
Abstract
Sclerostin is linked to bone physiology and cardiovascular disease through the Wnt/β-catenin signaling pathway. The goal of this study was to determine if sclerostin is related to bone physiology and cardiovascular disease during antiretroviral treatment in HIV-infected persons. This was a cross-sectional analysis from study entry into the Stopping Atherosclerosis and Treating Unhealthy bone with RosuvastatiN in HIV (SATURN) trial, an ongoing randomized trial comparing rosuvastatin to placebo in HIV-infected adults on antiretroviral therapy. Plasma sclerostin was measured at study entry by ELISA from participants with available samples. Spearman correlation and multivariable linear regression were used to test relationships between sclerostin and bone density or bone turnover and cardiovascular disease. Among 139 HIV-infected participants (median age 46 years, CD4 lymphocyte count 614 cells/μl), the median plasma sclerostin level was 444.1 (IQR 330.3, 570.1) pg/ml. Correlations were detected between sclerostin and age (r=0.26), lumbar spine Z-score (r=0.31), RANKL (r=−0.21), carotid intima-media thickness (CIMT, r=0.19), and sVCAM-1 (r=0.27), p<0.05. No significant correlations were detected between sclerostin and current (r=0.006) or nadir CD4 count (r=0.11). While associations between sclerostin, lumbar spine Z-score, and sVCAM-1 were robust to covariate adjustment (p<0.01), association with CIMT was no longer significant (p=0.08). Our findings provide preliminary support for a relationship between sclerostin and bone mineral density in HIV-infected persons. The Wnt/β-catenin pathway should be investigated as a potential mechanism for loss of bone mineral density in treated HIV infection.
Introduction
S
The Wnt/β-catenin pathway is also involved in vascular physiology and calcification. 11,16,17 The occurrence of aggressive coronary artery disease in an extended family network prompted the recent discovery of a gene mutation in the Wnt pathway that has been associated with abnormalities in lipids, glucose, and bone. 18,19 The relationship between sclerostin and surrogate cardiac markers, however, is variable and depends on the population studied. Whereas some studies show a positive association between sclerostin and carotid intima-media thickness (CIMT), coronary artery calcium (CAC), and aortic artery calcification, 16,20,21 others show a negative correlation, particularly among persons with diabetes mellitus. 9,17
Low BMD and cardiovascular disease appear to occur more frequently among HIV-infected compared to HIV-uninfected persons, even after adjustment for confounding factors. 22,23 Increased risks of both low bone density and cardiovascular disease are likely the result of multiple traditional factors (age, gender, lifestyle, and substance use) and HIV-related factors, including low levels of inflammation and immune activation. The low BMD among HIV-infected persons is further precipitated by a nearly 5% decline in the initial 6–12 months following antiretroviral therapy (ART) initiation, 24,25 with the most pronounced declines seen among those taking tenofovir disoproxil fumarate (TDF). 26 In an aging population with multimorbidity and polypharmacy, targeting mechanistic pathways in a disease cluster is an appealing approach for therapeutic interventions. 27 This is particularly applicable to sclerostin as the monoclonal antibody, romosozumab, is in Phase III clinical trials. However, to the best of our knowledge, there is only one recently published study of sclerostin among persons with HIV infection. 28 Based on studies among HIV-uninfected populations, we hypothesized that plasma sclerostin would be positively associated with BMD and cardiovascular disease markers among HIV-infected persons on effective antiretroviral therapy.
