
Abstract
There is continuous need to track genetic profiles of HIV strains circulating in different geographic settings to hasten vaccine discovery and inform public health and intervention policies. We partially sequenced the reverse transcriptase region of the HIV-1 pol gene from a total of 54 Kenyan patients aged 18–56 years who continued highly active antiretroviral treatment (HAART) for between 8 and 102 months. Subtyping was done using both the JPHMM tool and phylogenetic method. HIV-1 subtype A1 was the predominant strain in circulation, representing 57.4% and 70.4% of all isolates as determined by JPHMM and phylogenetic methods, respectively. Subtypes D (14.8%, 7.4%), C (5.6%, 9.3%), and A2 (0%, 5.6%) were determined at respective prevalence by both methods. JPHMM identified 22.2% of the isolates as recombinants. This surveillance focused on the RT gene and reaffirms the predominance of subtype A and an increasing proportion of recombinant strains in the Kenyan epidemic.
T
The Kenyan epidemic has declined significantly and steadily over the past 8 years to stabilize at low levels of 5.6%, 5,6 although there are key demographic pockets for escalating new infection. 7 The overall improvements in HIV prevalence in Kenya can be attributed to gains in uptake of testing and scaled access to HAART. 8 But increased access to HAART presents special challenges in diagnosing new infections, monitoring of the epidemic, and managing subepidemics as new or mutant virus strains appear in circulation. 9
We recently reported on HIV subtype variability in Kenyan HAART patients based on envelope sequences. 10 The epidemiologic architecture of the Kenyan epidemic displays characteristic variability at both genetic and geographic levels, with HIV-A dominating, although at a declining prevalence. 10 –13 Here, we report the genetic diversity of the HIV-1 RT gene among patients who have sustained HAART for between 8 and 102 months.
Fifty-four patients aged 18 to 56 years were enrolled between February and September 2013 from six comprehensive care centers located in Kiambu, Kajiado, Naivasha, Malindi, Kisumu, and Homa Bay counties. Five milliliters of EDTA venous blood was drawn from each patient and fractionated to obtain peripheral blood mononuclear cells (PBMCs) and plasma as described earlier. 10 RNA was extracted from plasma of patients with viral load (VL) above 1,000 RNA copies/ml using the QiaAmp Viral RNA Mini Kit while DNA was isolated from PBMCs of patients with VL up to 1,000 HIV RNA copies using the QiaAmp DNA Mini Kit and according to manufacturer's instructions. For the RNA, a 701-base pair segment of the HIV-1 pol-RT gene corresponding to nucleotides 2480–3180 of HIV-1HXB2 was amplified in a One-Step reverse transcriptase polymerase chain reaction (RT-PCR) protocol (Qiagen) followed by a nested PCR. Primers RT18 (5′-GGAAACCAAAAATGATAGGGGGAATTGGAGG-3′) and KS104 (5′-TGACTTGCCCAATTTAGTTTTCCCACTAA-3′) were used, respectively, in the forward and reverse RT-PCR reactions. A final PCR reaction volume of 25 μl included a 1×PCR buffer, 0.4 mM dNTPs, 1.5 mM MgCl2, 5 μl of RNA template, 1 μl enzyme mix, 0.6 μM of each primer, and 5 units of RNAseOut. Reverse transcription was performed at 50°C for 30 min followed by amplification steps of 15 min denaturation at 95°C and 40 cycles of denaturation at 94°C for 30 s, annealing at 55°C for 45 s, and extension at 72°C for 1 min. A final extension step was performed at 72°C for 10 min.
Second round PCR was done using HotStar taq polymerase (New England Biolabs) in a 25 μl reaction volume comprising 1×PCR buffer, 0.2 mM dNTPs, 2 mM MgCl2, 0.5 μM forward and reverse primers, 0.625 units of the enzyme, and 3 μl of RT-PCR product as template. The thermocycling profile comprised denaturation at 95°C for 5 min followed by 40 PCR cycles of 95°C denaturation for 30 s, annealing at 56°C for 45 s, and extension at 68°C for 45 s. Afinal extension was done at 68°C for 10 min. KS101 (5′-GTAGGACCTACACCTGTTCAACATAATTGGAAG-3′) and KS102 (5′-CCCATCCAAAGAAATGGAGGAGGTTCTTTCTGATG-3′) were used as forward and reverse nested PCR primer,s respectively. When DNA was used as the starting material, PCR procedures were similar except that the RT step was excluded. The PCR products were purified with Qiaquick purification columns and sequenced using standard Big-Dye chain terminator chemistry.
