
Abstract
Many HIV-infected individuals do not enter health care until late in the infection course. Despite encouraging earlier testing, this situation has continued for several years. We investigated the prevalence of late presenters and factors associated with late presentation among HIV-infected patients in an Asian regional cohort. This cohort study included HIV-infected patients with their first positive HIV test during 2003–2012 and CD4 count and clinical status data within 3 months of that test. Factors associated with late presentation into care (CD4 count <200 cells/μl or an AIDS-defining event within ±3 months of first positive HIV test) were analyzed in a random effects logistic regression model. Among 3,744 patients, 2,681 (72%) were late presenters. In the multivariable model, older patients were more likely to be late presenters than younger (≤30 years) patients [31–40, 41–50, and ≥51 years: odds ratio (OR) = 1.57, 95% confidence interval (CI) 1.31–1.88; OR = 2.01, 95% CI 1.58–2.56; and OR = 1.69, 95% CI 1.23–2.31, respectively; all p ≤ 0.001]. Injecting drug users (IDU) were more likely (OR = 2.15, 95% CI 1.42–3.27, p < 0.001) and those with homosexual HIV exposure were less likely (OR = 0.45, 95% CI 0.35–0.58, p < 0.001) to be late presenters compared to those with heterosexual HIV exposure. Females were less likely to be late presenters (OR = 0.44, 95% CI 0.36–0.53, p < 0.001). The year of first positive HIV test was not associated with late presentation. Efforts to reduce the patients who first seek HIV care at the late stage are needed. The identified risk factors associated with late presentation should be utilized in formulating targeted public health intervention to improve earlier entry into HIV care.
Introduction
I
The Therapeutics Research, Education, and AIDS Training in Asia (TREAT Asia) HIV Observational Database (TAHOD) is a multicenter, observational cohort study that was initiated in 2003 to assess regional HIV treatment outcomes in the Asia-Pacific region. 14 In this study, we aimed to describe trends in late presentation into care and to determine associated factors in TAHOD.
Materials and Methods
Study population
We analyzed data from TAHOD, a prospective, observational cohort study of HIV-infected adults at 22 sites in the Asia-Pacific region that was established in 2003 (see Supplementary data: List of TAHOD Sites; Supplementary Data are available online at
We enrolled only patients for whom CD4 cell counts and clinical status records within 3 months of the first positive HIV test date were available. Patients were included if their first positive HIV test was recorded in the database between 2003 and March 2012. To minimize selection bias, we excluded patients who were HIV-positive before TAHOD began actively enrolling patients in 2003.
Variables and definitions
The following data were included in the analyses: age at first positive HIV test, sex, year of first positive HIV test, CD4 cell count (cells/μl), HIV viral load (copies/ml), Centers for Disease Control and Prevention (CDC) stage at presentation, reported HIV infection route, and hepatitis serologies.
The exposure of interest was defined as the year of the first HIV-positive test. The primary endpoint was late presentation at the time of entering into care. Late presentation was defined as a CD4 cell count <200 cells/μl or an AIDS-defining event (CDC Category C) within 3 months of the first positive test.
Statistical analysis
To evaluate the factors associated with late presentation, we performed logistic regression analyses with random effect on site, to adjust for potential clustering within each site. We performed a sensitivity analysis to determine the site-level effect on late presentation by including the World Bank income categories in the fixed-effect logistic model. 15 Significant factors (p < 0.10) in the univariate model were included in the multivariate model. Using a backward stepwise selection process, factors significant at p < 0.05 were adjusted for in the final multivariate model. Descriptive statistics for the categorical variables were analyzed using the chi-squared or Fisher's exact test, and continuous variables were analyzed using the Wilcoxon rank-sum test. The analyses were performed using SAS (version 9.3; SAS Institute Inc., Cary, NC) and STATA (version 12.1; StataCorp, College Station, TX).
Results
A total of 5,415 patients in TAHOD were recorded as having their first positive HIV test between 2003 and 2012. To analyze late presentation into care, 3,744 patients were included in the study; patients with no AIDS diagnosis and no CD4 measurements available within ±3 months of their first positive HIV test were excluded.
Table 1 summarizes the characteristics of patients with early or late presentation at first positive HIV test. Of the 3,744 patients, 2,681 (72%) were late presenters. Approximately 72% were male, 38% were aged 31–40 years, and 64% were exposed to HIV via heterosexual contact.