Materials and Methods
Study design and participants
The SATURN-HIV (Stopping Atherosclerosis and Treating Unhealthy bone with RosuvastatiN in HIV) study is a randomized, double-blinded, placebo-controlled trial designed to measure the impact of daily rosuvastatin at 10 mg daily on cardiovascular disease and skeletal health (clinicaltrials.gov NCT01218802), as previously described. 29 –32 Randomization was stratified by protease inhibitor use at study entry, by the presence or absence of osteopenia (at either hip or spine) at study entry, and by the presence or absence of coronary calcifications by computed tomography (CT) scan. The current study is a post hoc, exploratory analysis at the study entry prior to initiation of study drug. Participants in SATURN-HIV were HIV-infected adults ≥18 years of age with a fasting low-density lipoprotein (LDL) cholesterol of ≤130 mg/dl and either a high sensitivity C-reactive protein (hsCRP) level of ≥2 mg/liter and/or ≥19% activated CD8+ T cells (coexpression of CD38 and HLA-DR). Additional eligibility criteria included receipt of stable ART for at least 12 weeks with a cumulative duration of ART of at least 6 months, plasma HIV-1 RNA ≤1,000 copies/ml, and no fragility fractures. Subjects were excluded for an active or chronic inflammatory condition (besides HIV), prior myocardial infarction, pregnancy/lactation, receipt of systemic chemotherapy or steroids, diabetes mellitus or thyroid disease, or use of anabolic agents, growth hormone, >81 mg aspirin daily, bisphosphonates, or teriparatide. All participants from SATURN-HIV were eligible for the present analysis if stored plasma was available. The study was approved by the Institutional Review Board of University Hospitals Case Medical Center (Cleveland, OH) and written, informed consent was provided by all participants.
Clinical assessments
At the initial visit, self-reported demographics, medical history, and HIV treatment history were obtained, with confirmation by medical records when available. A targeted physical examination included height and weight measurements. Blood samples were collected after a 12-h fasting period. HIV-1 RNA level and CD4 cell count were obtained as part of routine clinical care. Creatinine clearance was estimated by the Cockcroft–Gault equation. 33 Physical activity was estimated through a self-reported questionnaire as minutes per 2 weeks. 34
Dual-energy x-ray absorptiometry
Dual-energy X-ray absorptiometry (DXA) of whole body, lumbar spine (L1–4), and left hip BMD was performed in an anteroposterior view using Lunar Prodigy Advance (GE Healthcare, Madison, WI). Technicians used the same machine on the same subject throughout the study. All DXA scans were read at Case Medical Center by an experienced radiologist blinded to study information.
Cardiovascular assessments
CAC score and common CIMT were measured as previously described. 35 Briefly, calcified coronary lesions detected on chest CT scan were defined as areas of at least 6 pixels with density more than 130 Hounsfield units (HU). The total CAC score was quantified using the Agatston method. A high-resolution B-mode ultrasound scan of the carotid arteries was used to identify the presence of common carotid artery plaque, defined as a CIMT greater than 1.5 mm or more than 50% thicker than the adjacent vessel.
Measurements of bone turnover, inflammation, and activation
Plasma sclerostin was measured by quantitative sandwich enzyme-linked immunosorbent assay per the manufacturer's instructions (ELISA, R&D Systems, Minneapolis, MN). Samples were run in duplicate. One sample was excluded due to high intraassay variability of >20%. With this sample excluded, the intraassay variability was 3.8%. Other plasma and serum markers were measured as previously reported 30,31 and included 25-hydroxyvitamin D [25(OH)D]; bone turnover markers: intact N-terminal propeptide of type 1 procollagen (PINP), osteocalcin, c-terminal collagen crosslinks (CTX), RANKL, osteoprotegerin; cardiovascular disease markers: soluble vascular cell adhesion molecule-1 (sVCAM-1), intracellular adhesion molecule-1 (sICAM-1), and high sensitivity C-reactive protein (hs-CRP).
Statistical analyses
This study was a cross-sectional analysis. Continuous measures were described with medians and interquartile ranges (IQRs) and categorical measures with frequencies and percents. Unadjusted relationships of selected variables with sclerostin were estimated. Spearman correlation coefficients were used to estimate the relationship between sclerostin and continuous measures of markers of bone health and cardiovascular disease. Two-group nonparametric tests of significance (Wilcoxon rank sum tests) were used to estimate the relationships between sclerostin and categorical variables (e.g., race, sex). Multiple variable linear regression analysis was used to adjust for traditional bone or cardiovascular risk factors or factors known to impact sclerostin including age, race, sex, smoking, body mass index (BMI), physical activity, current CD4 count, serum 25(OH)D level, and creatinine clearance, with the addition of fasting glucose for CIMT and sVCAM-1. The level of significance was set at p=0.05 with no corrections for multiple comparisons. Analyses were performed using SAS v.9.3 (The SAS Institute, Cary, NC).
Results
Of the 147 overall participants in SATURN, 139 (95%) had available samples and were included in the current study. Baseline characteristics of the study population are summarized in Table 1. Briefly, the study participants had a median age of 46 years and were primarily male (78%) and black (67%). Participants had been taking ART for a median of about 6 years; 77% had a plasma HIV-1 RNA <50 copies/ml and the median CD4 lymphocyte count was 614 cells/μl.
