
Abstract
Vaginal microbicide gels containing tenofovir have proven effective in HIV prevention, offering the advantage of reduced systemic toxicity. We studied the vaginal distribution and effect on mucosal permeability of a gel vehicle. Six premenopausal women were enrolled. In Phase 1, a spreading gel containing 99mtechnetium-DTPA (99mTc) radiolabel and gadolinium contrast for magnetic resonance imaging (MRI) was dosed intravaginally. MRI was obtained at 0.5, 4, and 24 h, and single photon emission computed tomography with conventional computed tomography (SPECT/CT) at 1.5, 5, and 25 h postdosing. Pads and tissues were measured for activity to determine gel loss. In Phase 2, nonoxynol-9 (N-9), containing 99mTc-DTPA, was dosed as a permeability control; permeability was measured in blood and urine for both phases. SPECT/CT showed the distribution of spreading gel throughout the vagina with the highest concentration of radiosignal in the fornices and ectocervix; signal intensity diminished over 25 h. MRI showed the greatest signal accumulation in the fornices, most notably 1–4 h postdosing. The median (interquartile range) isotope signal loss from the vagina through 6 h was 29.1% (15.8–39.9%). Mucosal permeability to 99mTc-DTPA following spreading gel was negligible, in contrast to N-9, with detectable radiosignal in plasma, peaking at 8 h (5–12). Following spreading gel dosing, 0.004% (0.001–2.04%) of the radiosignal accumulated in urine over 12 h compared to 8.31% (7.07–11.01%) with N-9, (p=0.043). Spreading gel distributed variably throughout the vagina, persisting for 24 h, with signal concentrating in the fornices and ectocervix. The spreading gel had no significant effect on vaginal mucosal permeability.
Introduction
P
Previous HIV microbicide gel imaging studies added gadolinium contrast to the candidate gel followed by serial magnetic resonance imaging (MRI) studies over several hours. 3 –10 These images provided good anatomic resolution and location of gel signal, but they provided little quantitative data that can be translated into concentration within an anatomic compartment such as the vagina. Qualitatively, these studies have shown localization of gels within the vagina, with the most intense signal observed within the fornices, and spreading of the gel distally toward the introitus over time. Quantitative measures have been limited to examining either linear distance of gel migration in a sagittal plane or transverse spread at four prespecified anatomic levels along with longitudinal spread of the gel signal in the fornices in the sagittal plane, described as a percentage of the maximum of gel spread over time. A single study compared planar gamma scintigraphy with MRI to study vaginal microbicide vehicle distribution; however, the reported data were limited to describing the percentage of the maximum linear distance covered by the gel over 50 min. 11
We previously reported using single photon emission computed tomography along with x-ray computed tomography (SPECT/CT) to describe the rectal distribution of radiolabeled drug formulations. 12,13 Recently, we also used SPECT/CT to model the vaginal distribution of HIV surrogates following simulated intercourse using HIV-sized particles and autologous radiolabeled lymphocyte-enriched white blood cells mixed within a simulated seminal fluid delivered via an artificial phallus. 14 SPECT/CT has lower resolution than MRI, but some advantages in regard to quantitative assessments. Also, we used small molecule-sized SPECT/CT radiocontrast agents, e.g., 99mtechnetium-diethylene triamine pentaacetic acid (99mTc-DTPA) to simultaneously examine changes in vaginal mucosa permeability, defined as migration of radiolabel across the mucosa with subsequent detection of gamma activity in plasma or urine, following gel administration. Such changes may be reflective of tissue disruption as seen with nonoxynol-9 (N-9) that may increase the risk for HIV transmission. 15
A vaginal gel with spreading characteristics was formulated (CONRAD; Arlington, VA) in order to facilitate rapid coverage of the vaginal compartment with the gel vehicle. The present study was designed to compare the distribution, concentration, and persistence of this spreading gel formulation in the female genital tract through 24 h using both SPECT-CT and MRI. We also compared the spreading gel effects on vaginal mucosal permeability with N-9 as the positive control.
