
Abstract
Combined antiretroviral treatment (cART) modifications are often required due to treatment failure or side effects. We investigate cART regimens' durability, frequency of treatment-limiting adverse events, and potential risk factors and temporal trends. Data were derived from the Athens Multicenter AIDS Cohort Study (AMACS). Statistical analyses were based on survival techniques, allowing for multiple contributions per individual. Overall, 2,756 individuals, aged >15 years, initiated cART. cART regimens were grouped by their initiation date into four calendar periods (1995–1998, 1999–2002, 2003–2006, and 2007+). Median [95% confidence interval (CI)] time to first treatment modification was 2.11 (1.95–2.33) years; cumulative probabilities at 1 year were 31.6%, 29.0%, 33.1%, and 29.6% for the four periods, respectively. cART modifications were less frequent in more recent years (adjusted HR=0.96 per year; p<0.001). Longer treatment duration was associated with lower HIV-RNA, higher CD4 counts, and being previously ART naive. cART modifications due to treatment failure became less frequent in recent years (adjusted HR=0.91 per year; p<0.001). Estimated (95% CI) 1 year cumulative probabilities of treatment-limiting side effects were 16.4% (12.0–21.3%), 19.3% (15.6–23.3%), 24.9% (20.3–29.7%), and 21.1% (13.4–29.9%) for the four periods, respectively, with no significant temporal trends. Risk of side effects was lower in nonnucleoside reverse transcriptase inhibitor (NNRTI)-based regimens or triple nucleoside reverse transcriptase inhibitor (NRTI)-based cART regimens. Treatment modifications have become less frequent in more recent years. This could be partly attributed to the lower risk for side effects of NNRTI-based cART regimens and mainly to the improved efficacy of newer drugs. However, the rate of drugs substitutions due to adverse events remains substantially high.
Introduction
C
Despite the improvements in modern antiretroviral drugs in terms of both virological potency and tolerability, and the availability of drugs that facilitate the simplification of cART regimens, 10 a large proportion of HIV individuals modify or even interrupt their treatment. Several studies have investigated treatment modifications and have reported that up to 50% of HIV-infected individuals had to switch one or more drugs of their first line cART regimen. 11 –21 It is also noteworthy that reported rates of cART modifications or interruptions are higher in observational settings compared to those seen in clinical trials, with the former being more likely to reflect what actually happens in routine clinical care. 22
The most prevalent reasons for such modifications are side effects and treatment failure. Other reported reasons include the availability of newer drugs, drug–drug interactions, comorbidities, socioeconomic barriers, or patient's decision. A series of successive studies 18 –20 showed that treatment modification rates remain high with drug toxicity being the most frequent reason for such modifications. It is important to notice that when treatment fails, the clinical options are partly limited by the existence of cross-resistance among drugs of the same class. 23 Furthermore, similar limitations hold in cases of toxicity since various types of side effects are shared among several antiretroviral drugs. 24 However, it should be mentioned that during the past few years, new antiretroviral agents based on integrase inhibitors have been introduced and in addition to their antiviral potency they seem to be well tolerated. 25
As lifelong cART administration requires efficient and tolerable regimens, it is important to study their durability and the reasons leading to their modifications. In this study, we are using data from a large collaboration of HIV clinics in order to quantify the overall and reason specific rates of cART modifications. We are investigating factors potentially associated with the risk of treatment modifications without restricting our analyses to the first cART regimen only, but using data from all cART regimens per individual instead. Our focus is on temporal trends, investigating also the role of other demographic and clinical factors.
Materials and Methods
Data were derived from the Athens Multicenter AIDS Cohort Study (AMACS). AMACS is an open, ongoing, population-based cohort study of HIV+ individuals, initiated in 1996. Collaborative sites include the 10 largest HIV-1 clinics located in Athens, Greece. The study protocol was reviewed and approved by the National Organization for Medicines, by the Athens University Medical School Ethics committee, and by the corresponding hospital's scientific committee of each participating clinic. For this analysis we evaluated data collected up to July 2011 (the date at which fully recorded and quality-assured data were available). Eligible were all subjects who initiated cART while aged >15 years.
