31 –33 but were predominant in eastern Yunnan prior to 2002, including Honghe and Wenshan. 33
In this study, we have detected the pol gene subtype of ART-failed samples since 2010, including people who started ART in Honghe since 2004, and the results reveal that the prevalent subtypes in this prefecture before 2012 were similar to those in Yunnan. 8 The bootscanning and jphMM results demonstrated that in 19 people, 13 individuals exhibited the same HIV-1 variants during ART; there was one patient who showed a huge difference in subtypes at the two different time points. The different HIV-1subtypes of one person in a different period could have been caused by drug selection pressure or contact with other subtypes of HIV infection. From this result we find that if HIV-positive people follow the ART program regularly and lessen contact with other positive individual, HIV-1 variants could be controlled in the future.
An important concern for widespread use of ART is the potential emergence of HIVDR mutations given the improperly administered regimens and lack of drug adherence support in resource-limited settings. Our results here reveal that the HIVDR incidence rates in Honghe are lower than in the whole province, but higher than those in a number of countries. In Yunnan the total drug resistance rate was 3.7% and the incidence of HIVDR increased year on year from 0.9% person-year in 2008 to 2.0% in 2012. 34
An ecological study among ART-treated patients in British Columbia, Canada reported that the incidence of HIVDR diminished dramatically from 1.73 per 100 person-months of therapy in 1997 to 0.13 per 100 person-months of therapy in 2008. 35 Among those with mutations, the actual resistance mutations identified are not surprising for a developing country treatment program based on NRTIs and NNRTIs, with second-line PIs regimens not yet scaled up. Of concern, among 120 treatment-experienced patients with drug resistance mutations, 50.0% harbored resistance to both NRTIs and NNRTIs. Other studies from low- and middle-income countries have found a similar pattern. 36,37 M184I and K103N were the most prevalent NRTI- and NNRTI-related mutations in our study. M184I confers resistance to 3TC, which is also often the first mutation to develop in patients receiving partially suppressive triple combination therapy including 3TC.
K103N is one of the most clinically important NNRTI-relative resistant mutations, causing a 20- to 50-fold resistance to most available NNRTIs, with its high frequency not surprising given the prevalent use of nevirapine in China. So far, LPV/r is the only PI and the last defense against HIV infection in China. Fortunately, each patient with resistance to PIs had a single PI-related mutation, and none of the patients was resistant to LPV/r, which is an important component of the second-line regimens. The first-line ART regimens consist of two NRTIs and one NNRTI. The most common ART regimens in our study involved 3TC and NVP/EFV, because most HIV/AIDS patients enrolled in free ART programs started in 2005, and since 2005 3TC has been phased out by ddI. The frequency of NVP use was higher than EFV until 2012 in Honghe.
Resources are limited in China and the only available NNRTIs are NVP and EFV. NVP was the first free NNRTI used in HIV-infected individuals and was generically produced in China, whereas EFV was a brand drug that became available in 2005. 14 Although the PIs have been provided by SFDA as free antiretroviral drugs in China since 2008, it was used only when first-line ART failed or resistance emerged.
Taken together, this study is the first to reveal the prevalence of HIV drug resistance, genetic diversity, and timing of drug resistance that occurred in ART-failed individuals in Honghe, Yunnan, China. From a public health standpoint, it is critical to improve efforts to monitor the emergence of such mutations, to initiate a innovate ART and to monitor drug-naıve individuals to prevent the spread of resistant variants. Developing strategies to effectively optimize these ART regimens and to reduce the risk factors associated with HIV drug resistance will be a highly arduous task, but will be of momentous significance in improving HIV/AIDS prevention and control.
Footnotes
Acknowledgments
The authors wish to express their appreciation to the hospital staff members in Honghe for communicating with patients and collecting samples in performing this study. This work was supported by a grant from the National Natural Science Foundation of China (NSFC) to Zhongqi Bian (81371813). This study was also supported by the projects of the National Science Research for the 12th Five-Year Plan (2012ZX10001006 and 2012ZX10001-002). The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author Disclosure Statement
No competing financial interests exist.