Materials and Methods
Human subjects
The research protocol was approved for human subjects by the Johns Hopkins institutional review board. Following written informed consent, research participants were screened for study eligibility. To meet the enrollment criteria, women needed to be greater than age 18 years, use an effective and reliable form of contraception, have had a normal Pap smear at screening or within the past year, and show no evidence of active sexually transmitted infection, bacterial vaginosis, or candidiasis. Exclusion criteria included an immediate desire for childbearing, pregnancy, irregular menstrual bleeding, menopause, surgery or biopsy of the female genital tract in the prior 30 days, genital tract anatomic abnormality, hysterectomy, endometritis, or pelvic inflammatory disease in the prior 30 days, and known contraindication to MRI. Of the eight subjects providing consent, one subject was excluded due to a positive pregnancy test at screening. Another subject was excluded due to an abnormal Pap smear at screening that required medical follow-up.
Design
This was a comparative, open-label two-period crossover study to evaluate the distribution and retention of a 3.5 ml dose of a spreading gel and to compare vaginal mucosal permeability of the spreading gel with a 3.5 ml dose of N-9 gel as a positive control. Gadolinium and 99mTc-DTPA were mixed into the spreading gel to facilitate imaging. Since no imaging was conducted with the N-9 intervention, the N-9 formulation was mixed with 99mTc-DTPA only. Following the screening visit, research participants underwent two study intervention visits—an imaging visit for the spreading gel followed by the N-9 positive control permeability assessment visit. The day of each dosing visit, a serum pregnancy test was obtained and confirmed negative prior to proceeding with gel administration.
Following gel dosing, MRI was performed at 30 min, 4 h, and 24 h after gel application. SPECT/CT imaging was obtained at 1.5, 5, and 25 h following dosing. Blood was collected at 0.25, 0.5, 0.75, 1, 1.5, 2, 2.5, 3, 3.5, 4, 4.5, 5, 6, 8, 12, 16, and 24 h after gel insertion and plasma was separated for measurement of 99mTc. Urinary excretion of radioactivity was measured by timed urine collections at 0–1, 1–3, 3–6, 6–12, and 12–24 h postdosing. A sanitary pad was placed following gel dosing and changed just prior to each SPECT/CT procedure. The pads and any tissue paper used following urination were saved and counted for radioactivity to account for leakage of isotope from the introitus.
Procedures
Gel preparation and administration
The spreading gel formulation, a hydroxyethyl cellulose-based gel with ingredients and physical characteristics similar to Universal Placebo, was provided by CONRAD (Arlington, VA; osmolality: approximately 900 mosmol/kg). 16 Commercially available 4% N-9 (Conceptrol; osmolality: 1257 mosmol/kg; Advanced Care Products, Raritan, NJ) was obtained to serve as the positive permeability control. To assist with visualization on MRI, a 1:100 dilution of gadoteridol, a gadolinium-based contrast agent (ProHance; Bracco Diagnostics, Princeton, NJ), was added to the spreading gel vehicle. Then 3.5 ml volumes of each test vehicle were compounded with 500 μCi of 99mTc-DTPA that had previously been prepared by a commercial radiopharmacy (Cardinal Health, Beltsville, MD) and delivered to the nuclear medicine facility at The Johns Hopkins Hospital.
Once labeled, the syringe containing the gel vehicle was attached by a connector to a second syringe. To facilitate mixing, a series of 10 exchanges between syringes was completed. Radioactivity of the gel-containing syringe was measured in a dose calibrator (CRC 15-W; Capintec, Ramsey, NJ) and the time of measurement was recorded. Subjects were placed in a supine position, and the compounded isotope vehicle was injected in the upper vaginal canal, where slight tissue resistance was felt (approximating either the anterior vaginal fornix, or external surface of the cervix, using a rectal-vaginal luer applicator (product 35-1107; Professional Compounding Centers of America, Houston, TX) attached to the dosing syringe. Following dosing, the residual radioactivity in each syringe was measured. This amount was decay corrected and subtracted from the initial syringe measurement to determine the total dose administered to the subject. Subjects remained supine until completion of the first SPECT/CT imaging time point.