cART was defined as any regimen containing at least three drugs from at least two different classes or three nucleoside reverse transcriptase inhibitors (NRTIs) with one of them being abacavir or tenofovir. Regimens were categorized into (1) protease inhibitor (PI) based, (2) boosted PI based, (3) nonnucleoside reverse transcriptase inhibitor (NNRTI) based, (4) triple NRTI based (when one of the three NRTIs was abacavir or tenofovir), and (5) other (mainly enfuvirtide- or raltegravir-containing regimens). cART regimens were also categorized according to the date of their initiation into four calendar periods: 1995–1998, 1999–2002, 2003–2006, and 2007+ corresponding to the early cART era, the introduction of the NNRTIs, the wide use of the boosted PIs, and the modern cART era, respectively. Indinavir, invirase, nelfinavir, and ritonavir (used as a single PI in a cART regimen) are referred to as “older PIs” and the remaining PIs are referred to as “modern PIs.” Introduction of specific antiretroviral agents into AMACS collaborating clinics was in general consistent with their availability in most European Union countries.
Reasons for modifying or interrupting a cART regimen were grouped into three classes: (1) side effects (e.g., toxicities, abnormal fat redistribution, hypersensitivity reaction, and dyslipidemia), (2) treatment failure (virological and/or immunological), and (3) other (physician's or patient's decision not related to side effects or treatment failure or structured treatment interruption). If multiple reasons were reported for a specific treatment modification, the classification was based on the first (and most important) one; thus each modification was grouped to only one of the three aforementioned classes.
Statistical analysis
Data on time-to-cART modification were analyzed through survival analysis techniques. To analyze data from multiple cART regimens per individual and evaluate potential risk factors, we used modified Cox proportional hazards models according to a variation of the conditional risk set model. 26 The method is characterized by the assumption that a subject is not at risk for a second event until the occurrence of the first one and so on. In the specific application we used the variation in which time to each event is measured from the previous event.
When the event of interest was treatment modification due to side effects, modifications due to other reasons were not considered as censoring events, as individuals were still at-risk for the event of interest. In such cases, regimen-specific characteristics (type of cART regimen, baseline CD4 count/HIV-RNA viral load, age of individual at cART initiation) were treated as time updated covariates. A similar approach was used when the event of interest was a treatment modification due to treatment failure.
Cumulative incidence estimates and corresponding graphs were based only on the first cART regimen per individual. In this case, specific causes of treatment modifications were analyzed through a competing risks methodology. 27 Death rates were very low compared to rates of treatment modifications, thus death was not considered as a competing risk in any of the analyses.
In all cases, unknown reasons for treatment modifications were filled in using the multiple-imputations (MI) method. 28 The imputation model was based on multinomial logistic regression with bootstrap standard errors (1,000 replications) whereas calendar period, type of each cART regimen, prior ART exposure, sex, mode of infection, CD4 cell count/HIV-RNA viral load at each regimen's initiation, and regimens' duration were included as prognostic covariates. Thirty pseudocomplete datasets were created and combined according to standard MI methods. Statistical significance in all multivariable models was assessed through Wald tests.
Results
The AMACS database included 3,408 HIV-infected individuals. Among them, 2,764 (81.1%) received at least one cART regimen. Eight individuals were excluded from the analyses as they were <15 years old at cART initiation. The demographic and clinical characteristics of the remaining 2,756 individuals are presented in Table 1a. The majority of the study participants were male (82.3%), infected through homosexual contact (50.0%) with median (IQR) age at cART initiation 36.5 (30.6, 44.4) years. Median (IQR) follow-up after cART initiation was 5.5 (2.2, 9.6) years. Differences in these characteristics by calendar period were minor with the exception of the clear reduction over time in the proportion of individuals infected through transfusions. There are also, as expected, significant differences in the type of cART used over time (Table 1b) with unboosted PI regimens being replaced by boosted PI or NNRTI-based ones in more recent periods. During the study period, 279 (10.1%) individuals were lost to follow-up after a median time of 3.1 years and 207 (7.5%) died.
Based on chi-square tests for categorical variables and Kruskal–Wallis tests for continuous variables.
Not available: the corresponding information was missing from the patient's record.
All numbers are N (%) or median (IQR). Data are derived from the AMACS, an observational cohort study.