Sequences were manually inspected, joined in pairwise alignment (BioEdit ver. 7.2.5), and subjected to multiple sequence alignment using Clustal W (Supplementary Data; Supplementary Data are available online at
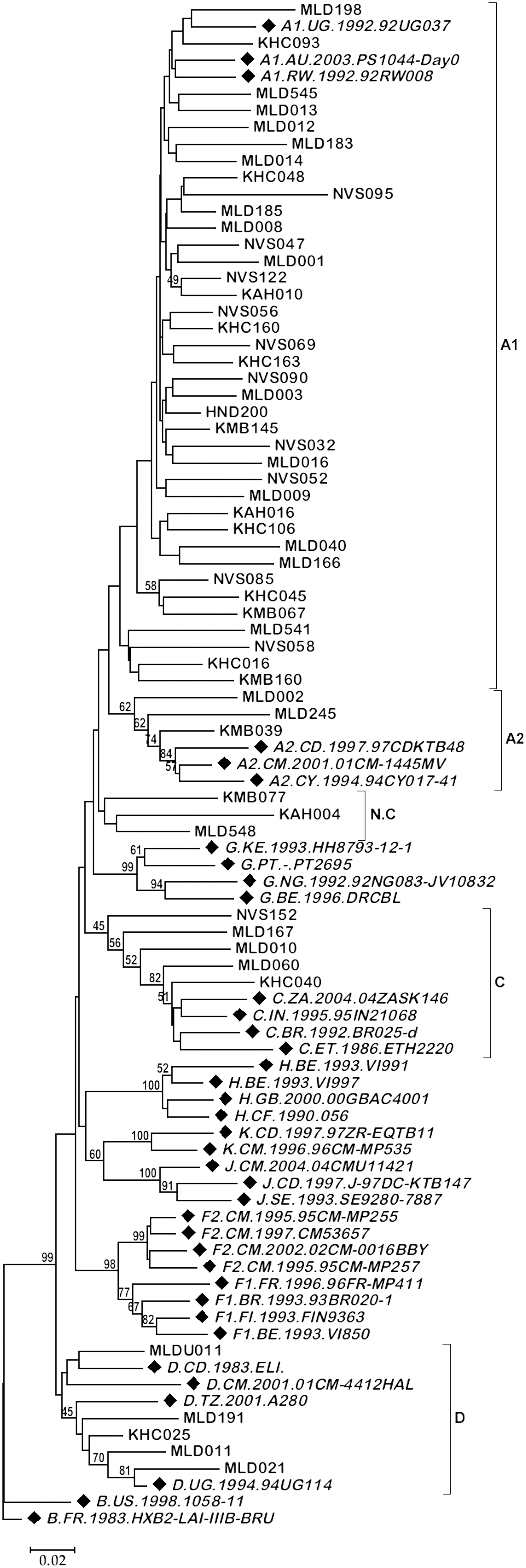
Phylogenetic tree of HIV pol-RT sequences from 54 highly active antiretroviral treatment (HAART) patients. The RT gene was partially sequenced using primers amplifying a 701-base pair region. Branches corresponding to partitions reproduced in less than 50% bootstrap replicates are collapsed and all positions with less than 50% site coverage were eliminated. Node statistics corresponding to less than 45% bootstrap values are hidden to minimize clutter. Reference sequences are italicized and shown by filled diamonds.
MLDU011 is an injecting drug use subject and is unique from MLD011.
NR, not reported; HAART, highly active antiretroviral therapy; N.C, not classified–sequence did not cluster discretely with any of the reference sequences; TDF, tenofovir; 3TC, lamivudine; NVP, nevirapine; d4T, stavudine; AZT, zidovudine; ABC, abacavir; EFV, efavirenz.
The phylogenetic method assigned more viruses as subtype A (76%), with the majority being A1 (70.4%). Seven of the 38 subtype A1 isolates were classified as A1A2 (n=2) or A1C (n=5) recombinants by JPHMM. The rest of the subtypes based on phylogenetics were HIV-1C at 9.3% and HIV-1D at 9.3%. Two sequences, MAD021 and MLD185, were substantially shorter than the rest, running just above half the length of the amplified RT gene segment. These isolates were identified by both methods as subtype D and A1, respectively, and are thus deemed to be accurately classified. Three isolates, KMB077, KAH004, and MLD548, that were determined as subtypes D, A1D, and D by JPHMM, respectively, did not cluster distinctly with any reference sequences on the phylogenetic tree and were “not classified” by this method.
Six (or 50%) of the recombinants were from the coastal region of Malindi. Of the 54 sequences, 27.8% contained reverse transcriptase inhibitor (RTI) drug resistance-associated mutations (DRAMs). Seventy-three percent of these mutations conferred resistance to both nucleoside RTIs (NRTIs) and nonnucleoside RTIs (NNRTIs), with the common ones being M184V/I and K103N, respectively. A few studies have recently endeavored to highlight differences in efficiency of different genotyping tools used for HIV subtyping. 14,15 We recently showed slight but useful differences in detecting HIV-1 subtypes based on the envelope C2V3 gene when using both the JPHMM and phylogeny. 10 This article reaffirms the same observations using the pol-RT gene, with both JPHMM and phylogenetic methods concurring on subtype assignment in 72.2% (39/54) of the isolates.
While subtype A HIV-1 is still predominant in Kenya, recombinant viruses may be on the rise. Whereas the phylogenetic method is robust at classifying HV strains based on evolutionary distances, it is not powered to detect recombinant viruses. Hence efficient detection tools should be developed or existing methods harnessed to sensitively identify small genetic differences that might influence the overall molecular pattern of the circulating epidemic. Such efforts will empower routine genetic surveillance to better inform public health and vaccine or drug discovery efforts.
GenBank Accession Numbers
The GenBank accession numbers are KM853096–KM853149.
Footnotes
Acknowledgments
This study was supported by the Consortium for National Health Research, Kenya, with funds from the Wellcome Trust (UK), grant RCDG-2012-005.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.