
Abstract
Antiretroviral therapy (ART) improved the survival of people living with HIV/AIDS (PLWHA) and decreased HIV-related morbidities. This study assesses the cancer incidence of all adult PLWHA in Israel by transmission routes before and after 1996. This cohort study was based on cross-matching the National HIV/AIDS and Cancer Registries of all HIV/AIDS and cancer cases reported from 1981 to 2010 with the National civil census. PLWHA were followed-up until cancer diagnosis, death, leaving Israel, or 2010, whichever occurred first. Cancer incidence was adjusted for age, and compared with the National incidence. Of all 5,154 PLWHA followed-up for 36,296 person-years, 362 (7.0%) developed cancer (997.4 cases per 100,000 person-years). Higher hazard ratios to develop cancer were demonstrated among older PLWHA, Jewish people, and intravenous drug users. Cancer incidence among PLWHA was higher in the pre-ART period than after 1997 (1,232.0 and 846.7 cases per 100,000 person-years, respectively). The incidence of AIDS-defining cancers was higher than non-AIDS-defining malignancies, and higher in the pre-ART than the post-ART period (777.0 and 467.2 cases per 100,000 person-years, respectively), while the incidence of non-AIDS-defining cancers showed the opposite trend (376.5 and 455.0 cases per 100,000 person-years, respectively). The incidence of AIDS-defining and non-AIDS-defining cancers declined between the pre-ART and the post-ART period by 2.0 to 3.4 times. PLWHA had higher rates of malignancies than the general population. In conclusion, cancer incidence among PLWHA was associated with age, and declined after ART introduction; yet it was higher than that of the general population. PLWHA may benefit from age-related cancer screening, increased adherence to ART, and reduction of environmental oncogenes.
Introduction
P
Antiretroviral treatment (ART) was introduced in Israel in 1997 and became available for all citizens in Israel. It has improved the immune function of PLWHA, reduced the risk of AIDS progression, and decreased AIDS-related mortality. 4 Despite these promising results, long-term studies have found that PLWHA remained at higher risk for developing malignancies. 5,6 Along with the longer survival of PLWHA, they are susceptible to the consequences of aging and also have prolonged exposure to cancer risk factors, such as environmental or infectious agents. 7 Therefore, data are needed to appraise the cancer incidence among PLWHA, and also to evaluate the long-term achievements of ART.
The aims of this study were to assess, for the first time in Israel, the incidence of cancers among all PLWHA (both AIDS-defining and non-AIDS-defining malignancies) before and after the introduction of ART in Israel in 1997 and by different HIV transmission routes.
Materials and Methods
This cohort study included all PLWHA adult Israeli citizens who were reported between 1981 and 2010. Individuals diagnosed with HIV or AIDS in Israel are reported by law to the Ministry of Health since 1981 and recorded in the National HIV/AIDS Registry (NHAR). The reports contain demographic (name, identification number, family status, address, ethnicity, e.g., Jewish or Arabic, date, and country of birth), behavioral, and clinical data for each notification. In response to a possible reporting bias of newly diagnosed patients who may refrain from disclosing their risk behavior immediately upon diagnosis, the NHAR is periodically updated with continuous name-based reports from all the AIDS treatment centers and the regional health departments regarding behavioral and clinical changes since the initial notification. The completeness of the NHAR is estimated at 99% of all PLWHA who were diagnosed in Israel. 8
The Israeli Cancer Registry includes all subjects identified with malignancies since 1960. This name and identification number Registry utilizes passive compulsory notification of cancers from all medical institutions in Israel, based on record linkage with patient's files and the death registry. All cancers are recorded according to the International Classification of Diseases for Oncology (ICD-O, version 3), including histological findings and stage of the tumors. 9 The completeness of this registry is estimated at 93% for solid tumors. 10
As both NHAR and the Cancer Registry are identified, cross-matching was performed in December 2011, using the names, dates of birth, and identification numbers of all PLWHA and cancer patients. These registries are also periodically cross-linked with the National Civil Census to identify those who died or left Israel. Inclusion criteria for this study involved all adults older than 15 years of age who were diagnosed with HIV/AIDS and/or cancer between 1981 and 2010. Only PLWHA who were Israeli citizens were included in this study, as they could be traced if they had died or left Israel by the end of the follow-up period. Those who were diagnosed with cancer before or during their first visit to the HIV clinic were excluded. The dates of reporting of HIV/AIDS or cancer were obtained by cross-matching the NHAR with the Cancer Registry, respectively. All PLWHA who were free of cancer were followed from their HIV/AIDS reporting date to either developing malignancy, death, leaving Israel to go to another country, or December 2010, whichever occurred earlier. In cases in which PLWHA were diagnosed with two malignancies, only the first diagnosis was recorded in our study.