SPECT/CT imaging
Pelvic SPECT/CT images were acquired as previously described 14 at approximately 1.5, 5, and 25 h after gel dosing. Briefly, images of the radiotracer were acquired using a dual-head VG series system (GE Medical Systems) equipped with a low-dose CT unit (Hawkeye). CT images were acquired before SPECT images. CT scans (1-cm thickness; step-and-shoot mode; 140 kVp; 1.0 mA; 180 degree fan angle) were acquired from the thorax to the upper one-third of the femur over a 213 degree arc. CT images were reconstructed with filtered back-projection onto a 256 by 256 matrix. Noise correction was performed using automatic body contouring to optimize signal and resolution. Image acquisition was performed with a 20% 99mTc energy window centered at 140 keV. Each SPECT acquisition was 35 min. The SPECT images were then reconstructed into a 128 by 128 matrix size using an iterative ordered subset–expectation maximization (OSEM) algorithm. SPECT images were also compensated for attenuation, scatter, and detector resolution blur during reconstruction.
MR imaging
MR images were acquired at 1, 4, and 24 h following gel dosing. Images were acquired using a 3.0-T whole-body TRIO imager (Siemens Medical Solutions USA) using the Total Image Matrix body matrix coil (Siemens Medical Solutions USA). Participants were imaged in the supine position. The following sequences were obtained: (1) sagittal, T2-weighted images with fat suppression [7470/160 [repetition time (TR) ms/echo time (TE) ms]; section thickness, 3 mm; intersection gap, 0.9 mm]; (2) axial, T2-weighted turbo spin-echo images (9670/116; section thickness, 3 mm; intersection gap, 0.9 mm); and (3) three-dimensional T1-weighted gradient-echo images with fat suppression (8.8/3.2; section thickness, 2 mm; intersection gap, 0 mm; flip angle, 10°). Three-dimensional T1-weighted gradient-echo MR images were reconstructed into axial, coronal, and sagittal images for qualitative analysis of contrast distribution.
Region of interest analysis
SPECT/CT images were evaluated semiquantitatively by region of interest (ROI) analysis of selected transaxial images using GE Healthcare Xeleris image reconstruction software (Version 2.0; Waukesha, WI). Three corresponding anatomic transaxial slices were selected for each subject and for each of the three imaging intervals—1.5 h, 5 h, and 25 h following gel dosing. These slices were defined as the Lower Vagina (the mid-point of the symphysis pubis identified on a transaxial image), the Forniceal Region (where the femoral head inserts into the acetabulum), and the Vaginal Midpoint (the vertical distance halfway between the lower vagina and the forniceal region transaxial slices). Within each transaxial image, ROIs were drawn around distinct areas of signal intensity, and the resulting mean number of counts per voxel in that ROI was obtained. The results were then paired and compared within individuals across time and anatomic location.
Gamma counting
Gamma emissions in all blood and interval-based urine specimens were measured on a gamma counter (Wizard 2 automatic gamma counter model 2480, PerkinElmer, Waltham, MA) within a 110- to 150-keV energy window. Samples were corrected for background activity and instrument detector efficiency. Gamma emission limit of quantitation was defined as background+(3× square root of background). Any gamma counts below this value (approximately 22 cpm) were considered “0” and considered not distinguishable from naturally occurring background radiation. To determine the cumulative urine gamma activity for a specified interval, gamma counts for urine aliquots were corrected for urine volume and sampling interval duration. Plasma and urine results were then decay corrected to account for time elapsed and were divided by the total amount of activity administered, to normalize for the dose retained by each subject. Plasma and urine results are expressed as a fraction of the initially administered isotope dose. Sanitary pads and paper tissues were measured in the dose calibrator and all measured values were decay corrected to the time of gel administration.