ART, antiretroviral treatment; HBV, hepatitis B virus; HCV, hepatitis C virus; cART, combined ART; PI, protease inhibitor; NNRTI, nonnucleoside reverse transcriptase inhibitor.
Time to treatment modification (all reasons)
The overall median (95% CI) time to the first cART regimen's modification was 2.11 (1.95–2.33) years. The corresponding figures were 1.69 (1.51, 1.86), 2.42 (2.08, 2.87), 2.33 (1.85, 2.92), and 3.64 (3.04, >4.70) for individuals who received their first cART regimen during 1995–98, 1999–2002, 2003–2006, and 2007+, respectively (log rank p-value<0.001). The estimated (95% CI) cumulative probabilities 1 year after cART initiation were 31.6% (28.2, 35.2), 29.0% (25.8, 32.5), 33.1% (29.5, 37.1), and 29.6% (26.0, 33.5) for individuals initiating cART in the four successive calendar periods, respectively. The corresponding cumulative incidence failure curves presented in Fig. 1a suggest that a substantial proportion of individuals modified their initial cART regimen within the first year, irrespectively of the calendar period of its initiation, whereas the risk of treatment modification after the first year of cART administration seems substantially lower in more recent periods.
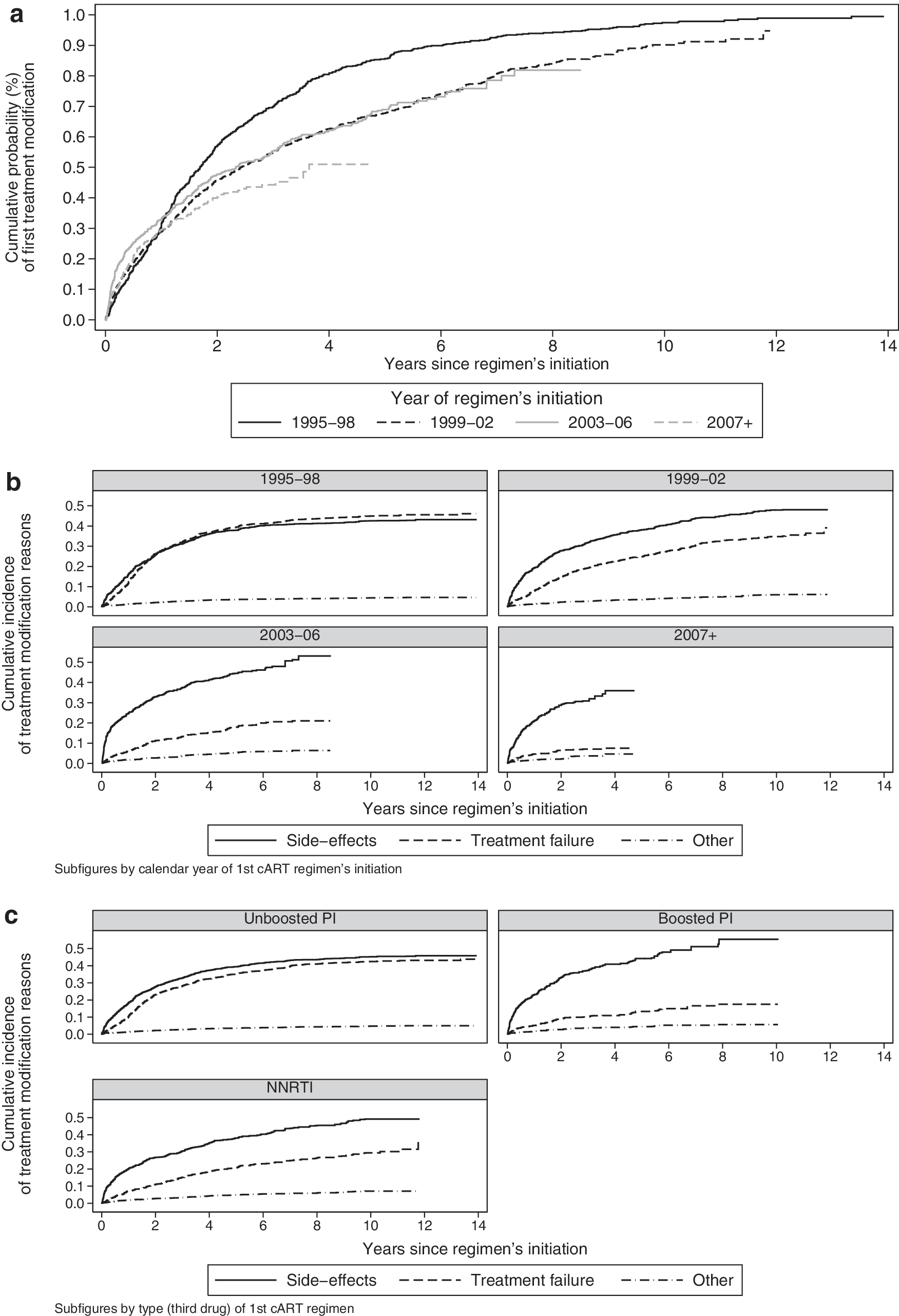
Cumulative incidence of first combined antiretroviral treatment (cART) regimen's modification
Multivariable analysis of all cART regimens per individual [median (IQR) number of regimens: 4 (2–5)] revealed a progressive decrease in the hazard of treatment modifications in more recent calendar periods even after adjustment for the type of cART and other confounders (Table 2). Results presented in Table 2 correspond to a 4% (95% CI: 3–5) reduction in the adjusted hazard of treatment modification per calendar year. Compared to unboosted PIs, all other types of cART were associated with a reduced risk of treatment modifications. The same holds for starting cART while previously treatment naive, being a non-IDU, and having higher CD4 cell count and lower HIV-RNA viral load at each regimen's initiation.
Adjusted hazard ratio (aHR).
Baseline category.
Not available.
Results are from the analysis of multiple cART regimens per individual through a multivariable (adjusted) modified Cox model. Results from separate (unadjusted) models are also shown. Data are derived from the AMACS, an observational cohort study.