AIDS-defining cancers included Kaposi's sarcoma, non-Hodgkin lymphoma, and cervical cancer, while all other malignancies were classified as non-AIDS-defining cancers. Coinfections with tuberculosis were recorded by cross-matching the NHAR with the National Tuberculosis Registry, while infectious syphilis (primary or secondary) was recorded by cross-matching with the individual reports reported to the Ministry of Health. HIV/AIDS, tuberculosis, and syphilis are reportable conditions in Israel.
Statistical analysis
The follow-up time from HIV diagnosis to developing cancer was determined by person-years (PY). Incidence density was calculated by dividing the number of PLWHA with cancer by the sum of PY of the population at risk. Trend analysis was performed by the Chi-square test to yield the linear-by-linear association test. Comparison between PLWHA who were Israeli citizens and developed cancer with PLWHA who were Israeli citizens and did not was performed by the Chi-square test for categorical variables, while continuous variables were compared by the Kruskal–Wallis test for attributes that were not distributed normally. Reference categories were designed according to findings in previous studies in order to highlight the differences between the independent variables. The results were presented by their odds ratio (OR) and 95% confidence intervals (95% CI). Independent variables included age, gender, religion, countries of birth, possible place of infection, periods of HIV reporting (before or after the introduction of ART), routes of HIV transmission, and other coinfections. If the route of HIV transmission was not known or the infection was acquired vertically, it was classified as “other.” p<0.05 was considered statistically significant and variables achieving statistical significance were included in the multivariable analyses. The multivariate analyses were performed by Cox proportional hazard models after assessing for collinearity (for example, country of birth and possible place of HIV infection) and also after testing that all covariates satisfy the assumptions of proportionality, to evaluate the association of specific independent factors with the risk of developing cancer. Results were expressed as hazard ratio and 95% CI. Adjusted Cox regression curves were used to describe time of follow-up classified by cancer type and HIV transmission routes before or after 1997.
The rate of cancer and site-specific malignancies in PLWHA before or after 1997 were described by incidence rates (IR) per 100,000 PY and also by age-adjusted standardized IR (SIR), which was calculated by dividing the observed number of cases in PLWHA in our study with that expected in the general population. The expected number of cases was estimated by weighting the age-specific and sex-specific IR for each annum for the general population using the Ministry of Health annual cancer publications.
All analyses were performed by SPSS program version 19.0. The study was approved by the Ben Gurion University Institutional Review Board.
Results
From January 1, 1981 to December 31, 2010, 5,154 PLWHA who were Israeli citizens older than 15 years of age were reported to the Ministry of Health. During the study period, which involved 36,296 PY, 362 PLWHA (7.0%) developed malignancies, demonstrating a cancer incidence density of 997.4 cancer cases per 100,000 PY. Of all PLWHA with malignancies in the pre-ART period, 140 (77.8%) died, while 85 (45.2%) PLWHA with malignancies died in the post-ART period (p<0.01).