Data analysis
Within subject paired comparisons were made between SPECT/CT imaging time and anatomic location for the spreading gel vehicle. Similar paired comparisons were conducted for gel assignment and plasma mucosal permeability data, as well as for activity detected on sanitary pads and tissue wipes. Statistical testing was done using the Wilcoxon sign rank test (SPSS Version 21, SPSS IBM, Armonk, NY). For the N-9 dosing arm, peak isotope concentration (C max) and time to peak concentration (T max) were assessed by visual inspection. Area under the isotope concentration curve over 24 h (AUC0–24) was calculated using the linear trapezoidal rule. MRI images were evaluated qualitatively for the presence or absence of signal in transaxial slices that corresponded with SPECT/CT images obtained within the same hour. Sanitary pad and paper tissue wipe activity analysis was limited to the first 6 h, due to low signal detection and overnight isotope signal decay. Urine isotope measurement was expressed as the cumulative percentage of the dose administered detected within the defined time interval. Data are reported as median [interquartile range (IQR)] unless otherwise stated.
Results
Six women completed the study. Four participants were African American and two were white. Their age ranged from 36 to 48 years. Individuals were dosed 12 (8–14) days prior to onset of menses in the spreading gel arm and 13 (7–17) days prior to menses in the N-9 arm. Each subject received the spreading gel and N-9 doses within 3 (1–3) days of the same phase of the menstrual cycle. One subject was amenorrheic on oral contraceptives. N-9 administration was incorrectly dosed in one subject and the resulting data were excluded from analysis.