Excluding not tested or missing values.
Includes those exposed to blood products and unknown exposures.
Late presentation was defined as a CD4 cell count <200 cells/μl or an AIDS-defining event (CDC Category C) within 3 months of the first positive test.
IQR, interquartile range
Table 2 lists the factors associated with late presentation after adjusting for site clustering. The year of the first positive test, as illustrated in Fig. 1, was not associated with late presentation. The following factors were independently associated with late presentation into care according to the multivariate regression analysis: older age [31–40 years: odds ratio (OR) = 1.57, 95% confidence interval (CI) 1.31–1.88; 41–50 years: OR = 2.01, 95% CI 1.58–2.56; and ≥51 years: OR = 1.69, 95% CI 1.23–2.31 compared to the age less than 30 years old, all p ≤ 0.001] and the injecting drug user (IDU) HIV exposure category (OR = 2.15 versus heterosexual contact, 95% CI: 1.42–3.27; p < 0.001). In contrast, homosexual HIV exposure had an odds reduction of 55% for late presentation (OR = 0.45, 95% CI: 0.35–0.58; p < 0.001). Female sex was also found to be a protective factor (OR = 0.44 versus the male sex, 95% CI: 0.36–0.53; p < 0.001).

Proportion of late presenters at first positive test.
Global p-values indicate tests for heterogeneity, excluding untested or missing values.
Includes those exposed to blood products and unknown exposures.
p-values in bold represent significant covariates in the final model. Nonsignificant factors are presented in the significant predictor adjusted multivariate model. Late presentation was defined as a CD4 cell count <200 cells/μl or an AIDS-defining event (CDC Category C) within 3 months of the first positive test.
CI, confidence interval; OR, odds ratio.
We included the country income level variable in the sensitivity analysis as a fixed covariate to determine whether there was a site-level association with late presentation. There was one site categorized as “low” income, seven sites as “lower-middle,” nine sites as “upper-middle,” and six sites as “high.” The categories were combined further into “low + lower-middle income” and “upper-middle + high income.” After adjusting for country income in the univariate model, we found no association between “upper middle + high income” countries compared with “low + lower-middle income” countries in the association with late presentation (OR = 1.07, 95% CI 0.93–1.23; p = 0.375).
Figure 2 presents a graph of the median time to ART initiation according to the year in which the first positive HIV test was obtained. A total of 3,429 patients who had begun receiving ART were included. Patients who satisfied the definition of late presentation began receiving ART relatively soon after the first HIV-positive test. Previously, the median time to treatment initiation among early presenters was much longer, as those who presented early in 2003 had a median time to treatment of 2.19 years (interquartile range 0.40–4.57) vs. a median of 0.35 years (interquartile range 0.14–1.14, p < 0.001) for those who presented in 2008, the time period in which the sharpest decline was observed. When the early and late presenters were compared, the early presenters in 2003 had a significantly longer time to ART initiation (2.19 years vs. 0.15 years, p < 0.001); this difference remained significant in 2008 (0.35 years vs. 0.14 years, p < 0.001). Beginning in 2011, the time to ART initiation was similar in both groups (2011: 0.11 years vs. 0.09 years; p = 0.233, and 2012: 0.06 years vs. 0.06 years; p = 0.364). It is important to note that only 25 patients were included in 2012 because of our analysis cut-off date of March 2012.