ART, antiretroviral therapy; 25-OH, 25-hydroxy.
The plasma sclerostin ranged from 146.2 pg/ml to 1,568.3 pg/ml with a median of 444.1 pg/ml (IQR 330.3, 570.1 pg/ml) and mean of 469.4 pg/ml (standard deviation 194.9 pg/ml). As shown in Table 2, correlations were detected between plasma sclerostin and age (r=0.26), BMI (r=−0.17), estimated duration of HIV infection (r=0.19), Framingham Risk Score (r=0.22), 25(OH)D (r=0.26), creatinine clearance (r=−0.24), and fasting glucose (r=0.20); all p<0.05. Sclerostin levels were lower among females (median 382; IQR 290, 479 pg/ml) compared to males (median 462; IQR 347, 576 pg/ml; p=0.021) and black (median 419; IQR 326, 550 pg/ml) compared to nonblack participants (median 470; IQR 367, 595 pg/ml; p=0.045). No significant differences were seen between current smokers (median 424; IQR 330, 520 pg/ml) and prior or nonsmokers (median 476; IRQ 330, 580; p=0.37), those with plasma HIV-1 RNA <50 copies/ml (median 449; IQR 326, 573 pg/ml) versus detectable levels ≥50 copies/ml (424; IQR 341, 519 pg/ml; p=0.82), and those using tenofovir-containing (median 438; IQR 330, 565 pg/ml) versus nontenofovir regimens (median 519; IQR 326, 595 pg/ml; p=0.33)
BMD, bone mineral density; RANKL, receptor activator of NF-κB ligand; CTX, c-terminal collagen crosslinks; PINP, intact N-terminal propeptide of type 1 procollagen; sICAM-1, soluble intracellular adhesion molecule-1; sVCAM-1, soluble vascular cell adhesion molecule-1.
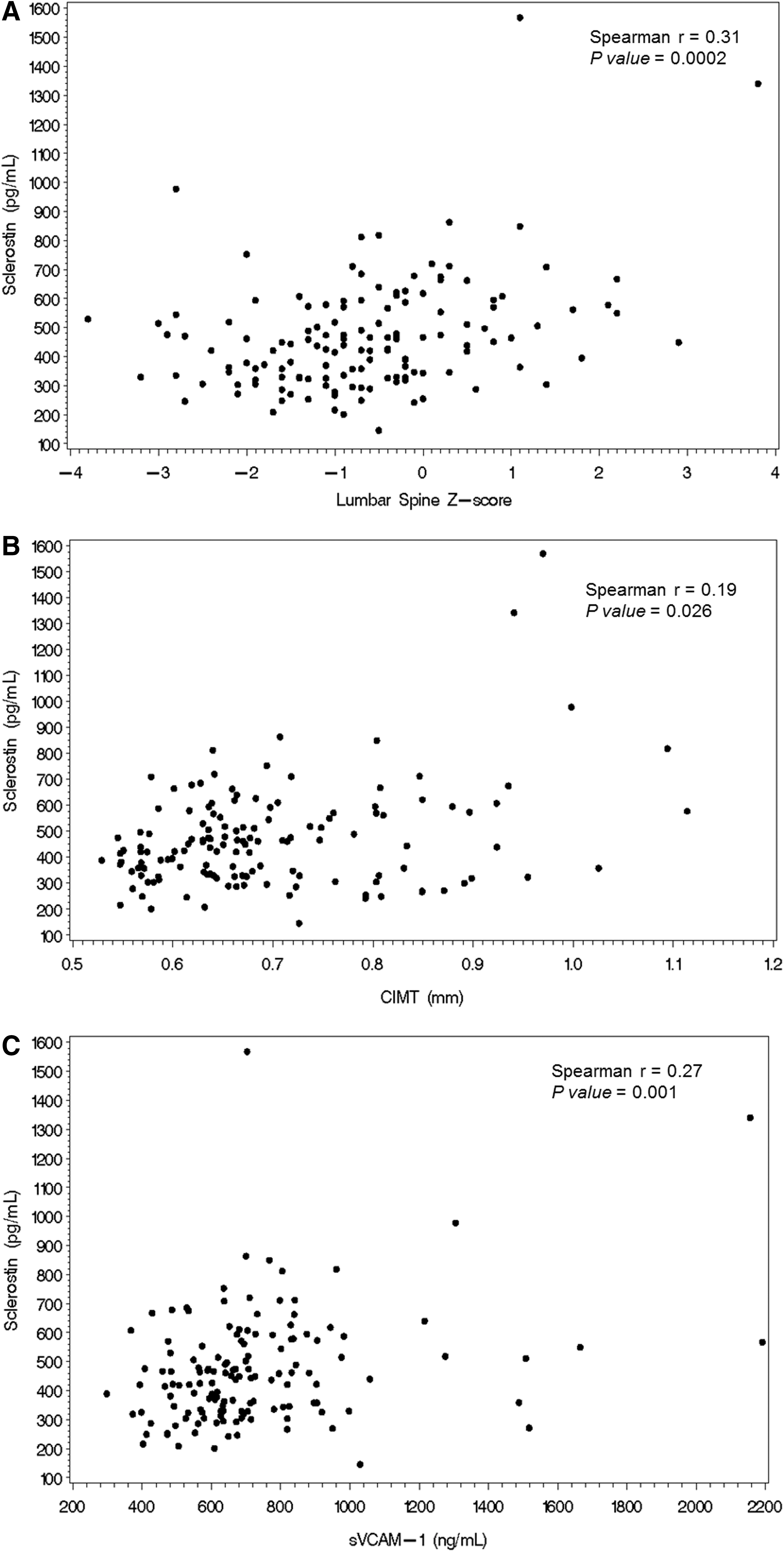
Positive correlations were detected between sclerostin and Z-scores at the total body (r=0.25), femoral neck (r=0.17), and lumbar spine (r=0.31), and a negative correlation was detected with RANKL (r=−0.21); all p<0.05. Correlations between sclerostin and BMD or other markers of bone turnover did not reach