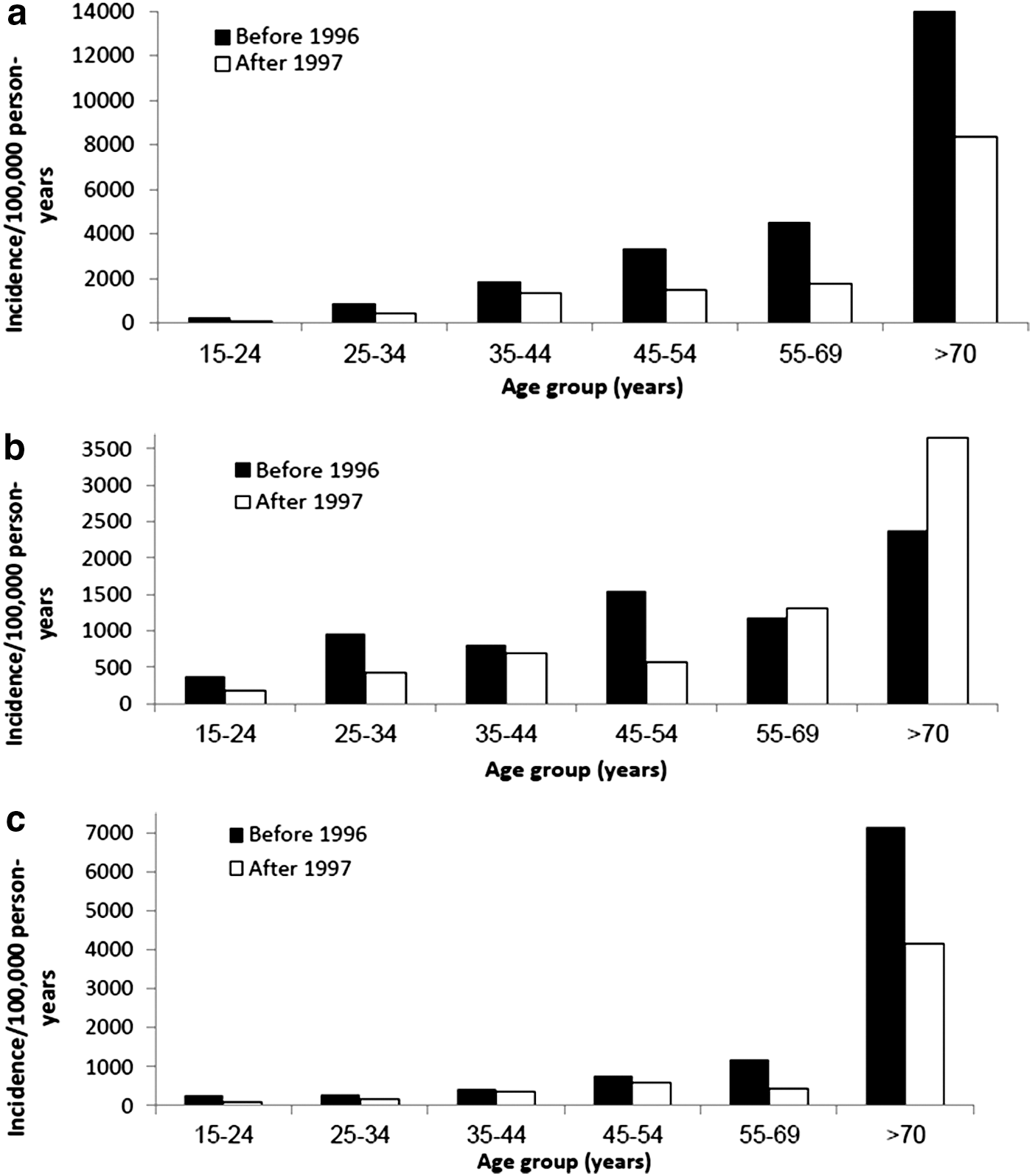
The incidence density of all malignancies among PLWHA who were diagnosed in the pre-ART period (1981–1996) was higher than in the post-ART period (1997–2010) across all age groups, demonstrating 1,232.0 and 846.7 cases per 100,000 PY, respectively, p<0.01 (Fig. 1a). PLWHA who developed any cancer were older, more likely to be Jewish and Israeli born, had HIV/AIDS reported before 1996, and were infected by homosexual contact or exposed to infected blood products (Table 1a). In multivariate analysis, older PLWHA, Israeli born, had HIV reported before 1996, and acquired the infection by homosexual contact or by exposure to infected blood products were predictive variables associated with cancer (Table 2a).
Adjusted for age and time of follow-up.
5-year interval.
SD, standard deviation; OR, odds ratio; CI, confidence interval; IVDU, intravenous drug users.
5-year interval.
CI, confidence interval; IVDU, intravenous drug users.
The incidence density of AIDS-defining malignancies was higher in the pre-ART than that the post-ART period, demonstrating 777.0 and 467.2 cases per 100,000 PY, respectively, p<0.01. The incidence was higher in the younger age groups in the pre-ART period, but higher for PLWHA older than 55 years of age in the post-ART period (Fig. 1b). PLWHA who developed AIDS-defining cancers were older, more likely to be Jewish and Israeli born, had HIV/AIDS reported before 1996, and were infected by homosexual contact or were exposed to infected blood products (Table 1b). In multivariate analysis, older PLWHA, being male, being Israeli born, had HIV reported before 1996, and acquired the infection by homosexual contact were predictive variables associated with AIDS-related cancers (Table 2b).
Adjusted for age and time of follow-up.
5-year interval.