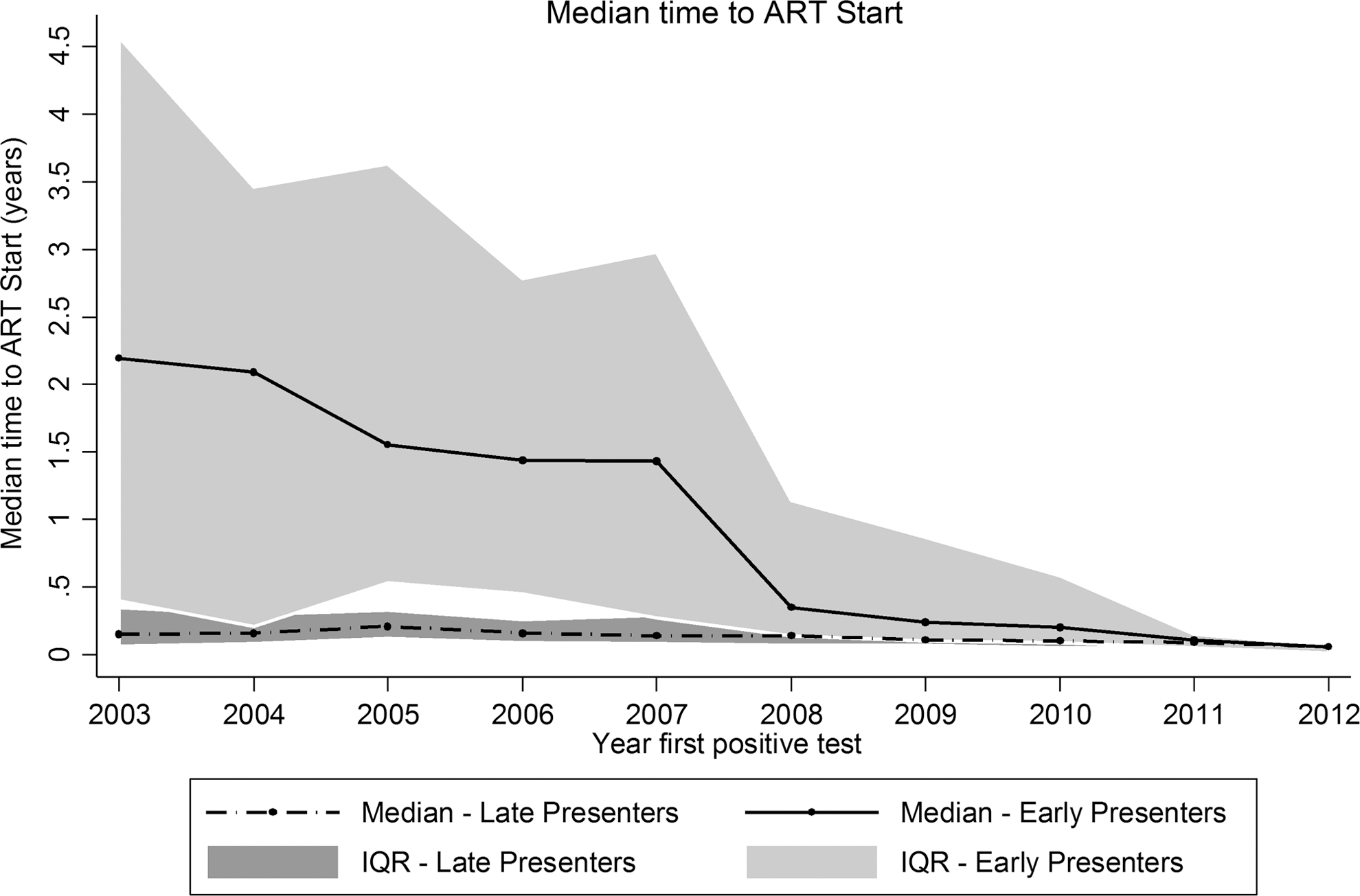
The median time to antiretroviral therapy (ART) initiation in HIV-infected patients. Late presenter was defined as an HIV-infected patient with CD4 cell count <200 cells/μl or an AIDS-defining event (CDC Category C) within 3 months of the first positive test.
Discussion
ART has significantly changed the natural history of HIV infection and has led to great reductions in morbidity and mortality in HIV-infected patients. 16 However, more than one-third of patients with HIV infection in Europe receive late diagnoses 17 and in the North America AIDS Cohort Collaboration (NA-ACCORD), the CD4 counts at first presentation have increased since 1997, although the proportion of patients who presented with CD4 counts <350 cells/μl remained 54% in 2007. 18 In the International Epidemiologic Databases to Evaluate AIDS (IeDEA) global consortium, the baseline CD4 counts across four regions in sub-Saharan Africa ranged from 126 to 211 cells/μl among patients presenting for care. 19 Therefore, the prevalence of late presentation to care did not decrease worldwide over time even after the introduction of ART.