significance (Table 2). Positive correlations were detected between sclerostin and CIMT (r=0.19) and CAC score (r=0.19; p=0.028). There was a trend toward higher sclerostin levels among subjects with a CAC score greater than 0 (467 pg/ml; IQR 359, 1,568 pg/ml) compared to subjects with a score of 0 (422 pg/ml; IQR 330, 978 pg/ml; p=0.054). Among other markers of cardiovascular disease, only the correlation between sVCAM-1 and sclerostin was significant (r=0.27; p=0.001) (Table 2).
The associations between sclerostin, BMD (lumbar spine Z-score), and cardiovascular disease markers (CIMT, sVCAM-1) are shown in Fig. 1A–C. As shown in Tables 3 and 4, the association between lumbar spine Z-score and sVCAM-1 with sclerostin remained robust in multivariate models. In contrast, the association between CIMT and sclerostin was no longer statistically significant with inclusion of the covariates.
CIMT, carotid intima-media thickness; sVCAM-1, soluble vascular cell adhesion molecule-1.
Discussion
As the inhibitor of a common pathway in bone and vascular metabolism, sclerostin and the Wnt/β-catenin pathway are attractive targets for understanding the pathogenesis of the highly prevalent low bone mineral density and cardiovascular disease among HIV-infected persons. 22,36,37 Early murine and human models have demonstrated modulating effects of the antiretroviral agent ritonavir on osteoclast β-catenin activity, 38 with a recent study suggesting that the noncanonical Wnt5a/b pathway may have a role in the BMD loss of HIV-infected persons. 39 In a well-characterized, middle-aged cohort of HIV-infected persons on effective ART, we provide a detailed description of sclerostin in HIV infection, crucial preliminary data providing support for Wnt/β-catenin as a possible pathway for BMD loss in HIV infection.