The greatest concentration of radiosignal was 1,959 (804–3,642) mean counts per voxel, measured in the fornices at the first imaging time point, approximately 1.5 h after dosing (Table 1). A signal intensity gradient extending between transaxial planes from the Forniceal Region to the Lower Vagina Region was also observed with the median counts per voxel in the lower vagina being 627 (247–1,186) at the same time point. Furthermore, the gel appears to provide coverage throughout a 25 h dosing interval, though the isotope concentration is approximately 5-fold lower in all regions 25 h after dosing.
Paired comparison of anatomic site to Lower Vagina; p<0.08.
Paired comparison (within anatomic site) with 25 h concentration; p<0.08.
T1-weighted MR images showed gadolinium enhancement throughout the vaginal canal, with evident forniceal pooling by 4 h (Fig. 1). There was no detectable uterine distribution at any time point. At 24 h, signal enhancement persisted in the same distribution but appeared to show less contrast to the surrounding vaginal mucosa. The intensity of the gel signal on MRI appeared to qualitatively correlate with the location and signal intensity of the isotope observed on SPECT/CT.
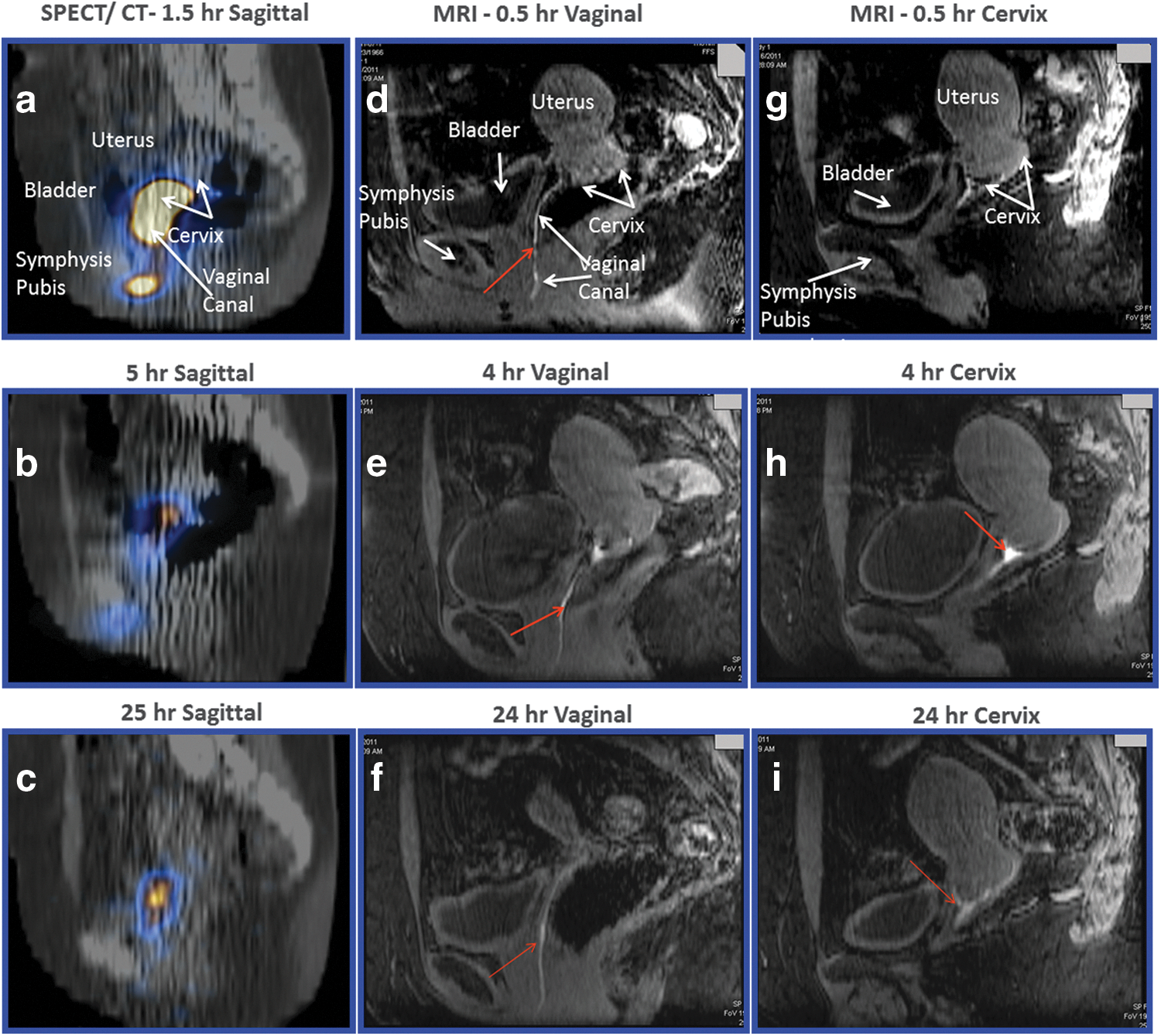
Magnetic resonance imaging (MRI) and single photon emission computed tomography/computed tomography (SPECT/CT) images of a typical subject.
Following the spreading gel dose, isotope was detectable in a single plasma sample in each of two of the subjects. There was no signal above detection limits in any plasma samples from the other four subjects (Fig. 2). In contrast, following 4% N-9 dosing, isotope was detectable in plasma samples among five of five subjects, indicating significantly greater vaginal mucosal permeability. Expressed as pharmacokinetic parameters, the N-9 permeability had an area under the curve 1.01×10−5 (0.56–1.34) fraction of dose administered h/ml, C max of 0.07×10−5 (0.04–0.11) fraction administered dose/ml, and T max of 8.05 h (6.52–8.05) (Table 2).