To our knowledge, this is the first regional report from the Asia-Pacific to examine the prevalence and risk factors of late presentation to care. In this study, we found that 72% of the patients presented late. It is difficult to compare the prevalence rates in earlier studies because a standardized definition of late presentation was not yet applied. After allowing for different definitions, the present study reported a greater proportion of HIV patients with late presentation than most of the other studies. Even after the introduction of ART, 55% of newly diagnosed patients were symptomatic at baseline ranging from a low of 39% in the first half of 1994 to a high of 71% in the second half of 1998 at a clinic in the United States. 20 In a province of Thailand, 55% of the patients who received initial HIV diagnoses from 2004 to 2005 presented with HIV-related symptoms at diagnosis. 21 Several studies reported that the late presentation for care observed in developing regions such as sub-Saharan Africa, Southeast Asia, and South America was due to limited health care access and health literacy. 22,23
The median time to starting ART after a new HIV diagnosis has been reduced and, in more recent years, a trend toward early ART initiation after HIV diagnosis has been observed among both early and late presenters, notably after the changes in the CD4 thresholds for ART initiation in international guidelines. 24 However, despite having a mix of low- to high-income countries, patients in this cohort continue to have a high rate of late presentation into care, which presents a barrier to early ART. Early HIV diagnosis and retention in HIV care represent an important opportunity for achieving earlier access to treatment and reducing the risk of transmission. 25 Late presentation into care and consequent delays in ART initiation are associated with more HIV-related, opportunistic infections, increased morbidity and mortality, diminished responses to ART, and health care expenditures. 9,26,27 Therefore, the reduction of late presentation into care should be a top HIV care priority in this region.
In the multivariate analysis, older age, male sex, and IDU were significant risk factors for late presentation into care. This finding suggests a lower risk perception in these populations and implies an insufficient level of HIV testing. Older age (≥30 years) was associated with increased risk of late presentation, and this result corresponds to the findings of previous studies. 28,29 Late-diagnosed patients would be expected to be older than patients diagnosed for other reasons because HIV-related symptoms usually develop after a prolonged period of infection at which point the immune system has been weakened. 30,31 In addition, a previous study reported that older patients were more likely to be diagnosed during hospitalization, and they suggested that these populations may have a lower perceived risk for HIV infection. 32
Late presentation was more common among men and was associated with IDU and heterosexual HIV exposure. These findings are consistent with those of other studies. Previous studies have reported the proportion of late diagnosis to be lower among men who have sex with men. 28,33 In addition, several previous reports identified IDU as a high-risk population for late diagnosis and care. 34,35 Females seem less likely to present late and this could be due to HIV testing during pregnancy. Furthermore, females get tested soon after their spouse test HIV positive, thereby discovering the virus at a much earlier stage of infection that their partners.
There are several limitations to this study. TAHOD data were collected from urban referral centers, which are more likely to receive referrals of sicker patients with advanced immune deficiency. Therefore, TAHOD participants are not necessarily representative of all HIV-infected patients in Asian countries, and therefore our results might not be fully generalizable. We could not analyze the impact of socioeconomic factors on late presentation as those data were not available. In addition, retrospective patient information collection in resource-limited settings remains a challenge.
In the past decade, 72% of the HIV patients in TAHOD who entered care were late presenters. Patients who present late to HIV care are often ill, have a high early mortality risk, are less likely to respond to ART, and have an increased forward HIV transmission risk. In order to achieve earlier entry into care, HIV testing programs, including provision of medical support involving HIV testing services for elderly populations with poor access to health care or regular check-up in IDU, must ensure the inclusion of those at highest risk of having HIV and of those missed by traditional HIV outreach programs. Region-specific efforts to facilitate early diagnosis should be implemented.
Footnotes
Acknowledgments
The study team would like to acknowledge TAHOD-TASER study members, steering committee, and patients for their support.