The hazard of treatment modifications differed significantly according to the NRTI backbone and the “third” (cornerstone) drug used in each cART regimen (Table 3a).
Adjusted hazard ratio (additional adjustments for prior ART history, risk group, baseline CD4 cell count, and HIV-RNA viral load).
Adjusted hazard ratio.
Baseline category.
Results are from the analysis of multiple cART regimens per individual through a multivariable modified Cox model. Data are derived from the AMACS, an observational cohort study.
The emtricitabine/tenofovir backbone was associated with the lowest risk of treatment modification, closely followed by lamivudine/abacavir, lamivudine/didanosine, and lamivudine/zidovudine. Lopinavir/ritonavir was the “third drug” associated with the longer periods without modifications but boosted atazanavir, fosamprenavir or darunavir, and nevirapine or raltegravir performed equally well. In general, regimens based on older unboosted PIs had the highest risk for treatment modifications followed by older boosted PIs (aHR=0.83; p=0.017), triple NRTIs (aHR=0.72; p=0.001), NNRTIs (aHR=0.70; p<0.001), modern boosted PIs (aHR=0.60; p<0.001), and modern unboosted PIs (HR=0.55; p<0.001).
Time to treatment modification due to side effects or treatment failure
Cumulative incidence of treatment modifications due to side effects, treatment failure, and other reasons, by time since the initiation of the first cART regimen, is shown in Fig. 1b (by calendar period of cART initiation) and Fig. 1c (by type of first cART regimen). As shown in these figures, the risk of side effect-related treatment modifications remained relatively constant, whereas the probability of treatment failure clearly declined over time. Rates of modifications due to treatment failure seem lower in boosted PI and NNRTI-based regimens compared to those based on unboosted PIs.
The mean (95% CI) estimated cumulative incidence of side effect-related treatment modifications, 1 year after the initiation of the first cART regimen, was 16.4% (12, 21.3), 19.3% (15.6, 23.3), 24.9% (20.3, 29.7), and 21.1% (13.4, 29.9) for individuals who received their first cART regimen during 1995–1998, 1999–2002, 2003–2006, and 2007+, respectively, with the corresponding figures for modifications due to treatment failure being 12.3% (8.3, 17), 7.8% (5.2, 11.1), 6% (3.5, 9.3), and 4.6% (2.2, 8.4).