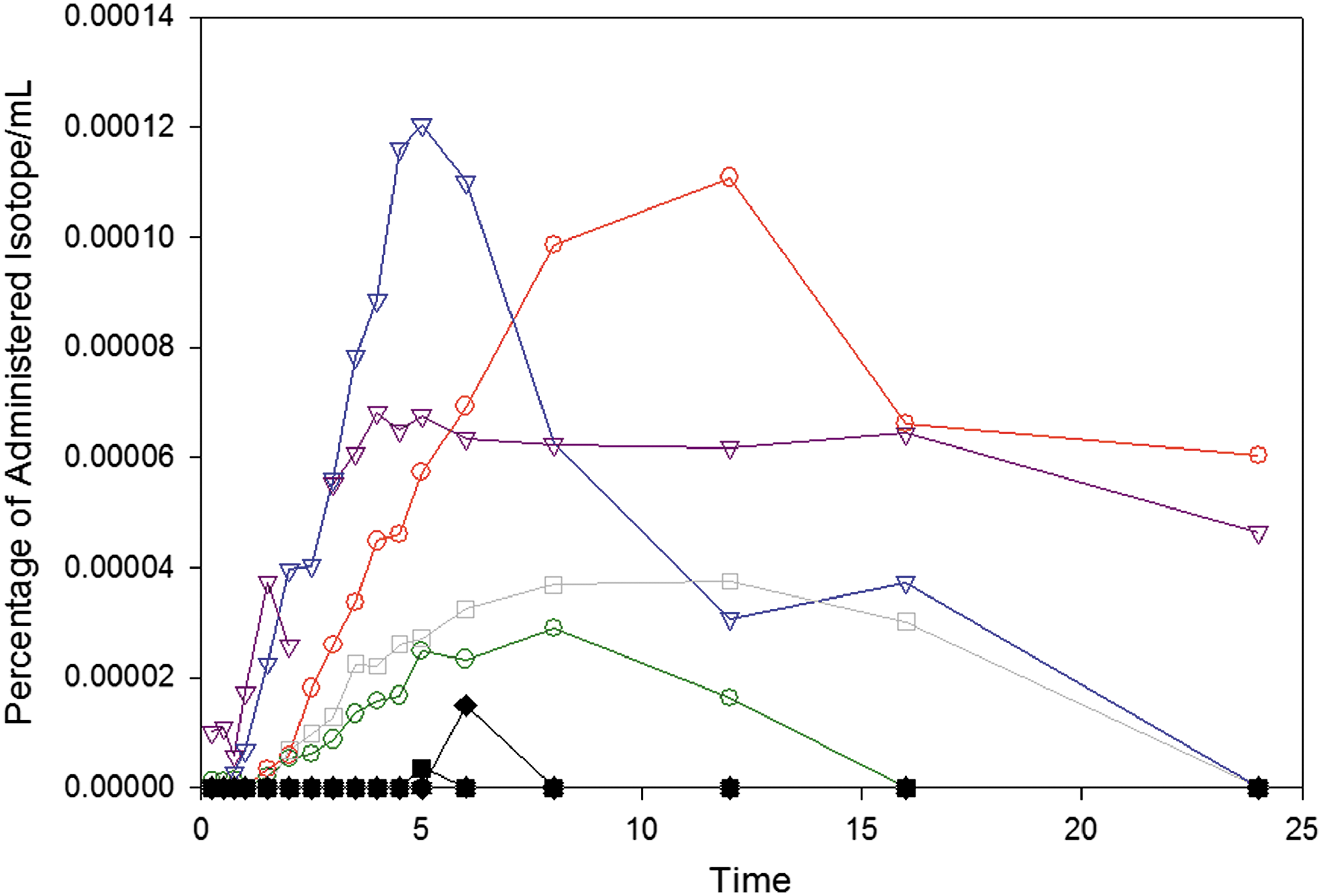
Plasma 99m-technetium (99mTc) levels for each research subject over time, following a single vaginal dose of 4% nonoxynol-9 gel (color lines, open symbols) and the spreading gel (black lines, closed symbols). The y-axis denotes 99mTc disintegrations per minute (DPM) as a percentage of the dose administered.
p<0.05 using Wilcoxon sign-rank test compared to spreading gel.
p=0.08.
BLQ, below limit of quantitation; PK, pharmacakinetic.
There was a statistically significant difference in paired cumulative gamma activity in the urine beginning 1 h following dosing (Table 2). Expressed as percent of dose administered, a median of 0.002% (0.000–0.009) of administered gamma activity was detected in the urine of subjects following the spreading gel dosing, compared to 0.132% (0.008–0.836) following N-9 dosing. This cumulative difference remained statistically significant through the first 12 h following dosing, with medians (IQR) of 0.004% (0.001–2.04%) and 8.31% (7.07–11.08%), respectively, p=0.043.