SD, standard deviation; OR, odds ratio; CI, confidence interval; IVDU, intravenous drug users.
5-year interval.
CI, confidence interval; IVDU, intravenous drug users.
The incidence of non-AIDS-defining malignancies has increased between the pre-ART and the post-ART period from 376.5 to 455.0 per 100,000 PY, respectively, p=0.01, and was associated with age (Fig. 1c). PLWHA who developed AIDS-defining cancers were older, more likely to be Jewish and Israeli born, had HIV/AIDS reported before 1996, were infected by homosexual contact or were exposed to infected blood products, and also developed tuberculosis (Table 1c). In multivariate analysis, older PLWHA, being Israeli born, had HIV reported before 1996, were infected by exposure to infected blood products, and developed tuberculosis were predictive variables associated with non-AIDS-related cancers (Table 2c).
Adjusted for age and time of follow-up.
SD, standard deviation; OR, odds ratio; CI, confidence interval; IVDU, intravenous drug users.
Adjusted for age and time of follow-up.
CI, confidence interval.
Cox proportional regression models adjusted for age and time of follow-up showed that PLWHA who acquired the infection by homosexual transmission were at the greatest risk of developing cancers of all causes before 1996, while those who were infected by contaminated blood products were at highest risk after 1997 (Fig. 2a). PLWHA who acquired the infection by homosexual transmission were at the greatest risk of developing AIDS-defining cancers before 1996, while this group and those who were infected by contaminated blood products were at highest risk after 1997 (Fig. 2b). PLWHA who acquire the infection by infected blood products were at the greatest risk of developing cancers of all causes before 1996, while those who were infected by homosexual contact were at highest risk after 1997 (Fig. 2c).

Both the IR and SIR of all AIDS-defining cancers, including KS, NHL, and invasive cervical cancer, were higher in the pre-ART period than the post-ART period. The IR and SIR of all non-AIDS-defining cancers were also higher in the pre-ART period (Table 3). The most common non-AIDS-defining cancers were Hodgkin's lymphoma (nine cases in the pre-ART period vs. seven cases in the post-ART period, age-adjusted SIR of 165.2 and 36.9, respectively), followed by malignancies of the lung (eight vs. seven cases, age-adjusted SIR of 73.5 and 18.1, respectively), malignancies of the liver (four vs. five cases, age-adjusted SIR of 102.6 and 400.0, respectively), and anal malignancies (four vs. four cases, age-adjusted SIR of 71.3 and 18.5, respectively).
F, female; M, male IR, incidence ratio; SIR, standardized incidence ratio.
Of all homosexuals who developed malignancies, a higher rate developed AIDS-defining cancers before ART was introduced than after its marketing (N=56, 75.3% and N=22, 51.1%, respectively, p=0.01), while non-AIDS-related cancers were more prevalent in the post-ART than the pre-ART period (N=20, 27.4% and N=22, 48.9%, respectively, p=0.01). KS has shown the most substantial decrease among homosexuals between the pre-ART and the post-ART period (N=42, 56.8% and N=12, 26.7%, respectively, p<0.01). In contrast, the rate of anal carcinoma among homosexuals has increased between the two periods, although it did not achieve statistical significance (N=4, 5.4% and N=4, 8.8%, respectively, p=0.3).
Discussion
This 30-year incidence study, which included all 5,154 PLWHA reported in Israel, found that 7.0% developed cancer, while the incidence density was lower in the post-ART period for both the AIDS and the non-AIDS-defining cancers than before ART was introduced. The decreasing rates of cancer between the two periods may be related to the improving efficacy and tolerability of ART, which has increased patient's adherence. ART's protective effects may include decreased immune activation and cytokine levels, boosting immune response, increased CD4 levels, and ART-related suppression of oncogenic viruses. 11 Due to the success of ART, PLWHA are now living longer and not succumbing to death due to other causes, resulting in a greater cumulative chance of cancerous events.
The proportion of cancer among PLWHA in our study was generally similar to that reported from other countries. 12 The risk for developing malignancies remained significantly more elevated in PLWHA than in the general population. It may be that advancing age and greater cumulative exposure to environmental (such as tobacco and alcohol) or viral (HHV-8, HPV, hepatitis B, or Epstein–Barr viruses) carcinogens are associated with an increased risk of malignancies. It is therefore imperative to understand how anticancer regimens and ART interact in order to develop optimal treatment approaches.