The only significant predictor, in a multivariable analysis of all cART regimens per individual, was the type of cART, with NNRTI and triple NRTI-based regimens being associated with a lower risk of side effects compared to PI-based ones, while time trends were not significant after adjusting for the type of cART (Table 4a). In an unadjusted model though and assuming a linear calendar time effect we estimated an indicative decrease of 2% (95% CI: 0–4%; p=0.081) reduction in hazard of treatment modification due to side effects per calendar year.
Adjusted hazard ratio.
Baseline category.
Not available.
Results are from the analysis of multiple cART regimens per individual through a multivariable modified Cox model. Data are derived from the AMACS, an observational cohort study.
Emtricitabine/tenofovir used as an NRTI backbone was associated with the lowest risk of side effects compared to all other combinations, but differences with lamivudine/abacavir, lamivudine/zidovudine, lamivudine/didanosine, and abacavir/didanosine were not statistically significant (Table 3b). Most “third drugs” had a similar risk for treatment modifications due to side effects compared to lopinavir/ritonavir. Notable exceptions were the low risk of abacavir or tenofovir (as third drugs in a triple NRTI regimen) and nevirapine and the high risk of boosted invirase (Table 3b). In general, triple NRTI or NNRTI-based regimens had a lower risk of side effects compared to old unboosted PIs (aHR=0.54; p=0.006 and aHR=0.73; p=0.001, respectively) followed by modern unboosted or boosted PIs (aHR=0.73; p=0.073 and aHR=0.83; p=0.022, respectively).
Regarding modifications due to treatment failure, there was a clear trend for a declining risk over time even after adjustment for all other confounders (Table 4b). Based on results from the multivariate analysis of all cART regimens per individual presented in Table 4b, this corresponds to a 9% (95% CI: 6–12) reduction in the adjusted hazard of treatment failure per year. Boosted PI regimens, lack of exposure to antiretroviral pre-cART, high baseline CD4 cell counts (i.e., >500 cells/μl), and low baseline HIV-RNA viral loads (i.e., <500 copies/ml) were all independently associated with a reduced risk of treatment failure.
All backbone NRTI combinations were associated with a significantly higher risk of treatment failure compared to emtricitabine/tenofovir. The highest risks were estimated for stavudine/didanosine, zidovudine/didanosine, abacavir/didanosine, and lamivudine/stavudine (Table 3c). Invirase, nelfinavir, indinavir, abacavir, or tenofovir (as third drugs in a triple NRTI regimen) and ritonavir, indinavir/r, nevirapine, and efavirenz were associated with an increased hazard of treatment failure compared to lopinavir/ritonavir (Table 3c). As expected, regimens based on older and unboosted PIs had the highest risk for modifications due to treatment failure followed by triple NRTI (aHR=0.78; p=0.327), NNRTI (aHR=0.64; p<0.001), older boosted PIs (0.56; p=0.001), modern unboosted PIs (aHR=0.44; p=0.005), and modern boosted PI-based regimens (aHR=0.38; p<0.001).
Discussion
We analyzed data on the durability and modification reasons of cART regimens. Results showed that almost one-third of the HIV-infected individuals modify their initial cART regimen within the first year of treatment, which is close to the estimates of a relatively recent and large study within the ART-CC collaboration. 29 Rates of treatment modifications due to virological and/or immunological failure showed a clear decline over the years, a finding supported by other cohort studies, 18,21,30,31 whereas those related to adverse events remained practically constant.
Ledergerber et al., 20 Vo et al., 18 and Elzi et al. 19 analyzed data from the Swiss HIV cohort study and found no change in the rates of modifications in the first line cART regimen over the years. Their estimated rates of adverse event-related cART modifications were close to the estimates of our study, but the overall rate of modifications was even higher, being approximately 40% in the first year compared to 30% in our study. The corresponding overall estimates reported by Cicconi et al. 21 and d'Arminio Monforte et al. 11 from the Italian I.CO.NA study were closer to our estimate, being 36% and 33% in their 2010 and 2000 publications, respectively. Their estimates regarding adverse event-related cART modifications were also very close to those found in our study. An older U.S.-based study 14 reported even higher overall modifications rates but similar rates of due to intolerability. Lodwick et al. 17 reported a rate of 15.4 cART modifications due to toxicities per 100 person-years among individuals with viral suppression.