Significant loss of isotope via the introitus, as measured on sanitary pads and paper tissues, occurred in the first 6 h following dosing. Signal loss was 26.8% (12.2–45.0%) for spreading gel and 29.1% (16.4–39.6%) for N-9, which was not statistically different. Overall, the loss of signal was 29.1% (15.8–39.9%) combining both gel formulations.
Discussion
SPECT/CT and MRI are complementary imaging modalities for describing the distribution and relative gel concentration in the lower female genital tract over 24 h. Qualitatively, the MRI data provided more distinct anatomic localization of the gel signal given its far greater resolution, but was generally consistent with the observations made on SPECT/CT.
Anatomic distribution of the spreading gel was limited to the vaginal canal and fornices, with the greatest signal enhancement in the fornices. We could not detect gel within the cervical canal or uterus. This is consistent with previous observations of a variety of vaginally applied gels. 3 –11 Similarly, the relative distribution of gel signal initially localized in the forniceal region with spread toward the introitus over time is consistent with prior observations in these same MRI studies. While our paired comparisons of SPECT/CT data suggest differences in relative anatomic distribution at the same time point as well as over time, the small sample size of this pilot study limits our ability to detect true differences that might be seen with a more formal statistical analysis and larger sample size. Detection of radiolabel on sanitary pads and paper tissues indicates significant gel leakage from the introitus, which has implications for gel formulation, dosing, and reapplication if multiple acts of vaginal sexual intercourse occur within that timeframe. Evaluation of gel loss following intercourse paired with tissue drug uptake would be additionally beneficial in assessing the adequacy of gel coverage in the pericoital context.
The data presented here suggest that shortly following intravaginal gel administration, relatively higher concentrations of an active pharmaceutical ingredient could be achieved and maintained within the region of the fornices and external surface of the cervix than in the lower vagina. This effect persists over 25 h, though the concentration gradient decreases over time. If the critical anatomic region to protect against establishment of HIV infection is the exterior surface of the cervix, the ability to deliver relatively higher concentrations of drug to the cervix could be reasonably achieved with this gel formulation. Alternatively, relatively lower concentrations are observed in the lower vagina, suggesting that if adequate coverage of the entire vaginal canal is necessary to prevent HIV transmission, gel formulation and dosing may need to take this into account.
To this point, the distribution observed for the spreading gel is consistent with our prior studies of HIV surrogate distribution within the lower female genital tract when mixed with fluid simulating semen in which both cell-free and cell-associated HIV surrogates migrate to the same pericervical location. 14 Suitability of a vaginal microbicide gel's spreading characteristics might best be studied by dual isotope labeling experiments in which we compare the distribution and clearance of a radiolabeled candidate microbicide gel vehicle administered prior to simulated sex and ejaculation with a different isotope-labeled HIV surrogate. We have previously used this approach in rectal microbicide gel development. 16
The 2.1 log10 greater urine isotope accumulation indicates a very large increase in vaginal mucosal permeability following N-9 administration, which peaked 6–8 h after dosing. In contrast, the spreading gel had very low vaginal mucosal permeability by our measure. Without a baseline permeability for comparison, we cannot state that there was no effect of the spreading gel on vaginal mucosal permeability, but any such effect appears to be quite small. While the clinical significance of increased vaginal mucosal permeability resulting from N-9 is not clear, these data are consistent with in vitro, ex vivo, and animal models that have demonstrated disruption of the mucosal barrier by N-9, which may increase the risk of HIV transmission. 17 –20
In comparison with our prior work with the rectal permeability of isotope in the presence of N-9, the median dose-adjusted AUC0–24 and C max were 5-fold and 10-fold lower, respectively, compared to rectal data. 13,15 Similarly, T max was reached several hours later than what was observed with rectal dosing. Taken together, these data suggest that the vaginal mucosa is less susceptible to permeability-related injury compared to the rectal mucosa, likely due to histologic differences of vaginal stratified squamous versus rectal columnar epithelium. The relative difference in mucosal susceptibility may actually be greater than observed since the two studies used differing formulations of N-9—2% Gynol II for the rectal study compared with 4% Conceptrol for the current study.