Counterintuitive to what would be expected, but consistent with prior reports in persons without HIV infection, higher plasma sclerostin levels were associated with less evidence of low bone mineral density, with the strongest associations seen at the lumbar spine. 7 –11 Limited data suggest that sclerostin is associated more strongly with trabecular than cortical bone, providing support for the stronger association between systemic sclerostin levels and the vastly trabecular lumbar spine rather than hip BMD in both our study and others. 7,8,11,40 The inclusion of traditional bone risk factors had little impact on the association between sclerostin and the lumbar spine Z-score. We observed a negative correlation of sclerostin with RANKL, a marker of osteoclastogenesis, but no significant correlations with markers of bone resorption or formation. This is in contrast to cross-sectional studies from HIV-uninfected populations demonstrating a positive correlation between sclerostin and the resorption marker CTX, 41,42 and findings from the Phase II trial where, following an initial increase, romosozumab led to a significant reduction in CTX compared to placebo. 14
The positive associations of sclerostin with known duration of HIV infection and duration of ART are likely explained by the positive correlation with age, a finding consistently reported in other populations. 43 Although we found no association between sclerostin and CD4 count, nadir CD4 count, or HIV-1 RNA, all of our participants were on ART, and the majority had an undetectable plasma HIV-1 RNA.
In vitro, sclerostin has been shown to be upregulated in the vascular wall during calcification, thus the association between sclerostin and markers of vascular disease or calcium deposition (CIMT and CAC score) was consistent with our hypothesis. In other disease states, such as diabetes, sclerostin levels were also associated with CIMT and aortic calcifications. 21 It is notable that our study included only subjects without diabetes or known cardiovascular disease and whose LDL-cholesterol was <130 mg/dl, which may have limited our ability to detect stronger findings. We did detect a highly significant relationship between sclerostin and sVCAM-1 that was robust to adjustment of underlying cardiovascular risk factors and has not previously been reported in the literature. This association may be explained through several pathways: sVCAM-1, an adhesion molecule released by vascular endothelium, is negatively regulated by Wnt signaling, similar to sclerostin 44 ; bone microvasculature is closely linked to bone remodeling 45,46 ; and sVCAM-1 is expressed in the surface of osteoblasts. 47,48
The primary strength of the study lies in the comprehensive assessment of BMD, bone turnover markers, and cardiovascular disease markers in a well-characterized population of effectively treated HIV-infected subjects from a single site. Our study has several limitations. The study population was primarily male, black, and younger than many other studies reported in the literature, with a low prevalence of osteopenia; thus our results may not be generalizable to other populations. Plasma sclerostin levels may not reflect processes at the level of the bone: some authors have suggested that peripheral levels of sclerostin may not be sensitive enough to detect changes at the level of the bone, 7 whereas others have demonstrated a strong correlation between serum and bone marrow levels of sclerostin. 49
Based on sample availability, we used the plasma sclerostin that has been shown to correlate strongly (r=0.9) with serum sclerostin levels but is approximately 30% higher. 50 For comparison, the median plasma levels in our cohort were markedly lower than those reported in a population of black, middle-aged persons with type 2 diabetes (median 1040 pg/ml) using the same plasma assay. 9 These differences should be validated in an appropriate HIV-uninfected control group with similar age, race, and risk characteristics, with assays completed in the same laboratory. Similarly, our cross-sectional findings should be investigated longitudinally to elucidate directionality. We chose lumbar spine measures to further investigate in the multivariate models due to the strength of the association, but acknowledge that other factors can impact lumbar spine osteoporosis, including arthritis or abdominal aortic calcification. Physical activity was collected only by self-report; differences may have been detected between sclerostin and physical activity with more objective measures. Finally, no corrections for multiple comparisons were done and associations should be considered exploratory.
In summary, we report the first analysis of sclerostin among HIV-infected adults. Our results demonstrate an independent relationship between sclerostin and lumbar spine Z-score. Importantly, the antisclerostin antibody romosozumab will allow for mechanistic studies of the effects of sclerostin inhibition in people with HIV. Targeted inhibition of sclerostin and the Wnt/β-catenin pathway should be investigated as potential pathways to decrease cardiovascular and bone-related morbidity in persons aging with HIV.
Footnotes
Acknowledgments
This study was supported by funding through the National Institutes of Health (NR012642 to G.A.M., K23AG050260 to K.M.E., and K23HL116209 to C.O.H.). The contents are the authors' sole responsibility and do not necessarily represent official NIH views.
Author Disclosure Statement
G.A.M. has served as a scientific advisor or speaker for Bristol Myers Squibb, Pfizer, ViiV, Janssen, ICON Merck, and Gilead Sciences, has received research grants from Bristol Myers Squibb, GlaxoSmithKline, and Gilead Sciences, and has served as the Data Safety and Monitoring Board Chair for a Pfizer-sponsored study.