In general, most studies agree that despite the continued improvement in the efficacy of antiretroviral agents, the rate of modifications in the first line cART regimens remains substantial, with the predominant reason accounting for this being toxicity or intolerance. 16
In contrast with other studies though, our study is not limited to the analysis of only the first line regimen, but considers the whole series of successive regimens per individual; thus characterization of temporal trends and risk factors reflects the complete treatment experience of HIV-infected individuals on cART. Our results suggest a slow but steady increase in cART regimens' durability over time caused mainly by the clear and steady decline in the frequency of treatment failure. It is noteworthy that these results were independent of the cART class, probably reflecting advances in the potency of newer drugs even within the same class of antiretrovirals. On the other hand, other cohort studies have shown shorter times to treatment switching in recent years, which were attributed to the expanding availability in the number of new drugs. 21,32
The well-known superiority, in terms of efficacy, of the NNRTI and boosted PI regimens compared to those based on unboosted PIs was also confirmed in our study, as we found that the risk of both, all cause and failure-related cART modifications, was lower in NNRTI and boosted PI-based regimens compared to unboosted PIs. On the contrary, we did not find any significant difference by type of cART in the risk of cART modifications due to side effects. The slight and not significant, in the multivariate analysis, decrease of 2% per year (p=0.08) in the risk of treatment modifications due to adverse events could reflect the more tolerable newly available regimens.
Preexposure to antiretrovirals, intravenous drug use, and worse immunological–virological status at each regimen's initiation were independently associated with an increased likelihood of cART modifications. These observations are consistent with the findings of previous studies. 18,31 On the contrary, concerning baseline CD4 cell counts, some investigators observed the opposite finding and suggested that patients with less urgent indication for cART have a lower motivation to continue the cART regimen. 19,29 Stability of cART was also affected by the choice of NRTI backbone and cornerstone drug, with modern antiretrovirals leading to longer lasting cART regimens, mainly through improvements in terms of efficacy rather than tolerability. Similar to findings based on the Swiss HIV cohort study 18 and the ART-CC collaboration, 29 emtricitabine/tenofovir was associated with a significantly lower risk of treatment changes compared to other NRTIs combinations.
NNRTI-based regimens had a more favorable side effect profile when compared with PIs, a finding being reported in other studies as well. 19 However, resistance and subsequently virological failure occur faster on NNRTIs than on PIs, which is probably due to the low genetic resistance barrier of NNRTIs. 33 It is also interesting that the risk of treatment modifications due to side effects in raltegravir-based regimens was the lowest one among all other “third drugs.” Unfortunately though, the proportion of regimens based on integrase inhibitors in our study was very low, thus their favorable tolerability profile 25 could not be clearly supported by the data (for example, the corresponding difference between raltegravir and boosted lopinavir did not reach formal statistical significance levels).
These results cannot be directly compared to those reported by other studies since most of them focus on modifications of the first line cART regimen or those observed within the first year of treatment. Moreover, the analysis of temporal trends in cART stability and the corresponding comparisons between different studies are often confounded by differences in the inclusion criteria, calendar period of investigation, physicians' policy, methods of statistical analysis, etc. Clinical trials tend to report lower rates of treatment modifications but they usually exclude patients with severe comorbidities. Other studies focus on relatively short calendar periods and thus have limited power to detect temporal trends. In the past few years, ease of access to new antiretrovirals and national health system policies may also have influenced the frequency of drugs substitutions. Finally, there may be physicians who would substitute a drug in a successful regimen due just to concerns regarding potential long-term toxicity.
In general, there are two mechanisms with a common source but opposite effects on the overall rate of treatment modifications: newer antiretrovirals are more efficient, thus treatment failure occurs more rarely, but on the other hand their availability may lead some physicians to modify a successful and tolerable regimen for other reasons (e.g., regimen simplification and pill burden reduction). Moreover, the mere availability of alternate agents may have also changed how side effects are viewed: mild ones may be tolerated when there are few therapeutic options but not when there are multiple other choices. This change may partly explain the stable and relative high rate of side effect-related drug substitutions.