Interestingly, the cumulative fraction of isotope collected over 24 h after N-9 from the urine was about 1.5 times higher than the value observed with rectal dosing of N-9. However, we used the clean catch urine collection method and not bladder catheterization, which would have largely avoided vaginal fluid contamination of urine collections. This potential for vaginal gel contamination of urine isotope limits our ability to compare rectal and vaginal permeability using urine isotope accumulation. It may introduce variability of product comparisons in this study, but the potential for contamination would affect both product assessments.
A limitation of the current study design is the resolution of SPECT/CT, which limits the ability to make conclusions about the degree of surface coating or penetration into the rugae, which will influence drug delivery to the tissues. The use of MRI as a complementary imaging modality can help to address these concerns, but better computational models for fusing SPECT/CT and MRI images for quantitative purposes are still in development.
The SPECT resolution has been less important in our rectal microbicide drug distribution studies where there is a far larger distribution of product within the distal colon and the resolution differences are diminished and the MRI signal is confounded by signal from colonic contents other than gadolinium-labeled product. Furthermore, while the radiolabel can provide information on the potential distribution of a drug-sized molecule, it can be considered only a representative model, since an API may have different tissue permeability characteristics based on size, dynamic polar surface area, charge, lipid solubility, and drug transporters. The relative concentrations described as counts per voxel at a particular anatomic level can be considered as an approximate surrogate for drug concentration only in a transverse section. Nevertheless, this method might be validated in future studies by correlating concentrations of API and radiolabel contained in the same gel vehicle. Similarly, changes in permeability for one small molecule may indicate relative changes in permeability for other small molecules. However, changes in small molecule permeability may have very limited relevance for HIV infectivity.
The use of SPECT/CT in combination with MRI can provide complementary anatomic and quantitative imaging data on gel distribution and concentration following intravaginal dosing. Furthermore, the 99mTc-DTPA radiolabel used for SPECT/CT can also be used as a surrogate measure of vaginal mucosal permeability that can describe the relative effect of different gel formulations on some aspects of the structural integrity of the vaginal mucosa. While the significance of alteration of vaginal mucosal permeability for either increasing tissue toxicity or susceptibility to HIV infection remains to be determined, use of this method with other gel formulations may help to further characterize alterations in tissue permeability that have clinical significance. Thus, the use of this combination of imaging modalities along with measuring associated mucosal permeability changes may enhance the process of topical gel formulation development.
Footnotes
Acknowledgments
We would like to express our appreciation to Stephanie Everts, CCRC, research coordinator for the study protocol, and Ms. Maleeha Memon, BS, who assisted in organizing the data for analysis. Lastly, we would like to express our gratitude to the women who volunteered and dedicated their time to participating in this research study.
This work was supported by CONRAD, Eastern Virginia Medical School under a Cooperative Agreement (GPO-A-00-08-00005-00) with the United States Agency for International Development (USAID) and by the Johns Hopkins Institute for Clinical and Translational Research (ICTR) that is funded in part by grant UL1 TR 000424-06 from the National Center for Advancing Translational Sciences (NCATS), a component of the National Institutes of Health (NIH), and NIH Roadmap for Medical Research. Its contents are solely the responsibility of the authors and do not necessarily represent the official view of the Johns Hopkins ICTR, NCATS, USAID, Eastern Virginia Medical School, or NIH.
These results were previously presented at the following conference: Microbicides 2012, Sydney, April 15–18, 2012.
Author Disclosure Statement
Mr. Fuchs and Dr. Hendrix received grant support from CONRAD to conduct this study.