Although all AIDS-defining cancers have decreased between the pre-ART and post-ART periods (especially KS), AIDS-related cancers still remained the most common malignancies in the PLWHA population in Israel, as was also found in the United States. 3 NHL and invasive cervical cancers also remained the most common malignancies in the post-ART period in our study. It might be that the damage done by the initial HIV infection, on-going immune reactivation, 13 suboptimal immune reconstitution, 14 and perhaps long-tern ART exposure continue to increase the risk of PLWHA for KS 15 and other AIDS-related cancers. Cervical cancer, which is also characterized by a viral etiology, has a long lag time between primary infection and clinical disease. As such, the initiating event for cancer that manifests itself clinically in the early periods of widely available ART could have taken place when the patients were exposed to less than optimal ART or when no therapy was available. 15
The number of PLWHA with invasive cervical cancer increased between the pre-ART and the post-ART period, as was also found in another study. 16 It may a result of the greater number of HIV-infected women diagnosed in the post-ART period (N=1,350 vs. N=319 in the pre-ART period in our study) and also a result of increasing awareness among women and physicians to screen for cervical cancer. 16 It is also possible that HIV-infected women are more exposed sexually to HPV than the general population or that HPV coinfection has a relatively long latency before its oncogenic effects become relevant in PLWHA. 11
The incidence of non-AIDS-defining cancers among PLWHA has decreased between the pre-ART and the post-ART period, in line with other studies 7 and contradicting results published by others. 6,11 It might be that the longer survival of PLWHA and the relative older age of the newly diagnosed PLWHA in the post-ART compared to the pre-ART period were related to the greater risk of cancer. Unlike other studies, 11 we did not find an increased incidence of anal carcinoma in the post-ART period. It is probably due to the relatively small size of the specific cancer types detected in PLWHA in Israel, as also suggested in an Italian publication, which found similar results. 7
Although PLWHA who acquire the infection by homosexual transmission were at highest risk of developing AIDS-defining cancers in both the pre-ART and the post-ART periods, the rate of malignancies among them has decreased between the two periods, especially the incidence on KS. However, the rate of non-AIDS-defining cancers has increased between the pre-ART and the post-ART period, especially the rate of anal carcinoma, in line with other studies focusing on homosexuals. 17,18 It was suggested that the relatively high adherence of ART affects carcinogens that occur at low CD4 levels, such as HHV-8. The reduction may also be related to the adaptation of safer sex practices that have reduced the transmission of HHS-8, as almost 50% of cancers are linked to environmental and lifestyle factors. 18
Our study is noteworthy, as it is the first study describing the natural history through 30 years of all PLWHA with Israeli citizenship who have free access to HIV treatment and care, in updated National databases characterized by high completeness and good quality. Yet it is subject to several limitations. First, we had no data regarding the specific ART used by each patient. However, as all PLWHA who are citizens are entitled to unrestricted clinical and laboratory follow-up and free ART, it is probable that most patients are prescribed the most updated available therapy, which supports adherence. Second, data regarding other cancerous cofactors, such as smoking, family history, and viral infection, were not available nor were laboratory data pertaining to CD4 counts. However, we believe that these cofactors remained unchanged among PLWHA, and that the bias, if it occurs, is nondifferential and conservative. Third, the SIR calculation is more subject to overdiagnosis bias in the PLWHA than that of the general population, as PLWHA are more commonly screened for malignancies. Fourth, regular screening of PLWHA led to early diagnosis and possible better survival than the general population, causing lead time bias. Fifth, survival bias may have also affected our results between the pre-ART and post-ART periods, as the life expectancy of HIV-infected individuals had increased after the introduction of the ART; thus, they live long enough to develop AIDS. We therefore analyzed the results by adjusting to age and time of follow-up.
In conclusion, both AIDS-related and non-AIDS-related cancers decreased after the introduction of ART and their diagnoses were strongly associated with age. The incidence density of AIDS-defining malignancies was higher in the pre-ART than in the post-ART period, while the incidence of non-AIDS-defining malignancies showed the opposite trend, and increased between the pre-ART and the post-ART period. Yet, cancers remain an important prognostic factor in PLWHA and the initiation of age-related cancer screening and ART early in the course of HIV infection can sustain high levels of immune function and reduce malignancies.
Footnotes
Acknowledgment
The authors wish to thank Ms. Zehuvit Wiexelbom from the department of tuberculosis and AIDS in the Ministry of Health for her exceptional maintenance of the National HIV/AIDS Registry.
Author Disclosure Statement
No competing financial interests exist.