To interpret and generalize our results, it is necessary to take into account some specific issues related to the analysis method and the nature of our data. For example, our estimates of first line treatment modifications probabilities, due to specific failure or side effects, have been derived using the competing risks methodology, thus they should not be interpreted independently of each other. Results concerning specific antiretroviral agents should in general be cautiously interpreted, due to potential confounding effects driven by other associations with other drugs frequently used in the same regimens (e.g., newer NRTI backbones became available at the same time as newer, more potent, better tolerated, boosted PIs did). However, in our multivariable models, both backbone and “third drug” effects are simultaneously considered, thus adjusted for each other. The substantial proportion of cases in which the reason for a treatment modification was not available, especially in the early cART years, was a drawback of our study. However, we addressed this issue through multiple imputation methods; thus the increased uncertainty due to missing data is appropriately reflected in our results. Finally, although we adjusted our models for all available confounders, AMACS is an observational study, thus residual confounding cannot be ruled out.
In conclusion, in our cohort, the reduction in the risk of modifications due to virological failure over the years was substantial. However, our findings suggest that toxicity remains an issue and highlight the need for the application of even more tolerable regimens. An approximately constant rate of modifications due to intolerance or toxicity and a very low rate of modification for other reasons led to a significant but less impressive improvement in cART stability. Optimizing initial cART and individualizing treatment thereafter, in terms of tolerability and efficacy, have become indispensable for the management of patients and the durability of their treatment.
Footnotes
Acknowledgments
Parts of the data were presented at the 25th Conference of the Hellenic Society for the Study and Control of AIDS (2013), Athens, Greece.
AMACS consists of the following members:
Steering Committee: Antoniadou A, Chrysos G, Daikos G, Gargalianos-Kakolyris P, Gogos HA, Katsarou O, Nikolaos V Sipsas, Lazanas M, Nikolaidis P, Panos G, Paparizos V, Paraskevis D, Sambatakou H, Skoutelis A, Touloumi G (Chair).
Coordinating Center: Department of Hygiene, Epidemiology and Medical Statistics, Athens University Medical School, Athens, Greece (Touloumi G, Pantazis N, Vourli G, Gountas I, Gioukari V).
Participating Centers: Fourth Department of Internal Medicine, Athens Medical School, Attikon University Hospital (Antoniadou A, Papadopoulos A, Petrikkos G); Infectious Disease Unit, “Tzaneio” General Hospital of Pireaus (Chrysos G, Paraskeva D, Hatziastros P); First Department of Propedeutic Medicine, Athens University, Medical School “Laikon” General Hospital (Daikos G, Psichogiou M); 1st Department of Medicine, Infectious Diseases Unit, “G. Gennimatas” Athens General Hospital (Gargalianos-Kakolyris P, Xylomenos G); First Department of Internal Medicine, Infectious Diseases Section, Patras University Hospital (Gogos HA, Marangos MN, Panos G); Haemophilia Centre, Second Blood Transfusion Centre, “Laikon” Athens General Hospital (Katsarou O, Kouramba A, Ioannidou P); Infectious Diseases Unit, Department of Pathophysiology, “Laikon” Athens General Hospital and Medical School, National and Kapodistrian University of Athens (Sipsas NV, Kontos A); Infectious Diseases Unit, Red Cross General Hospital of Athens (Lazanas M, Chini M, Tsogas N); First Department of Internal Medicine, Infectious Diseases Division, AHEPA University Hospital, Aristotle University HIV Unit (Metallidis S, Tsachouridou O, Skoura L); Second Internal Medicine Clinic, First IKA (Panos G, Haratsis G); AIDS Unit, Clinic of Venereologic and Dermatologic Diseases, Athens University, Medical School, Syngros Hospital (Paparizos V, Leuow K, Kourkounti S); HIV Unit, Second Department of Internal Medicine, Athens University, Medical School, Hippokration General Hospital (Sambatakou H, Mariolis I); Infectious Diseases and HIV Division, Department of Internal Medicine, Evaggelismos Athens General Hospital (Skoutelis A, Papastamopoulos V, Baraboutis I); Infectious Diseases Unit, University General Hospital of Alexandroupolis, Democritus University of Thrace (Panagopoulos P, Ganitis A).
Author Disclosure Statement
No competing financial interests exist.