TAHOD-TASER study members: • A Kamarulzaman, SF Syed Omar, S Ponnampalavanar, I Azwa, N Huda, and LY Ong, University Malaya Medical Centre, Kuala Lumpur, Malaysia; • BLH Sim, YM Gani, and R David, Hospital Sungai Buloh, Sungai Buloh, Malaysia; • CV Mean, V Saphonn, and V Khol, National Center for HIV/AIDS, Dermatology and STDs, Phnom Penh, Cambodia; • E Yunihastuti,
†
D Imran, and A Widhani, Working Group on AIDS Faculty of Medicine, University of Indonesia/Cipto Mangunkusumo Hospital, Jakarta, Indonesia; • FJ Zhang, HX Zhao, and N Han, Beijing Ditan Hospital, Capital Medical University, Beijing, China; • JY Choi, Na S, and JM Kim, Division of Infectious Diseases, Department of Internal Medicine, Yonsei University College of Medicine, Seoul, South Korea; • M Mustafa, and N Nordin, Hospital Raja Perempuan Zainab II, Kota Bharu, Malaysia; • N Kumarasamy, S Saghayam, and C Ezhilarasi, YRGCARE Medical Centre, VHS, Chennai, India; • OT Ng, PL Lim, LS Lee, and PS Ohnmar, Tan Tock Seng Hospital, Singapore; • MP Lee, PCK Li, W Lam, and YT Chan, Queen Elizabeth Hospital and KH Wong, Integrated Treatment Centre, Hong Kong, China; • P Kantipong and P Kambua, Chiangrai Prachanukroh Hospital, Chiang Rai, Thailand; • P Phanuphak, K Ruxrungtham, A Avihingsanon, P Chusut, and S Sirivichayakul, HIV-NAT/Thai Red Cross AIDS Research Centre, Bangkok, Thailand; • R Ditangco,
†
E Uy, and R Bantique, Research Institute for Tropical Medicine, Manila, Philippines; • R Kantor, Brown University, Rhode Island, United States; • S Oka, J Tanuma, and T Nishijima, National Center for Global Health and Medicine, Tokyo, Japan; • S Pujari, K Joshi, and A Makane, Institute of Infectious Diseases, Pune, India; • S Kiertiburanakul, S Sungkanuparph, L Chumla, and N Sanmeema, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand; • TP Merati,
‡
DN Wirawan, and F Yuliana, Faculty of Medicine, Udayana University and Sanglah Hospital, Bali, Indonesia; • R Chaiwarith, T Sirisanthana, W Kotarathititum, and J Praparattanapan, Research Institute for Health Sciences, Chiang Mai University, Chiang Mai, Thailand; • TT Pham, DD Cuong, and HL Ha, Bach Mai Hospital, Hanoi, Vietnam; • VK Nguyen, VH Bui, and TT Cao, National Hospital for Tropical Diseases, Hanoi, Vietnam; • W Ratanasuwan and R Sriondee, Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok, Thailand; • WW Wong, WW Ku, and PC Wu, Taipei Veterans General Hospital, Taipei, Taiwan; • YMA Chen and YT Lin, Kaohsiung Medical University, Kaohsiung City, Taiwan; • AH Sohn, N Durier, B Petersen, and T Singtoroj, TREAT Asia, amfAR—The Foundation for AIDS Research, Bangkok, Thailand; • DA Cooper, MG Law, A Jiamsakul, and DC Boettiger, The Kirby Institute, UNSW Australia, Sydney, Australia.
The TREAT Asia HIV Observational Database, TREAT Asia Studies to Evaluate Resistance, and the Australian HIV Observational Database are initiatives of TREAT Asia, a program of amfAR, The Foundation for AIDS Research, with support from the Dutch Ministry of Foreign Affairs through a partnership with Stichting Aids Fonds, and the U.S. National Institutes of Health's National Institute of Allergy and Infectious Diseases, Eunice Kennedy Shriver National Institute of Child Health and Human Development, and National Cancer Institute, as part of the International Epidemiologic Databases to Evaluate AIDS (IeDEA; U01AI069907). Queen Elizabeth Hospital and the Integrated Treatment Centre received additional support from the Hong Kong Council for AIDS Trust Fund. The Kirby Institute is funded by the Australian Government Department of Health and Ageing, and is affiliated with the Faculty of Medicine, UNSW Australia (The University of New South Wales). J.Y.C.'s involvement was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education, Science and Technology (NRF-2013R1A1A2005412), a grant from Chronic Infectious Disease Cohort (4800-4859-304-260) from Korea Centers for Disease Control and Prevention, and BioNano Health-Guard Research Center funded by the Ministry of Science, ICT & Future Planning (MSIP) of Korea as Global Frontier Project (H-GUARD_2013M3A6B2078953). The content of this publication is solely the responsibility of the authors and does not necessarily represent the official views of any of the governments or institutions mentioned above.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.